
Abstract
Purpose
The purpose of the study was to evaluate the efficacy and safety of tirofiban use in endovascular thrombectomy for intravenous thrombolysis applicable patients of large vessel occlusion stroke with data from Direct-MT trial.
Materials and Methods
Direct-MT was the first randomized controlled trial to prove the non-inferiority of thrombectomy alone to bridging therapy (intravenous thrombolysis before thrombectomy) for large vessel occlusion stroke. Patients who underwent endovascular procedure were included and divided into thrombectomy-alone group and bridging therapy group. The effect of tirofiban use on 90 days MRS distribution, MRS 0–2 and mortality, successful reperfusion, the ASPECTS and outcome lesion volume of index stroke, re-occlusion of the treated vessel, futile recanalization and safety outcomes were further evaluated in both groups after adjustment for relevant confounding factors. The interaction between tirofiban and rt-PA was also assessed.
Results
Of 639 patients included in this analysis, 180 patients underwent thrombectomy with tirofiban use (28.2%). Patients with tirofiban use had lower percentage of bridging therapy (41.1% vs 54.3%, P = 0.003), higher proportion of large artery atherosclerosis (P < 0.001) and more emergent stenting (30.56% vs 6.97%, P < 0.001). After adjustment for confounding factors, the 90-day modified Rankin Scale distribution, successful final recanalization rate, outcome lesion volume of index stroke on CT and intracranial hemorrhage risk showed no difference after tirofiban use in thrombectomy-alone group and in bridging therapy group. No interaction effect between tirofiban and rt-PA was detected.
Conclusion
Based on data from Direct-MT trial, tirofiban is a safe medication for intravenous thrombolysis applicable patients with large vessel occlusion stroke undergoing thrombectomy.
Level of Evidence
Level 3, cohort study of randomized trial.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Tirofiban, a non-peptide selective glycoprotein IIb/IIIa receptor inhibitor, can inhibit fibrinogen-dependent platelet aggregation and subsequent thrombosis [1]. It has been routinely applied in percutaneous coronary intervention for prevention of recurrent myocardial infarction and ischemic complications before its wide application in neurointervention [2, 3]. Tirofiban inhibits platelet aggregation in a dose-dependent manner and exerts the antiplatelet effect from 30 min after loading dose, with normalization of platelet function within no more than 4 h after treatment stop [4].
Tirofiban has been gradually accepted as an adjunctive therapy to thrombectomy for emergent large vessel occlusion (LVO) stroke, although its general efficacy and safety remained controversial [5,6,7,8]. In cases of intracranial atherosclerotic stenosis (ICAS)-related LVO stroke, tirofiban is effective and well-tolerated [9]. On the other hand, tirofiban, as an antiplatelet agent, can theoretically increase hemorrhagic risk after rt-PA infusion. However, tirofiban administration was reported for no increase in the occurrence of intracranial hemorrhage after intravenous thrombolysis (IVT) [10, 11]. The safety of tirofiban administration after IVT in stroke patients undergoing endovascular thrombectomy (EVT) is still indecisive. Meanwhile, with the progress of thrombectomy techniques, the successful recanalization rate has reached to over 80%, whether the tirofiban use might further improve the efficacy of thrombectomy is unclear.
Recently, the Endovascular Treatment With vs Without Tirofiban for Patients with Large Vessel Occlusion Stroke (RESCUE BT) trial revealed no difference in the 90 days modified Rankin Scale (MRS) distribution between two groups, but suggested a possible benefit of tirofiban use in the large artery atherosclerosis (LAA) subgroup [12]. The RESCUE BT trial enrolled patients undergoing EVT between 4.5 h and 24 h after symptoms onset, and patients with IVT were excluded. The question for the efficacy and safety of tirofiban use in IVT applicable patients was not answered by the RESCUE BT trial.
