
Abstract
Background
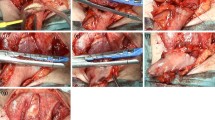
We herein report the feasibility and safety of cervical end-to-end anastomosis by the iTriangular stapling technique (iTST), which was developed as an extension of the triangular stapling technique (TST) after minimally invasive esophagectomy (MIE).
Methods
A total of 45 patients with thoracic esophageal cancer who underwent reconstruction with cervical esophagogastric anastomosis by iTST using a linear stapler after MIE between January 2016 and January 2019 were retrospectively reviewed. We modified and improved upon the TST by adding a 1- to 2-cm vertical incision on the anterior wall of the remnant esophageal stump to enlarge the anastomotic lumen and thereby reduce the risk of anastomotic stenosis. The short-term patient outcomes were determined to assess the safety and feasibility of our procedures.
Results
The median operating time was 686 (range, 319–1110) minutes, and the median blood loss was 170 (range, 5–1180) ml. There were no cases of anastomotic stenosis in this study, although 2 patients (4.4%) developed minor anastomotic leakage. A case (2.2%) of tracheal fistula due to the apex of the triangular anastomosis was resolved simply by delaying the patient’s oral intake. The mean length of the hospitalization was 21 days.
Conclusions
The iTST provides a larger lumen unlimited by the size of the esophagus in cervical esophagogastric anastomosis. This technique is feasible, and sufficient short-term results have been achieved. Further studies with the accumulation of more cases will be required to prove the benefits of iTST for reconstruction after MIE.


Similar content being viewed by others


References
Mamidanna R, Bottle A, Aylin P et al (2012) Short-term outcomes following open versus minimally invasive esophagectomy for cancer in England: a population-based national study. Ann Surg 255:197–203
Dewar L, Gelfand G, Finley RJ et al (1992) Factors affecting cervical anastomotic leak and stricture formation following esophagogastrectomy and gastric tube interposition. Am J Surg 163:484–489
Robertson GS, Lloyd DM, Wicks AC et al (1996) No obvious advantages for thoracoscopic two-stage oesophagectomy. Br J Surg 83:675–678
Valverde A, Hay JM, Fingerhut A et al (1996) Manual versus mechanical esophagogastric anastomosis after resection for car- cinoma: a controlled trial. French Assoc Surg Res Surg 120:476–483
Law S, Fok M, Chu KM et al (1997) Comparison of hand-sewn and stapled esophagogastric anastomosis after esophageal resection for cancer: a prospective randomized controlled trial. Ann Surg 226:169–173
Saluja SS, Ray S, Pal S et al (2012) Randomized trial comparing side-to-side stapled and hand-sewn esophagogastric anastomosis in neck. J Gastrointest Surg 16:1287–1295
Takeuchi H, Miyata H, Gotoh M et al (2014) A risk model for esophagectomy using data of 5354 patients included in a Japanese nationwide web-based database. Ann Surg 260:259–266
Haverkamp L, Van der Sluis PC, Verhage RJ et al (2013) End-to-end cervical esophagogastric anastomoses are associated with a higher number of strictures compared with end-to-side anastomoses. J Gastrointest Surg 17:872–876
Van Heijl M, Gooszen JA, Fockens P et al (2010) Risk factors for development of benign cervical strictures after esophagectomy. Ann Surg 251:1064–1069
Wong J, Cheung H, Lui R et al (1987) Esophago-gastric anastomosis performed with a stapler: the occurrence of leakage and stricture. Surgery 101:408–415
Honda M, Kuriyama A, Noma H et al (2013) Hand-sewn versus mechanical esophagogastric anastomosis after esophagectomy: a systematic review and meta-analysis. Ann Surg 257:238–248
Xu QR, Wang KN, Wang WP et al (2011) Linear stapled esophagogastrostomy is more effective than hand-sewn or circular stapler in prevention of anastomotic stricture: a comparative clinical study. J Gastrointest Surg 15:915–921
Nederlof N, Tilanus HW, Tran TC et al (2011) End-to-end versus end-to-side esophagogastrostomy after esophageal cancer resection: a prospective randomized study. Ann Surg 254:226–233
