
Abstract
Background
There is scarce evidence on whether a total gastrectomy or an Ivor Lewis esophagectomy is preferred for gastroesophageal junction (GEJ) cancers regarding effects on morbidity, pathology, survival and health-related quality of life (HR-QoL). The aim of this study was to investigate the difference in long-term HR-QoL in patients undergoing total gastrectomy versus Ivor Lewis esophagectomy in a tertiary referral center.
Methods
Patients with a follow-up of >1 year after a total gastrectomy or an Ivor Lewis esophagectomy for GEJ/cardia carcinoma completed the EORTC QLQ-C30 and EORTC QLQ-OG25 questionnaires. ‘Problems with eating,’ ‘reflux,’ and ‘nausea and vomiting’ were the primary HR-QoL endpoints. The secondary endpoints were the remaining HR-QoL domains, postoperative complications and pathology results.
Results
Thirty patients after gastrectomy and 71 after esophagectomy were included. Mean age was 63 years. Median follow-up was 2 years (range 12–84 months). Patients after gastrectomy reported less ‘choking when swallowing’ and ‘coughing’ (β = − 5.952, 95% CI − 9.437 to − 2.466; β = − 13.084, 95% CI − 18.525 to − 7.643). More lymph nodes were resected in esophagectomy group (p = 0.008). No difference was found in number of positive lymph nodes, R0 resection or postoperative complications.
Conclusions
After a follow-up of >1 year ‘choking when swallowing’ and ‘coughing’ were less common after a total gastrectomy. No differences were found in postoperative complications or radicality of surgery. Based on this study, no general preference can be given to either of the procedures for GEJ cancer. These results support shared decision making when a choice between the two treatment options is possible.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In 2018, esophageal and gastric cancers were diagnosed in over 570.000 and 1.033.000 patients, respectively, worldwide [1]. Only a small percentage of patients present with a gastroesophageal junction (GEJ) or cardia carcinoma, defined as a tumor involving the GEJ with the epicenter within 2 cm of the cardia (true GEJ tumor) or a tumor of the gastric cardia without esophageal involvement (cardia cancer). The actual incidence of these specific cancers, however, is unknown. The Dutch Upper Gastrointestinal (GI) Cancer audit shows that in 2018, 174 patients were operated for GEJ cancer in the Netherlands, which also includes patients with cardiac tumors [2]. Treatment of gastroesophageal junction tumors is challenging. The therapy for these cancers usually consists of neoadjuvant chemoradiotherapy or perioperative chemotherapy followed by surgery. Different surgical approaches exist: both a total gastrectomy with a Roux-Y reconstruction or an esophagectomy with gastric tube reconstruction can be performed. An esophagectomy can be executed both transhiatally and transthoracically, with either an intrathoracic or cervical anastomosis. Additionally, the operative approach can be open, minimally invasive or hybrid. There is no substantial evidence which is the preferred procedure in terms of postoperative morbidity, mortality, pathology, health-related quality of life (HR-QoL), survival or health-care costs [3,4,5,6]. In addition, the results could be conflicting for the different outcome parameters: an esophagectomy might result in a better long-term survival at the cost of a worse quality of life compared to a gastrectomy or vice versa. Furthermore, not all patients value these outcome parameters the same, as for some patients, survival is more important and for others quality of life. These issues complicate surgical decision making even more.
Functional complaints after Upper GI surgery such as reflux and nausea are common, posing a challenge in maintaining QoL. Therefore, it is of great importance to examine the effects of these operations in terms of functional complaints and HR-QoL in addition to short-term morbidity and long-term survival.
Few studies compared QoL following a total gastrectomy and a transthoracic esophagectomy using different HR-QoL questionnaires [7,8,9,10]. Three out of four of these studies show better HR-QoL after a total gastrectomy, with better global health, role, social functioning and less fatigue [8], better physical functioning and less dyspnea and reflux [9] and less gastrointestinal symptoms [7]. The follow-up time in these studies varied from three months to 2 years. However, these studies had either a low response rate (34.5% and 52.5%) [9, 10] or a small sample size (N = 27 and N = 53) [7, 8], and patients with a distal esophageal cancer were not excluded [8]. The aim of this study was to investigate the differences in long-term HR-QoL domains in a large series of patients with a true GEJ or cardia carcinoma undergoing a total gastrectomy with a Roux-Y reconstruction versus a transthoracic esophagectomy with gastric tube reconstruction with an intrathoracic anastomosis (Ivor Lewis) in a tertiary referral center.