The Direct-MT trial was the first randomized controlled trial to prove the non-inferiority of thrombectomy alone to bridging therapy (intravenous thrombolysis before thrombectomy) for emergent LVO stroke of anterior circulation in endovascular treatment capable centers [13]. Patients within 4.5 h after stroke symptom onset were enrolled and assigned to thrombectomy-alone group or bridging therapy group randomly. In such a context, the effect of tirofiban use can be critically evaluated in thrombectomy-alone patients and in bridging therapy patients with comparable baseline data. This post hoc analysis aimed to provide reference to the efficacy and safety of tirofiban use in thrombectomy for emergent LVO stroke of IVT applicable patients.
Material and Methods
Patient Selection
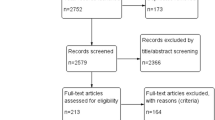
The data of this study are available from the corresponding author upon reasonable request. Patient eligibility and the protocol of the Direct-MT trial (NCT03469206) have been reported previously [14]. There were 1586 patients screened for eligibility and 656 patients randomized. Of 656 patients, 327 patients allocated to the thrombectomy-alone group and 329 patients to the bridging therapy (intravenous thrombolysis before thrombectomy) group. After that, 11 patients in the thrombectomy-alone group and six in the bridging therapy group were excluded because of not undergoing catheter angiography. Finally, a total of 639 patients, with 316 in the thrombectomy-alone group and 323 in the bridging therapy group, were included in this post hoc analysis. This study was approved by all relevant local ethics committees and research boards. Written informed consent was obtained from all the patients or their legal representatives.
Tirofiban Use
Tirofiban use was defined as periprocedural intravenous with or without intra-arterial use of the tirofiban if, (1) emergent stent angioplasty was unavoidable, and (2) vessel re-occlusion occurred or was expected after successful recanalization. The expected re-occlusion after successful recanalization indicated the antegrade flow in the treated vessel got deterioration after successful recanalization which was detected at any single run before the end of procedure. For tirofiban use, the loading dose was 0.1–0.4 ug/(kg min) for 30 min by intravenous infusion or combined with intra-arterial infusion, or 3-12 ug/kg intravenous bolus dose, then followed with intravenous maintenance dose of 0.1 ug/(kg min). Oral dual antiplatelets were prescribed for stenting patients after 24 h from IVT with the exclusion of intracranial hemorrhage by CT and overlapped with intravenous tirofiban for 6 h. For patients without stenting, single antiplatelet was prescribed in the same manner.
Radiographic Variables Assessment
The location of occlusion was evaluated on baseline pre-procedure CTA and classified as ICA, M1 and M2 by the core laboratory. The extent of thrombus was quantified using the clot burden score [15]. The collateral grading system was scored on a 4-point scale of 0–3 and dichotomized into grades 0–1 and grades 2–3 [16].
Primary and Secondary Outcomes
The primary outcome was 90 days MRS distribution shift. The secondary outcomes included good clinical outcome and mortality at 90 days, rates of successful reperfusion on final angiogram, the Alberta Stroke Program Early Computed Tomography score (ASPECTS) and outcome lesion volume of index stroke on follow-up CT, re-occlusion rate of the treated vessel on follow-up CTA and futile recanalization rate. The good clinical outcome was defined as MRS 0–2 at 90 days. Mortality was defined as MRS 6 at 90 days. Successful reperfusion was defined as final extended thrombolysis in cerebral ischemia (eTICI) 2b, 2c or 3 [17]. The outcome lesion volume was assessed on follow-up CT on days 5–7 using an automated algorithm [18]. Re-occlusion was defined as the total occlusion on follow-up CTA of the treated vessel (final eTICI > 0). Futile recanalization was defined as 90 days MRS > 2 despite a successful reperfusion (final eTICI ≥ 2b) [19,20,21].
Safety Outcomes
Safety outcomes included rates of symptomatic intracranial hemorrhage (sICH), any ICH, large or malignant middle cerebral artery (MCA) infarction, infarctions in new territory at 5–7 days and femoral access complications. The sICH was defined according to the Heidelberg criteria [22].
