
Abstract
Background
Anastomotic leakage after rectal resection represents a severe complication for the patient and requires an early and appropriate management. Endoscopic vacuum therapy (EVT) has become the treatment of choice for anastomotic leakage after rectal resection in several institutions in Germany, and commercially available systems are currently distributed in approximately 30 countries worldwide. However, there is no evidence that EVT is superior to any other treatment for anastomotic leakage after rectal resection.
Methods
Twenty-one patients treated with EVT for anastomotic leakage after rectal resection were retrospectively compared to a historical cohort of 41 patients that received conventional treatment. Primary endpoints were death, treatment success and long-term preservation of intestinal continuity. Secondary endpoints were length of hospital stay and duration of treatment.
Results
There was no difference in mortality (p = 0.624). The intention-to-treat analysis showed a significantly higher success rate of EVT compared to conventional treatment (95.2% vs. 65.9%, p = 0.011). EVT was associated with preservation of intestinal continuity in a significant higher percentage of patients than patients undergoing conventional treatment (86.7% vs. 37.5%, p = 0.001). Conventional treatment tended to a shorter length of hospital stay (31.1 vs. 42.2 days, p = 0.066) but with no difference in overall duration of treatment. Time until closing of a diverting stoma did not differ between groups (10.2 months in the EVT group vs. 9.4 months in the conventional treatment group, p = 0.721).
Conclusion
According to this retrospective study, conventional therapy and EVT are both options for the treatment of anastomotic leakage after rectal resection. EVT might be more effective in terms of definite healing and preservation of intestinal continuity.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Vacuum-assisted wound closure (VAC) has some advantages over traditional wound management and is very commonly used in various fields of surgery [1]. The first larger patient series for endoscopic use of vacuum therapy was published by Weidenhagen et al. [2]. The working group from Munich successfully used endoscopic vacuum therapy (EVT) to treat anastomotic leaks after rectal resection. Published case series report on high average success and stoma reversal rates. Our working group has already reported on successful EVT for various other defects comprising rectal perforations and other colorectal lesions [3]. Thanks to this new approach, an operative revision with relaparotomy can be avoided in the majority of patients. Therefore, EVT has become the treatment of choice for extraperitoneal anastomotic leakage after rectal or recto-sigmoid resection in several institutions in Germany and commercially available systems are now distributed in approximately 30 countries worldwide. However, there is still no evidence that EVT is superior to any other treatment for anastomotic leakage after rectal resection. This study aimed at comparing outcomes after EVT to conventional treatment for anastomotic leakage.
Methods
All patients (n = 62) had undergone rectal or recto-sigmoid resection at the department of surgery, University of Rostock, Rostock, Germany. Twenty-one patients treated with EVT for anastomotic leakage after rectal or recto-sigmoid resection were retrospectively compared to a historical cohort of 41 patients that received conventional treatment (Table 1). These 41 patients were recruited from a database for colorectal cancer (420 rectal and 709 colon cancer patients), and all of them were operated between 2000 and 2012. All patients receiving EVT were treated between November 2007 and March 2015. Treatment modality for leakage was indicated by the responsible surgeon.
Inclusion criteria were rectal or recto-sigmoid resection and an extraperitoneal anastomotic leakage or rectal stump insufficiency. All anastomoses were performed in double-stapling technique end to end. Anastomotic leakage was identified postoperatively as described previously [4]: In case of unusual elevation of CRP or white blood cell count, clinical symptoms as well as suspicious drain secretion, diagnostics were performed to determine an anastomotic leakage by rectal digital examination, water-soluble contrast study, endoscopy or CT scan. If any of the diagnostic tools showed an anastomotic leakage, it was documented as such regardless of the clinical consequences (stages I–III). Exclusion criteria were: primary treatment in other hospitals, Crohn’s disease, ulcerative colitis, chronic fistulas and iatrogenic perforations. Only patients with primary anastomosis were considered for analysis of long-term preservation of intestinal continuity (Table 2).