Methods
Study population
All patients following surgery for GEJ or cardia cancer defined as a tumor involving the GEJ with the epicenter within 2 cm of the cardia (true GEJ tumor) or a tumor in the gastric cardia without esophageal involvement (cardia cancer) attending the Amsterdam UMC (location AMC) were asked to participate in the study when they visited the outpatient clinic between 2014 and 2018. Theoretically, all of these patients could have undergone either an esophagectomy or a gastrectomy for their GEJ/cardia tumor. Patients were included if they had undergone a total gastrectomy or an Ivor Lewis esophagectomy for a GEJ or cardia carcinoma with a minimum follow-up of 1 year (operated between 2010 and 2017). Patients with metastases, patients following a transhiatal esophagectomy, patients with a cervical anastomosis, patients with a colonic interposition, patients after salvage esophagectomy or patients with a recurrence or who died during follow-up were excluded. Official ethical approval for this study was waived by the Institutional Review Board of Amsterdam UMC (location AMC). This paper adheres to the STROBE guidelines for the reporting of prospective studies [11].
(Neo)adjuvant therapy
Patients scheduled for an esophagectomy were generally treated with neoadjuvant chemoradiotherapy according to the CROSS scheme [12], and patients for a gastrectomy were treated with perioperative chemotherapy consisting of EOX (Epirubicin, Oxaliplatin and Capecitabine), based on the MAGIC study [13]. Some of the patients in the gastrectomy group received adjuvant chemoradiotherapy because of their participation in the CRITICS trial [14]. If the stomach involvement was more than 3 cm as evaluated by upper GI endoscopy, perioperative chemotherapy instead of neoadjuvant chemoradiotherapy was administered to esophagectomy patients. A diagnostic laparoscopy was performed for advanced T stages (>T3) if the bulk of the tumor was located in the stomach before initiation of neoadjuvant therapy [15].
Surgery
The treatment plan including the surgical procedure was determined during the weekly Multi-Disciplinary Team meeting of the Amsterdam Gastrointestinal oncology outpatient clinic (GIOCA—Gastro-Intestinal Oncologic Center Amsterdam). If more than 2 cm ingrowth in the esophagus was seen and a gastric tube could still be performed (determined during diagnostic laparoscopy), an esophageal resection with gastric tube reconstruction was performed. If ingrowth in the stomach was extensive to a level that a gastric tube could not be created, and ingrowth in the esophagus was limited, a gastrectomy was performed. If clinical lymph node metastases were present in locoregional lymph node stations that did not have an overlap between the esophageal and gastric cancer classification systems, this also influenced the choice for the surgical approach. Excluded were patients that had extensive tumor expansion in both the esophagus and stomach necessitating an esophagogastric resection with colonic interposition. In case of a total gastrectomy, a modified D2 lymphadenectomy was performed, including complete omentectomy with a Roux-Y reconstruction. In case of an esophagectomy, a 2-field lymphadenectomy was performed, including the paratracheal lymph node stations and a gastric tube reconstruction with an intrathoracic anastomosis. Operations were performed using an open as well as a minimally invasive approach.
Follow-up
Outpatient clinic visits were scheduled every 3 months the first year and every 6 months the second–fourth year, and once yearly until the fifth postoperative year. No imaging was performed unless clinically indicated, in accordance with the Dutch guideline [16].
Baseline characteristics and perioperative morbidity
Clinical data were obtained from a prospectively maintained database of all operated patients with an esophageal or gastric cancer in the Amsterdam UMC (location AMC). This database includes patient and tumor characteristics such as age, gender, American Society of Anesthesiologists (ASA) classification and neoadjuvant therapy, details on surgical procedure and perioperative complications.
Health-related quality of life
The European Organization for Research and Treatment of Cancer (EORTC) quality of life questionnaires (EORTC QLQ-C30 and EORTC QLQ-OG25) were handed out during the outpatient clinic visits [17,18,19]. These questionnaires are validated for evaluating HR-QoL in cancer patients and patients with gastroesophageal cancer, respectively. The EORTC QLQ-C30 contains one global health score, five functional scores (physical, role, social, cognitive and emotional functioning) and nine symptom scores (fatigue, nausea and vomiting, pain, dyspnea, insomnia, appetite loss, constipation, diarrhea, financial difficulties). The EORTC QLQ-OG25 contains one functional score (body image) and 15 symptom scores (dysphagia, reflux, odynophagia and problems with eating with others, pain and discomfort, anxiety, problems with eating, dry mouth, trouble with taste, trouble with swallowing of saliva, choking when swallowing, trouble with coughing, trouble with talking, weight loss, hair loss).