Statistical Analysis
Categorical variables were expressed as frequencies and percentages, continuous as mean (SD, standard deviation) for normal distribution or median (IQR, interquartile range) for non-normal distribution. Missing data were imputed with the use of multiple imputation by fully conditional specification regression for continuous variables or by fully conditional specification logistic regression for binary and ordinal variables. Categorical variables were tested using the Chi-square test. Continuous variables with normal distribution were tested using the t-test. Continuous variables with non-normal distribution were tested using the rank-sum test. Non-parametric testing of categorical variables was tested using Fisher’s exact test. Multivariable logistic regression analysis was applied to estimate the adjusted odds ratio (OR) for a shift in direction toward better outcome for with tirofiban vs without tirofiban in thrombectomy-alone group and bridging therapy group after adjustment for confounding factors. Confounding factors included age, sex, cause of stroke, the National Institutes of Health Stroke Scale (NIHSS) score at baseline, the time from stroke onset to randomization, the MRS score before stroke onset, cerebral collateral blood flow status, history of antiplatelet agents and emergent stenting. Adjusted OR was reported with 95% confidence interval (CI). The interaction between tirofiban and rt-PA was also evaluated after adjustment for confounding factors. Statistical testing was conducted at a two-tailed α level of 0.05. All the analyses were performed using the SAS software, version 9.2 (SAS Institute).
Results
Baseline and Clinical Data of Patients With/Without Tirofiban in Direct-MT Trial
Overall, there were 639 patients included in this post hoc analysis. The flow diagram for patient selection is presented in Fig. 1. Among 639 patients, there were 180 (28.2%) patients with tirofiban use. Patients with tirofiban use were younger and more male sex. Lower percentage of bridging therapy (41.1% vs 54.3%, P = 0.003) and history of antiplatelet agents use (8.33% vs 16.1%, P = 0.011) were observed with tirofiban use. Difference in cause of stroke was detected, as more intracranial atherosclerosis and more ipsilateral extracranial ICA obstruction in patients with tirofiban use (P < 0.001). There was also more stenting in patients with tirofiban use (30.6% vs 6.97%, P < 0.001). Baseline data are presented in Table 1.

The flow diagram for patient selection
Primary and Secondary Outcomes
After being adjusted for age, sex, cause of stroke, the NIHSS score at baseline, the time from stroke onset to randomization, the MRS score before stroke onset, cerebral collateral blood flow status, history of antiplatelet agents and emergent stenting, tirofiban use showed no benefit in primary outcome of 90 days MRS distribution shift and in secondary outcomes of 90 days MRS 0–2, 90 days mortality, successful reperfusion rate, follow-up ASPECTS, outcome lesion volume of index stroke, re-occlusion rate of the treated vessel and futile recanalization rate in thrombectomy-alone group and in bridging therapy group. No interaction was detected between tirofiban and rt-PA considering the primary and secondary outcomes.
Safety Outcomes
Tirofiban use had no influence on the risk of sICH and any ICH in thrombectomy-alone group and in bridging therapy group. There was no interaction effect between tirofiban and rt-PA for ICH occurrence. No deterioration was detected in other safety outcomes. Relevant data are presented in Tables 2 and 3.
Discussion
Taking LVO stroke patients as a whole group, the efficacy and safety of tirofiban use in thrombectomy remained controversial. An observational study based on a single-center prospective registry study in China showed that tirofiban was not associated with higher sICH and leads to lower odds of deaths and better odds of long-term functional independence [23]. A multicenter registry from Korea revealed the safety of tirofiban use during endovascular therapy after IVT but failed to prove its efficacy [24]. In our study, tirofiban use showed no improvement in 90 days MRS distribution in LVO stroke patients undertaking thrombectomy with or without IVT. Also, it failed to bring benefit in successful recanalization rate enhancement and final infarct volume reduction. In Direct-MT trial, general successful recanalization rate reached at the level of 80%. If tirofiban brought potential contributions to the improvements in recanalization rate, it is really hard to be recognized with significance. Recently, a meta-analysis indicated that the use of tirofiban during IVT bridging thrombectomy might reduce the risk of re-occlusion of the treated vessel and 90 days mortality without increasing the risk of sICH and any ICH [25]. But no difference in re-occlusion rate after tirofiban use was detected in thrombectomy-alone group or in bridging therapy group according to our study. Given that we had adjusted confounding factors, such as the cause of stroke and emergent stenting, the additional benefit of tirofiban use in terms of preventing vessel re-occlusion other than in cases of LAA-related LVOs and of stent angioplasty was not claimed.