The following parameters were collected from charts or during patients’ follow-up visits: basic patient characteristics, type and duration of neoadjuvant treatment, details of rectal or recto-sigmoid resection, details of anastomotic leak, type of therapy, details of therapy, success rate (anastomotic healing as proven by endoscopy and patient recovery), time to stoma reversal, complications of therapy, and in-hospital mortality.
Primary endpoints were death, treatment success and long-term preservation of intestinal continuity. Treatment success was defined as healing of the anastomotic leakage or rectal stump insufficiency. Long-term preservation of intestinal continuity was defined as the absence of a stoma after 12 months. Secondary endpoints were length of hospital stay and duration of treatment. All patients were followed for at least 15 months.
This study was performed as an intention-to-treat (ITT) analysis. Outcome of patients receiving initial EVT or conventional treatment was compared. In 21 patients, EVT was used as first-line therapy; in further seven patients, EVT was used as second-line therapy after failure of conventional treatment.
All patients or their legal representatives had given written informed consent to the interventions.
Endoscopic vacuum therapy (EVT)
EVT was performed as described before [3]. Briefly, flexible endoscopic examination and lavage were conducted. Sponges were then cut accordingly to the size of the cavity and installed transanally via an overtube. If the leakage became too small for placing the sponge intracavitary and the wound healing was considered to be insufficient for terminating the treatment, we placed the sponge intraluminally covering the cavity. The polyurethane sponges were changed every 3 days. Wound healing was evaluated after each cycle of EVT. The commercially available system Endo-Sponge (B. BRAUN®, Melsungen, Germany) was used in all patients receiving EVT. All polyurethane sponges were placed and changed in the surgical endoscopy unit of our department, in the operating room or on the intensive care unit.
Conventional treatment
Modalities of conventional treatment are presented in Table 2. Whether conventional or endoscopic treatment was applied was based on an individual decision of the responsible surgeon. In the conventional group, the leaks were treated by drainage (percutaneous (CT-assisted) or surgically placed), relaparotomy with lavage and diverting ileostomy, anastomotic re-suturing or resection of the anastomosis with proximal colostomy and closure of the rectal stump (Hartmann procedure).
Statistical analysis
Statistical analysis was performed using Statistical Package for Social Science (SPSS), version 23.0. Statistical analysis was conducted using Pearson’s Chi-square test (Fisher’s exact test) or t test. A p value of <0.05 was considered as statistically significant.
Results
Patients’ characteristics are shown in Table 1. There was a significant higher rate of colorectal carcinoma in the conventional treatment group than in the EVT group. Neoadjuvant therapy was conducted in 48.3% of all patients. There was a significant higher proportion of neoadjuvant-treated patients in the conventional treatment group (53.7 vs. 38.1%, p = 0.008). Of note, in 21 patients EVT was used as first-line therapy; in further seven patients, EVT was used as second-line therapy after failure of conventional treatment. A mean number of seven sponges were used in the EVT group. In around 60% of patients treated with EVT, sponges were placed intracavitary, and in the remaining 40%, sponge placement went from initially intracavitary to intraluminally. There was no difference in mortality between both groups (overall, n = 2, 3.2%; EVT 4.8% vs. conventional treatment 2.4%, p = 0.624). In one patient of the EVT group, EVT had led to local but not systemic control of septic progress. One patient in the conventional treatment group died due to aggravation of septic complications after anastomotic leakage. Analysis for treatment success based on the initial treatment modality revealed an overall success rate of 75.8% for treatment of anastomotic leakage (Table 2). The outcome analysis based on the initial treatment showed a significantly higher success rate of EVT compared to conventional treatment (95.2% vs. 65.9%, p = 0.011). Analysis based on final treatment (including all patients that switched from conventional to EVT group) showed an overall success rate of 80.6% (Table 3). Here, EVT showed higher numerical success rates without reaching statistical significance (85.7 vs. 76.5%).
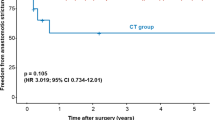
EVT was associated with preservation of intestinal continuity in a significant higher percentage of patients than patients undergoing conventional treatment (86.7% vs. 37.5%, <p = 0.001).