All questions employ four response categories ranging from 1 (not at all) to 4 (very much), with the exception of two questions representing global health, whose response options ranged from 1 (very poor) to 7 (excellent). Questionnaire scores were linearly transformed into scores ranging from 0 to 100 (best global health or functioning or worst symptoms) according to the scoring manual of the EORTC QoL Group [20].
Endpoints
The primary endpoints were three HR-QoL domains: ‘nausea and vomiting,’ ‘reflux’ and ‘problems with eating.’ These domains were chosen during a consensus discussion between two surgeons, a medical psychologist and a PhD candidate (SSG, MIBH, MAGS & EJ). The ‘nausea and vomiting,’ ‘reflux’ and ‘problems with eating’ domains were chosen because these symptoms occur most frequently during follow-up according to the recent literature and professional experience [21]. The secondary endpoints were the remaining HR-QoL domains, postoperative complications (such as anastomotic leakage, atrial fibrillation and pulmonary complications) according to the ECCG criteria [22], Clavien–Dindo grade and pathology results (c/ypTNM stage, histology, R0 resection rate, (positive) lymph node count). All endpoints were measured after a follow-up of more than 1 year.
Statistical analysis
Descriptive statistics were used for the analysis of baseline and pathology characteristics as well as postoperative complications. These parameters were reported as proportions for binary or categorical variables, as means with standard deviations (SD) for parametric continuous variables, and as medians with interquartile ranges (IQR) for nonparametric continuous variables. Characteristics of both groups and postoperative morbidity outcomes were compared using the Mann–Whitney U test (for nonparametric continuous variables) or Student’s t test (for parametric continuous variables) and the Chi-square or Fisher’s exact test for categorical data. Univariable linear regression analysis was performed to analyze QoL (sub)domain differences between the gastrectomy and esophagectomy groups. QoL (sub)domains with p < 0.10 were selected subsequently to be included in a multivariable linear regression analysis. The following variables were tested for confounding and effect modification: gender, age, ASA score and neoadjuvant therapy (yes/no). A variable was considered a confounder, if the β of remission changed more than 10%. The variable that resulted in the highest change in β was added first. The other variables were then again tested for confounding until the correlation coefficient of remission did not change >10% (adjusted model). Effect modification was tested using interaction terms. No significant effect modification for the tested variables was found. Results were presented with a mean difference between both groups and corresponding 95% confidence interval (CI). All p values were based on a 2-sided test. Given the many outcomes, the number of statistical tests relative to the sample size is large. Therefore, a stringent p value below 0.01 was considered statistically significant. A difference in mean values of HR-QoL domains of more than 10 points between the two procedures was considered clinically relevant according to the EORTC guideline [19]. Statistical analyses were performed in SPSS Statistics version 24.
Results
Demographic and clinical characteristics
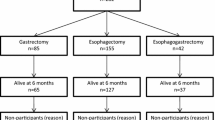
One-hundred and twenty-six eligible patients were asked to complete the questionnaires. The response rate was 80.2%, resulting in 101 included patients, 30 in the gastrectomy group and 71 in the esophagectomy group (Fig. 1). Baseline characteristics of the study population are depicted in Table 1. Mean age was 63 years. Most patients were male (83.2%). Gender, ASA classification and comorbidities did not statistically differ between treatment groups. As expected, perioperative chemotherapy was applied more often in the gastrectomy group and neoadjuvant chemoradiotherapy more in the esophagectomy group. A minimally invasive operation was performed in 23 patients (76.6%) in the gastrectomy group and in 67 patients (94.4%) in the esophagectomy group (p = 0.015). Median follow-up was 24 months (range 12–84 months) in the gastrectomy group and also 24 months (range 12–72 months) in the esophagectomy group.

Study flowchart
Endpoints
Primary endpoints
The results of the multivariable analysis of HR-QoL domains are presented in Table 2. Additional data of univariable analysis is given in supplementary Table 1. The difference between the mean scores of the ‘problems with eating’ domain was more than 10 points, which makes the difference clinically relevant. However, no significant difference was found in ‘problems with eating,’ ‘reflux’ or ‘nausea and vomiting’ between the gastrectomy and esophagectomy groups.