Several large-scale studies have investigated the efficacy and safety of tirofiban use in EVT for LVOs of LAA etiology. In a multicenter prospective study, 649 patients with LAA stroke were enrolled to evaluate the efficacy and safety of tirofiban use. Tirofiban was found to be associated with superior clinical outcomes in anterior circulation stroke and major stroke (NIHSS > 5) patients but with no cerebral hemorrhage increase [26]. In another study with 503 patients of LVOs retrospectively examined, intravenous tirofiban was associated with high recanalization rate and good outcome in both the whole cohort and the LAA subgroup [27]. Intravenous tirofiban infusion can also decrease the risk of early re-occlusion of the treated arteries with no increased risk of hemorrhage after angioplasty and stenting in ICAS-related LVOs [28].
As for the safety outcome, this post hoc analysis proved that tirofiban use increased ICH risk in neither group. No interaction effect existed between tirofiban and rt-PA. These results are consistent with the findings of a meta-analysis which included 722 patients with IVT bridging therapy from three trials, and 846 patients with IVT alone from seven studies published between 2001 and 2021. Pooled results showed that early tirofiban administration with IVT or bridging therapy did not increase the risks of sICH and ICH [29]. However, it was demonstrated that tirofiban, as an adjunct to thrombectomy, increased fatal bleeding risk in a dose-dependent manner [30]. In another nonrandomized study, tirofiban treatment increased risk of major ICH after endovascular thrombectomy, which might be the consequence of the sole intra-arterial administration of tirofiban [31]. Later, sole intra-arterial tirofiban was verified the association with higher hemorrhage rate and death rate as an adjunct to EVT [27]. In RESCUE BT trial, tirofiban was prescribed in a “routine” manner before EVT instead of in a flexible manner. Although no significant difference in the incidence of sICH between two groups (numerically higher for tirofiban group), the incidence of any ICH was increased in the tirofiban group [12]. In real-world practice, several noteworthy factors might influence the risk of cerebral hemorrhage after adjunctive tirofiban use during EVT. The first one is the actual time window of endovascular reperfusion. The hemorrhage risk increases with time period from symptom onset to reperfusion [32]. The second one is the severity of stroke, as the higher baseline NIHSS score can predict sICH risk after EVT independently [33]. The third one is the route and dosage of tirofiban use, which for now still lack consensus. In Direct-MT trial, the time period from symptom onset to reperfusion was strictly controlled, and tirofiban was administrated based on specific demand at a relatively low dosage level and mainly by transvenous route. Precise prescription of tirofiban in LVO stroke patients with acceptable hemorrhagic risk should be explored profoundly in the future.
Our study had several limitations. First, for now, neuro-interventionists still lack international guidelines for tirofiban use in the endovascular recanalization for LVOs. However, all of the operators from selected enrollment centers were of full experience in EVT, and the prescribed dosage of tirofiban in Direct-MT trial was within the range of the recommendations from 2019 Chinese expert consensus on clinical application of tirofiban in atherosclerotic cerebrovascular disease. Second, according to the design of Direct-MT trial, stent retriever was the primary device, and aspiration devices could be used as a secondary option if the initial reperfusion failed. This analysis, to some degree, represents the situation of tirofiban use in stent retrieval thrombectomy, in which the endothelial damages are regarded as unavoidable. Third, Direct-MT trial is a study based on Chinese population for whom the ICAS-related LVO is more common, but in western population, tirofiban is typically used in extracranial stenting evolved in tandem occlusion. The results of this analysis should not be generalized to all population. Fourth, given the nature of post hoc analysis, bias should be unavoidable. Well-designed prospective randomized controlled trials are needed to address this issue in the future. But we can still provide insight into the clinical practice and future research of tirofiban use in thrombectomy for IVT applicable patients with emergent LVO stroke.