Conventional treatment tended to a shorter length of hospital stay without reaching statistical significance (31.1 vs. 42.2 days, p = 0.066). Time until closing of a diverting stoma did not differ between groups (10.2 months in the EVT group vs. 9.4 months in the conventional treatment group, p = 0.721). Further treatment characteristics and outcomes are presented in Table 2.
Discussion
A very recent systematic review by Shalaby et al. [5] analyzed the outcome of EVT for anastomotic leaks in 276 patients arising from 17 different studies/case series. The mean rate of success was 85.3% with a median duration of therapy of 47 days. The mean rate of stoma reversal across the studies was 75.9%. Despite the very convincing results of EVT for treatment of anastomotic leaks, there is no evidence for the superiority of EVT over any other treatment regarding success rate, duration of therapy or restoration of intestinal continuity. Therefore, we aimed to compare results of EVT to a historical cohort of patients with anastomotic leaks after rectal resections for rectal cancer.
Only few study groups compared specific treatment forms for anastomotic leaks after colorectal surgery. Nagell and Holte [6] compared four patients treated with EVT for anastomotic leakage after rectal resection to a control group of ten patients undergoing conservative therapy. The median healing time for patients with EVT was 51 days (range, 43–195). The control group had a significantly longer healing time of 336 days (range, 52–1434).
Blumetti et al. [7] analyzed treatment and outcome of intra- and extraperitoneal anastomotic leaks in 103 patients after colorectal surgery. Non-operative management (i.e., antibiotics, percutaneous drainage) in patients with extraperitoneal anastomotic leaks was successful in 57%. Operative revision (i.e., diverting ileostomy and drain, Hartmann’s procedure, resection with redoing anastomosis) was successful in 41% of patients. Failure of treatment was defined as evidence of persistent leak or persistent stoma.
In a study by Gardenbroek et al. [8], treatment of anastomotic leakage after pouch-anal anastomosis for ulcerative or FAP was analyzed. They compared 15 patients who received EVT after transanal re-suturing of anastomosis to a historical control group (n = 30) that had undergone conventional treatment. The primary endpoint of the study was anastomotic healing after 6 months. There was a healed anastomosis in all patients that had received EVT compared to 52% in the conventional group (p = 0.003). Time to healing was 48 days in the EVT group compared to 70 days in the control group (p = 0.013). There was no statistically significant difference in the stoma reversal rate (EVT 93% vs. 89% in conventional group) or in the rate of long-term pouch failure (EVT 7% vs. 14.1% in the conventional group).
Another study examined the effect of endoscopic treatment on healing of anastomotic leaks after anterior rectal resection [9]. Twenty patients underwent either conventional operative or endoscopic treatment. The endoscopic treatment included either endoscopic debridement in combination with stenting, endoluminal vacuum therapy or fibrin injection. Mean healing time of the anastomotic leak in the endoscopic and conventional group was 105 and 173 days, respectively. The stoma reversal rate was similar in both groups (50 vs. 57%), but the overall rate of patients without colostomy was higher in the endoscopic group (77 vs. 57%).
In our patient series, outcome analysis based on the initial treatment showed a significantly higher success rate of EVT compared to conventional treatment. However, when study groups were classified by final treatment, the potential benefit was not significant anymore. This could be due to delayed start of EVT after failure of conventional treatment. Next to treatment success, the difference of preservation or restoration of bowel continuity was an interesting and impressive finding of our analysis. Intestinal continuity could be preserved or restored in 86.7% of patients undergoing EVT but only in 37.5% of patients receiving conventional treatment (p < 0.001). Other reports from the “pre-EVT era” confirm that approximately 30–40% of patients who undergo bowel diversion owing to anastomotic leaks after rectal resection will not undergo stoma reversal [9, 10].
There are some limitations of this analysis that have to be mentioned: the retrospective study design with two groups that were not completely comparable with regard to baseline characteristics. In the conventional group, there were a significant higher proportion of patients with colorectal cancer than in the EVT group. Accordingly, fewer patients in the EVT group received neoadjuvant treatment which may be a reason for the higher success rate. Therefore, the data presented should be considered with caution. All results should only be considered as trends because a selection bias cannot be excluded in the present study. However, due to lack of available data in the current literature, we believe that this analysis might contribute to a better management of patients with anastomotic leaks after rectal resection.