Venkatesh KS, Morrison N, Larson DM et al (1993) Triangulating stapling technique: an alternative approach to colorectal anastomosis. Dis Colon Rectum 36:73–76
Furukawa Y, Hanyu N, Hirai K et al (2005) Usefulness of automatic triangular anastomosis for esophageal cancer surgery using a linear stapler (TA-30). Ann Thorac Cardiovasc Surg 11:80–86
Toh Y, Sakaguchi Y, Ikeda O et al (2009) The triangulating stapling technique for cervical esophagogastric anastomosis after esophagectomy. Surg Today 393:201–206
Noshiro H, Urata M, Ikeda O et al (2013) Triangulating stapling technique for esophagogastrostomy after minimally invasive esophagectomy. Surgery 154:604–610
Deng XF, Liu QX, Zhou D et al (2015) Hand-sewn versus linearly stapled esophagogastric anastomosis for esophageal cancer: a meta-analysis. World J Gastroenterol 21:4757–4764
Nakata K, Nagai E, Ohuchida K et al (2015) Outcomes of cervical end-to-side triangulating esophagogastric anastomosis with minimally invasive esophagectomy. World J Surg 39:1099–1104
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications. A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–13
Kimura M, Kuwabara Y, Ishiguro H et al (2014) A new technique for shaping the gastric tube, using both radial and linear staplers. J Am Coll Surg 219:e15–e18
Sugimachi K, Ikeda M, Kai H et al (1982) Assessment of the blood flow in various gastric tubes for esophageal substitutes. J Surg Res 33:463–468
Lee Y, Fujita H, Yamana H et al (1994) Factors affecting leakage following esophageal anastomosis. Surg Today 24:24–29
Okuyama M, Motoyama S, Suzuki H et al (2007) Hand-sewn cervical anastomosis versus stapled intrathoracic anastomosis after esophagectomy for middle or lower thoracic esophageal cancer: a prospective randomized controlled study. Surg Today 37:947–952
Sarela AI, Tolan DJ, Harris K et al (2008) Anastomotic leakage after esophagectomy for cancer: a mortality-free experience. J Am Coll Surg 206:516–523
Beitler AL, Urschel JD (1998) Comparison of stapled and hand-sewn esophagogastric anastomoses. Am J Surg 175:337–340
Collard JM, Romagnoli R, Goncette L et al (1998) Terminalized semimechanical side-to-side suture technique for cervical esophagogastrostomy. Ann Thorac Surg 65:814–817
Ercan S, Rice TW, Murthy SC et al (2005) Does esophagogastric anastomotic technique influence the outcome of patients with esophageal cancer? Thorac Cardiovasc Surg 129:623–631
Orringer MB, Marshall B, Iannettoni MD et al (2000) Eliminating the cervical esophagogastric anastomotic leak with a side-to-side stapled anastomosis. Cardiovasc Surg 119:277–288
Ishibashi Y, Fukunaga T, Mikami S et al (2018) Triple-stapled quadrilateral anastomosis: a new technique for creation of an esophagogastric anastomosis. Esophagus 15:88–94
Dai JG, Zhang ZY, Min JX et al (2011) Wrapping of the omental pedicle flap around esophagogastric anastomosis after esophagectomy for esophageal cancer. Surgery 149:404–410
Yoshida N, Baba Y, Watanabe M et al (2015) Triangulating stapling technique covered with the pedicled omental flap for esophago-gastric anastomosis: a safe anastomosis with fewer complications. J Am Coll Surg 220:e13–e16
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest or financial ties to disclose. All procedures were conducted in accordance with the ethical standards of the respective committees on human experimentation (institutional and national) and with the 1964 Declaration of Helsinki and later versions. This study was approved by the Ethics Committee of University of Occupational and Environmental Health, Kitakyushu, Japan.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Shibao, K., Inoue, Y., Sawatsubashi, Y. et al. iTriangular Stapling Technique: A Novel Reconstruction Method and Clinical Outcomes of Cervical Esophagogastric Anastomosis after Esophagectomy. World J Surg 45, 1828–1834 (2021). https://doi.org/10.1007/s00268-021-05997-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-021-05997-6