Secondary endpoints: remaining HR-QoL domains
Of the remaining HR-QoL domains, patients after total gastrectomy reported significantly ‘less choking when swallowing’ (p = 0.001) and ‘trouble with coughing’ (p < 0.001). These differences were also clinically relevant according to EORTC as the difference in mean scores was more than 10 points in both domains. No significant differences were found in ‘global health,’ or in any of the functioning scores, ‘fatigue,’ ‘pain,’ ‘dyspnea,’ ‘insomnia,’ ‘appetite loss,’ ‘constipation,’ ‘diarrhea,’ ‘financial difficulties,’ ‘dysphagia,’ ‘odynophagia,’ ‘pain and discomfort,’ ‘anxiety,’ ‘eating with others,’ ‘dry mouth,’ ‘trouble with taste’ or ‘swallowing saliva,’ ‘trouble with talking,’ ‘weight loss’ and ‘hair loss’ between the gastrectomy and esophagectomy groups.
Secondary endpoints: perioperative morbidity
The occurrence of postoperative complications did not significantly differ between the two groups (Table 3). In particular, no significant difference in atrial fibrillation, anastomotic leakage, pneumonia and Clavien–Dindo classification was found between the gastrectomy and the esophagectomy group.
Secondary endpoints: pathology results
Pathology results are displayed in Table 4. Most patients in both groups presented with an adenocarcinoma (98 patients). In the gastrectomy group, 26 patients had a cardia carcinoma, and 4 patients had a GEJ tumor. In the esophagectomy group, 69 patients had a GEJ tumor and 2 patients had cardia carcinoma. cT3 and cN0 were most often seen in both groups. In both the gastrectomy and esophagectomy groups, one patient had an R1 resection (3.3% vs 1.4%, p = 0.508). In the esophagectomy group, significantly more lymph nodes were resected (p = 0.008), however, no difference in lymph node metastases was found. In addition, there were no significant differences in tumor regression grade.
Discussion
This study describes the difference in long-term quality of life in disease-free patients who underwent either a total gastrectomy or an Ivor Lewis esophagectomy for GEJ or cardia cancer. We found no significant difference in the primary endpoint HR-QoL domains ‘problems with eating,’ ‘reflux’ and ‘nausea and vomiting.’ Of the secondary HR-QoL endpoints, significantly less ‘problems with choking when swallowing’ and ‘coughing’ were found after gastrectomy. These differences were also clinically relevant. No significant differences were found in the occurrence and grade of postoperative complications. Furthermore, more lymph nodes were resected during esophagectomy with an equal number of positive lymph nodes and an equal R0 resection rate.
In the few studies on long-term HR-QoL in patients with GEJ carcinoma after esophagectomy or gastrectomy, an overall decrease in HR-QoL was observed after esophagogastric surgery, which restored within 6–12 months in disease-free patients [10, 23,24,25]. Generally, better global health and functional outcomes such as role and social functioning are found after a total gastrectomy compared to esophagectomy [8]. Also less fatigue, pneumonia and reflux-related symptoms are found after gastrectomy compared to esophagectomy [8, 9]. Our results are different compared to these studies as no significant difference in global health or functioning domains was found. Furthermore, no significant difference was found in reflux or fatigue scores. The former studies were heterogenous with respect to included patients (e.g., both distal esophageal, GEJ and cardia cancer) [8] and baseline characteristics (age, gender, comorbidity, neoadjuvant therapy, open/minimally invasive approach) [7,8,9,10]. In three of these studies, no correction for confounders was performed [7,8,9]. Furthermore, these studies had either a low response rate (34.5% and 52.5%) [9, 10] or a small sample size (N = 27 and N = 53) [7, 8]. In addition, except for the study by Fuchs et al., follow-up was short, ranging from three to six months [7, 8, 10]. The current study describes a large patient cohort with a true GEJ/cardia carcinoma with a high response rate and long follow-up time. In addition, correction for confounders such as differences in baseline characteristics was performed. The long follow-up time decreased the influence of surgical approach (open versus minimally invasive) and neoadjuvant therapy (chemo- or chemoradiotherapy) on HR-QoL.