Conclusion
Based on data from Direct-MT trial, tirofiban is a safe medication for IVT applicable patients with LVO stroke undergoing thrombectomy. However, no matter with or without IVT, tirofiban use showed no benefits in achieving favorable outcomes.
Abbreviations
- LVO :
-
Large vessel occlusion
- ICAS :
-
Intracranial atherosclerotic stenosis
- IVT :
-
Intravenous thrombolysis
- EVT :
-
Endovascular thrombectomy
- NIHSS :
-
National Institutes of Health Stroke Scale
- MRS :
-
Modified Rankin Scale
- ASPECTS :
-
Alberta Stroke Program Early Computed Tomography score
- eTICI :
-
Extended thrombolysis in cerebral ischemia
- sICH :
-
Symptomatic intracranial hemorrhage
- LAA :
-
Large artery atherosclerosis
References
McClellan KJ, Goa KL. Tirofiban: a review of its use in acute coronary syndromes. Drugs. 1998;56(6):1067.
Braunwald E, et al. Rationale and clinical evidence for the use of GP IIb/IIIa inhibitors in acute coronary syndromes. Eur Heart J. 1998;19:D22-30.
van’t Hof AW, Valgimigli M. Defining the role of platelet glycoprotein receptor inhibitors in STEMI: focus on tirofiban. Drugs. 2009;69(1):85–100.
Harder S, Klinkhardt U, Alvarez JM. Avoidance of bleeding during surgery in patients receiving anticoagulant and/or antiplatelet therapy: pharmacokinetic and pharmacodynamic considerations. Clin Pharmacokinet. 2004;43(14):963–81.
Zhang P, et al. Efficacy and safety of tirofiban therapy in patients receiving endovascular treatment after large vessel ischaemic stroke: a systematic review and meta-analysis. J Clin Neurosci. 2020;80:112–20.
Gong J, et al. Tirofiban for acute ischemic stroke: systematic review and meta-analysis. Eur J Clin Pharmacol. 2020;76(4):475–81.
Sun Y, et al. Safety and efficacy of tirofiban combined with endovascular therapy compared with endovascular therapy alone in acute ischemic stroke: a meta-analysis. Neuroradiology. 2021;63(1):17–25.
Zhang A, et al. Continuous intravenous tirofiban can improve the 90-day functional outcome and decrease 90-day mortality without increasing bleeding risk in acute ischemic stroke patients treated by endovascular therapy: a meta-analysis. J Clin Neurosci. 2022;99:109–16.
Sang H, et al. Association of tirofiban with functional outcomes after thrombectomy in acute ischemic stroke due to intracranial atherosclerotic disease. Neurology. 2023;100(19):e1996–2006.
Siebler M, et al. Safety of tirofiban in acute Ischemic Stroke: the SaTIS trial. Stroke. 2011;42(9):2388–92.
Seitz RJ, et al. Thrombolysis with recombinant tissue plasminogen activator and tirofiban in stroke: preliminary observations. Stroke. 2003;34(8):1932–5.
Investigators RBT, et al. Effect of intravenous tirofiban versus placebo before endovascular thrombectomy on functional outcomes in large vessel occlusion stroke: the rescue bt randomized clinical trial. JAMA. 2022;328(6):543–53.
Yang P, et al. Endovascular thrombectomy with or without intravenous alteplase in acute stroke. N Engl J Med. 2020;382(21):1981–93.
Yang P, et al. Direct Intra-arterial thrombectomy in order to Revascularize AIS patients with large vessel occlusion efficiently in Chinese tertiary hospitals: a multicenter randomized clinical trial (DIRECT-MT)-protocol. Int J Stroke. 2020;15(6):689–98.