Conclusion
According to this retrospective comparison study, conventional therapy and EVT are both options for the treatment of anastomotic leakage after rectal resection. EVT might be more effective in terms of definite healing and preservation of intestinal continuity, whereas conventional treatment tends to a shorter length of hospital stay.
Availability of data and material
All data and materials are contained within the manuscript.
Abbreviations
- EVT:
-
Endoscopic vacuum therapy
- VAC:
-
Vacuum-assisted wound closure
- CT:
-
Computed tomography
- SPSS:
-
Statistical Package for Social Science
- FAP:
-
Familial adenomatous polyposis
- LAR:
-
Low anterior resection
References
Argenta LC, Morykwas MJ (1997) Vacuum-assisted closure: a new method for wound control and treatment: clinical experience. Ann Plast Surg 38:563–576
Weidenhagen R, Gruetzner KU, Wiecken T, Spelsberg F, Jauch KW (2008) Endoscopic vacuum-assisted closure of anastomotic leakage following anterior resection of the rectum: a new method. Surg Endosc 22:1818–1825
Kuehn F, Janisch F, Schwandner F, Alsfasser G, Schiffmann L, Gock M, Klar E (2016) Endoscopic vacuum therapy in colorectal surgery. J Gastrointest Surg 20:328–334
Schiffmann L, Wedermann N, Gock M, Prall F, Klautke G, Fietkau R, Rau B, Klar E (2013) Intensified neoadjuvant radiochemotherapy for rectal cancer enhances surgical complications. BMC Surg 13:43
Shalaby M, Emile S, Elfeki H, Sakr A, Wexner SD, Sileri P (2018) Systematic review of endoluminal vacuum-assisted therapy as salvage treatment for rectal anastomotic leakage. BJS Open 3:153–160
Nagell CF, Holte K (2006) Treatment of anastomotic leakage after rectal resection with transrectal vacuum-assisted drainage (VAC). A method for rapid control of pelvic sepsis and healing. Int J Colorectal Dis 21:657–660
Blumetti J, Chaudhry V, Cintron JR, Park JJ, Marecik S, Harrison JL, Prasad LM, Abcarian H (2014) Management of anastomotic leak: lessons learned from a large colon and rectal surgery training program. World J Surg 38:985–991. https://doi.org/10.1007/s00268-013-2340-y
Gardenbroek TJ, Musters GD, Buskens CJ, Ponsioen CY, D’Haens GR, Dijkgraaf MG, Tanis PJ, Bemelman WA (2015) Early reconstruction of the leaking ileal pouch-anal anastomosis: a novel solution to an old problem. Colorectal Dis 17:426–432
Chopra SS, Mrak K, Hünerbein M (2009) The effect of endoscopic treatment on healing of anastomotic leaks after anterior resection of rectal cancer. Surgery 145:182–188
Khan AA, Wheeler JM, Cunningham C, George B, Kettlewell M, Mortensen NJ (2007) The management and outcome of anastomotic leaks in colorectal surgery. Colorectal Dis 10:587–592
Acknowledgements
Open Access funding provided by Projekt DEAL.
Funding
This research did not receive any specific grant from funding agencies.
Author information
Authors and Affiliations
Contributions
LS designed research, acquired data, analyzed data, performed statistics and wrote the manuscript. FK designed research, acquired data, analyzed data and wrote the manuscript. FJ, FS, MG, NW, MW and EK acquired data and revised the manuscript critically for important intellectual content. All authors revised and approved the manuscript for publication.
Corresponding author
Ethics declarations
Conflict of interests
The authors declare that they have no competing interest.
Consent for publication
Not applicable.
Ethical approval
According to local ethics committee (Rostock University), no formal ethics approval was required in this retrospective study.
Informed consent
Written informed consent forms about the procedures were obtained from all patients.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kühn, F., Janisch, F., Schwandner, F. et al. Comparison Between Endoscopic Vacuum Therapy and Conventional Treatment for Leakage After Rectal Resection. World J Surg 44, 1277–1282 (2020). https://doi.org/10.1007/s00268-019-05349-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-019-05349-5