No significant difference was found in postoperative complications and Clavien–Dindo classification. More specifically, no differences were observed in anastomotic leakage rates between the groups, which corresponds with the findings of Schumacher et al. who compared a transthoracic esophagectomy (N = 29) with a gastrectomy (N = 67) in GEJ carcinoma [26]. They did find a significant difference in the occurrence of atrial fibrillation between the two groups, which can be explained by the transthoracic phase of the procedure in Ivor Lewis esophagectomy. This finding corresponds to those of other recent studies. The study of Lohani et al. found that the transthoracic approach (N = 134) was an independent risk factor for the development of atrial fibrillation after surgery compared to transhiatal approach (N = 58) [27]. In our study, we did not observe such difference and the complication rate is comparable to that of other studies [14, 28, 29]. In the present study, a minimally invasive approach was performed in 94.4% of the patients in the esophagectomy group. The open approach with right thoracotomy is well known to account for the majority of postoperative pulmonary complications (both pneumonia and pleural effusion) which drop significantly when adopting the minimally invasive approach [30]. The similar rate reported between the gastrectomy and the esophagectomy groups in postoperative pulmonary complications as well as the comparable results in symptoms such as dyspnea could be explained by the reduced pulmonary surgical trauma.
There are limitations of this study that merit attention. Patients who did not participate in the study could have had a worse or better HR-QoL. However, a response rate of 80.2% was achieved, which is higher than the response rates published in recent studies [9, 10]. More importantly, baseline HR-QoL data are lacking. It remains unknown whether the treatment groups differed a priori with respect to HR-QoL and how HR-QoL may have changed over time. Two ongoing studies are relevant in this respect as they include a baseline. The RENAISSANCE trial in Germany investigates the effect of chemotherapy alone versus chemotherapy followed by surgery on survival and HR-QoL in patients with limited-metastatic adenocarcinoma of the stomach or esophagogastric junction [31]. The POCOP cohort study in the Netherlands is set up to obtain clinical and HR-QoL data from patients with esophageal and gastric cancer at different points over time [32]. Furthermore, the two treatment groups differed with respect to sample size (30 vs 71) and baseline characteristics, with more patients having received chemoradiotherapy and significantly more minimally invasive procedures in the esophagectomy group. For most of these baseline characteristics, statistical correction was performed. One should keep in mind that we could not adjust for all differences, in this naturally occurring sample. Conducting a randomized clinical trial with a sufficiently large number of patients with true GEJ carcinoma is a challenge that is yet to be taken up. Moreover, given the many outcomes the number of statistical tests relative to the sample size is large. However, a stringent p value of < 0.01 for significance was chosen to counteract this obstacle. Although we distinguished between primary and secondary outcomes, some of the results may have been found by chance. Moreover, the results of morbidity and pathology are biased by the inclusion criteria (alive and disease-free) and are therefore only applicable to the selected group of patients in this study with a long recurrence-free survival. Finally, the inclusion criterion ‘alive and disease-free’ precluded the investigation of a possible long-term survival difference between the two treatment groups. Conflicting results for HR-QoL and survival may be observed in such a study, and, additionally, individual patients may also value QoL and survival differently, making both endpoints essential subjects for future research projects. Yet, this study currently provides the most reliable long-term HR-QoL data.
In conclusion, after a follow-up of more than 1 year no significant difference was found in ‘problems with eating,’ ‘reflux’ or ‘nausea and vomiting.’ Of the less clinically relevant HR-QoL domains, ‘choking when swallowing’ and ‘coughing’ were found to be significantly less common in the gastrectomy group. No significant difference was found in postoperative complications or radicality of surgery. Based on this study, it is difficult to determine a priori which procedure for GEJ cancer is to be preferred. However, the study provides important information on long-term HR-QoL following major Upper GI surgery. Patients may be informed about the HR-QoL domains that are likely to be affected by the different surgical procedures, which in turn may support shared decision making when a choice between the two treatment options is possible. A multicenter randomized trial examining long-term HR-QoL, postoperative complications and pathology results in patients with GEJ or cardia carcinoma is the logical, much needed, next step.