Puetz V, et al. Intracranial thrombus extent predicts clinical outcome, final infarct size and hemorrhagic transformation in ischemic stroke: the clot burden score. Int J Stroke. 2008;3(4):230–6.
Tan IY, et al. CT angiography clot burden score and collateral score: correlation with clinical and radiologic outcomes in acute middle cerebral artery infarct. AJNR Am J Neuroradiol. 2009;30(3):525–31.
Goyal M, et al. 2C or not 2C: defining an improved revascularization grading scale and the need for standardization of angiography outcomes in stroke trials. J Neurointerv Surg. 2014;6(2):83–6.
Boers AM, et al. Automated cerebral infarct volume measurement in follow-up noncontrast CT scans of patients with acute ischemic stroke. AJNR Am J Neuroradiol. 2013;34(8):1522–7.
Molina CA. Futile recanalization in mechanical embolectomy trials: a call to improve selection of patients for revascularization. Stroke. 2010;41(5):842–3.
Baek JH, et al. Number of stent retriever passes associated with futile recanalization in acute stroke. Stroke. 2018;49(9):2088–95.
Pedraza MI, et al. Brain atrophy and the risk of futile endovascular reperfusion in acute ischemic stroke. Stroke. 2020;51(5):1514–21.
von Kummer R, et al. The heidelberg bleeding classification: classification of bleeding events after ischemic stroke and reperfusion therapy. Stroke. 2015;46(10):2981–6.
Zhao W, et al. Low-dose tirofiban improves functional outcome in acute ischemic stroke patients treated with endovascular thrombectomy. Stroke. 2017;48(12):3289–94.
Jang SH, et al. The safety of intra-arterial tirofiban during endovascular therapy after intravenous thrombolysis. AJNR Am J Neuroradiol. 2021;42(9):1633–7.
Li W, et al. Safety and efficacy of tirofiban during intravenous thrombolysis bridging to mechanical thrombectomy for acute ischemic stroke patients: a meta-analysis. Front Neurol. 2022;13:851910.
Huo X, et al. Safety and efficacy of tirofiban for acute ischemic stroke patients with large artery atherosclerosis stroke etiology undergoing endovascular therapy. Front Neurol. 2021;12:630301.
Yang J, et al. Intraarterial versus intravenous tirofiban as an adjunct to endovascular thrombectomy for acute ischemic stroke. Stroke. 2020;51(10):2925–33.
Baek BH, et al. intravenous tirofiban infusion after angioplasty and stenting in intracranial atherosclerotic stenosis-related stroke. Stroke. 2021;52(5):1601–8.
Liu Q, et al. Early tirofiban administration for patients with acute ischemic stroke treated with intravenous thrombolysis or bridging therapy: Systematic review and meta-analysis. Clin Neurol Neurosurg. 2022;222:107449.
Kellert L, et al. Endovascular stroke therapy: tirofiban is associated with risk of fatal intracerebral hemorrhage and poor outcome. Stroke. 2013;44(5):1453–5.
Wu Y, et al. Endovascular thrombectomy. Stroke. 2018;49(11):2783–5.
Sun J, et al. Risk factors of hemorrhagic transformation in acute ischaemic stroke: a systematic review and meta-analysis. Front Neurol. 2023;14:1079205.
Tian B, et al. Clinical and imaging indicators of hemorrhagic transformation in acute ischemic stroke after endovascular thrombectomy. Stroke. 2022;53(5):1674–81.
Funding
This study was not supported by any funding.
Author information
Authors and Affiliations
Consortia
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Consent for Publication
For this type of study, consent for publication is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhang, Y., Zhang, P., Tao, A. et al. The Efficacy and Safety of Tirofiban Use in Endovascular Thrombectomy for Intravenous Thrombolysis Applicable Patients with Large Vessel Occlusion Stroke—a Post Hoc Analysis from the Direct-MT Trial. Cardiovasc Intervent Radiol 47, 208–215 (2024). https://doi.org/10.1007/s00270-023-03540-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-023-03540-9