
Abstract
Background
Gastric pneumatosis (GP) is a rare radiologic finding with an unpredictable prognosis. The aim of this study was to identify mortality risk factors from patients presenting with GP on computed tomography (CT), and to develop a model which would allow us to predict which patients would benefit most from operative management.
Methods
Between 2010 and 2020, all CT-scan reports in four tertiary centers were searched for the following terms: “gastric pneumatosis,” “intramural gastric air” or “emphysematous gastritis.” The retrieved CT scans were reviewed by a senior surgeon and a senior radiologist. Relevant clinical and laboratory data for these patients were extracted from the institutions’ medical records.
Results
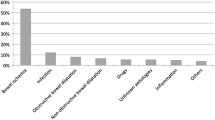
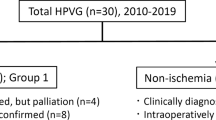
Among 58 patients with GP, portal venous gas and bowel ischemia were present on CT scan in 52 (90%) and 17 patients (29%), respectively. The 30-day mortality rate was 31%. Univariate analysis identified the following variables as predictive of mortality at the time of the diagnosis of GP: abdominal guarding, hemodynamic instability, arterial lactate level >2 mmol/l, and the absence of gastric dilatation. Multivariable analysis identified the following variables as independent predictors of mortality: arterial lactate level (OR: 1.39, 95% CI: 1.07–1.79) and the absence of gastric dilatation (OR: 0.07, 95% CI: 0.01–0.79). None of the patients presenting with a baseline lactate rate<2 mmol/l died within 30 days following diagnosis, and no more than 17 patients out of 58 had bowel ischemia (29%).
Conclusions
GP could be managed non-operatively, even in the presence of portal venous gas. However, patients with arterial lactate level>2 mmol/l, or the absence of gastric dilation should be surgically explored due to a non-negligible risk of mortality.


Similar content being viewed by others

References
Johnson PT, Horton KM, Edil BH et al (2011) Gastric pneumatosis: the role of CT in diagnosis and patient management. Emerg Radiol 18(1):65–73
Matsushima K, Won EJ, Tangel MR et al (2015) Emphysematous gastritis and gastric emphysema: similar radiographic findings, distinct clinical entities. World J Surg 39(4):1008–1017
Nemakayala DR, Rai MP, Rayamajhi S, et al (2018) Role of conservative management in emphysematous gastritis. BMJ Case Rep bcr2017222118
Cohen NS, Collins JN (2018) Gastric pneumatosis: Fatal or Benign? Am Surg 84(11):e485–e486
Mulgund A, Razeghi S, Poreddy S (2017) Gastric pneumatosis from isolated gastric calciphylaxis. ACG Case Rep J 19(4):e91
Watson A, Bul V, Staudacher J et al (2017) The predictors of mortality and secular changes in management strategies in emphysematous gastritis. Clin Res Hepatol Gastroenterol 41(1):e1–e7
Szuchmacher M, Bedford T, Sukharamwala P et al (2013) Is surgical intervention avoidable in cases of emphysematous gastritis? A case presentation and literature review. Int J Surg Case Rep 4(5):456–459
Pastor-Sifuentes FU, Moctezuma-Velázquez P, Aguilar-Frasco J (2020) Gastric pneumatosis: the spectrum of the disease. Rev Gastroenterol Mex (Engl Ed) 85(2):219–220
DeLong ER, DeLong DM, Clarke-Pearson DL (1988) Comparing the area under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 44:83745
Sunnapwar A, Ojili V, Katre R et al (2017) Multimodality imaging of adult gastric emergencies: a pictorial review. Indian J Radiol Imaging 27(1):13–22
Monneuse O, Pilleul F, Barth X et al (2007) Portal venous gas detected on computed tomography in emergency situations: surgery is still necessary. World J Surg 31(5):1065–1071
Abboud B, El Hachem J, Yazbeck T et al (2009) Hepatic portal venous gas: physiopathology, etiology, prognosis and treatment. World J Gastroenterol 15(29):3585–3590
Spektor M, Chernyak V, McCann TE et al (2014) Gastric pneumatosis: Laboratory and imaging findings associated with mortality in adults. Clin Radiol 69(11):e445–e449
Sharma A, Mukewar S, Chari ST et al (2017) Clinical features and outcomes of gastric ischemia. Dig Dis Sci 62(12):3550–3556
Clavien PA, Barkun J, de Oliveira ML et al (2009) The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg 250(2):187–196
Author information
Authors and Affiliations
Contributions
AE, GP, BLR and AF contributed to design of the work.NK, OM, JYM, PAF, SC, DP, BM, RG, NW contributed to acquisition and analysis of the work. CL contributed to interpretation of data. All authors have approved the submitted version (and any substantially modified version that involves the author's contribution to the study). All authors have agreed both to be personally accountable for the author's own contributions and ensured that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature abdominal.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests concerning this article.
Ethical approval
The authors declare that they comply with journal’s ethical policies. The anonymous data collection was supported by an ethical approval with ID IRBN702021/CHUSTE issued by the Institutional Review Board: IORG0007394.
Consent for publication
All patients signed consent for publication.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Epin, A., Passot, G., Christou, N. et al. Gastric Pneumatosis with Portal Venous Gas can be Treated Non-operatively: A Retrospective Multi-institutional Study. World J Surg 46, 784–790 (2022). https://doi.org/10.1007/s00268-021-06433-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-021-06433-5