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 68(6):394–424
DUCA. https://dica.nl/duca/home. Accessed 4 June 2019
Busweiler LA, Henneman D, Dikken JL, Fiocco M, van Berge Henegouwen MI, Wijnhoven BP, van Hillegersberg R, Rosman C, Wouters MW, van Sandick JW, D.U.G.C.A. group (2017) Failure-to-rescue in patients undergoing surgery for esophageal or gastric cancer. Eur J Surg Oncol 43(10):1962–1969
Liu JF, Wang Q, Ping YM, Zhang YD (2008) Complications after esophagectomy for cancer: 53-year experience with 20,796 patients. World J Surg 32(3):395–400. https://doi.org/10.1007/s00268-007-9349-z
Sauvanet A, Mariette C, Thomas P, Lozac’h P, Segol P, Tiret E, Delpero JR, Collet D, Leborgne J, Pradère B, Bourgeon A, Triboulet JP (2005) Mortality and morbidity after resection for adenocarcinoma of the gastroesophageal junction: predictive factors. J Am Coll Surg 201(2):253–262
Karl RC, Schreiber R, Boulware D, Baker S, Coppola D (2000) Factors affecting morbidity, mortality, and survival in patients undergoing Ivor Lewis esophagogastrectomy. Ann Surg 231(5):635–643
Spector NM, Hicks F, Pickleman J (2002) Quality of life and symptoms after surgery for gastroesophageal cancer: a pilot study. Gastroenterol Nurs 25:120e5
Barbour AP, Lagergren P, Hughes R, Alderson D, Barham CP, Blazeby JM (2008) Health-related quality of life among patients with adenocarcinoma of the gastro-oesophageal junction treated by gastrectomy or oesophagectomy. Br J Surg 95:80e4
Fuchs H, Hölscher A, Leers J, Bludau M, Brinkmann S, Schröder W, Alakus H, Mönig S, Gutschow CA (2016) Long-term quality of life after surgery for adenocarcinoma of the esophagogastric junction: extended gastrectomy or transthoracic esophagectomy? Gastric Cancer 19(1):312–317
Kauppila JH, Ringborg C, Johar A, Lagergren J, Lagergren P (2018) Health-related quality of life after gastrectomy, esophagectomy, and combined esophagogastrectomy for gastroesophageal junction adenocarcinoma. Gastric Cancer 21(3):533–541
von Elm E, Altman D, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, S. Initiative (2008) The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol 61(4):344–349
Shapiro J, van Lanschot JJB, Hulshof MCCM, van Hagen P, van Berge Henegouwen MI, Wijnhoven BPL, van Laarhoven HWM, Nieuwenhuijzen GAP, Hospers GAP, Bonenkamp JJ, Cuesta MA, Blaisse RJB, Busch ORC, Ten Kate FJW, Creemers GM, Punt CJA, Plukker JTM, Verheul HMW (2015) Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): long-term results of a randomised controlled trial. Lancet Oncol 16(9):1090–1098.
Ostwal V, Sahu A, Ramaswamy A, Sirohi B, Bose S, Talreja V, Goel M, Patkar S, Desouza A, Shrikhande SV (2017) Perioperative epirubicin, oxaliplatin, and capecitabine chemotherapy in locally advanced gastric cancer: safety and feasibility in an interim survival analysis. J Gastric Cancer 17(1):21–32
Cats A, Jansen E, van Grieken NCT, Sikorska K, Lind P, Nordsmark M, Meershoek-Klein Kranenbarg E, Boot H, Trip AK, Swellengrebel HAM, van Laarhoven HWM, Putter H, van Sandick JW, van Berge Henegouwen MI, Hartgrink HH, van Tinteren H, van de Velde CJH (2018) Chemotherapy versus chemoradiotherapy after surgery and preoperative chemotherapy for resectable gastric cancer (CRITICS): an international, open-label, randomised phase 3 trial. Lancet Oncol 19(5):616–628
Oncoline. https://www.oncoline.nl/maagcarcinoom. Accessed 4 June 2019
Oncoline. https://www.oncoline.nl/oesofaguscarcinoom. Accessed 4 June 2019
EORTC. http://www.eortc.org/. Accessed 4 June 2019
Lagergren P, Fayers P, Conroy T, Stein HJ, Sezer O, Hardwick R, Hammerlid E, Bottomley A, Van Cutsem E, Blazeby JM, E.O.f.R.T.o.C.G.a.Q.o.L. Groups (2007) Clinical and psychometric validation of a questionnaire module, the EORTC QLQ-OG25, to assess health-related quality of life in patients with cancer of the oesophagus, the oesophago-gastric junction and the stomach. Eur J Cancer 43(14):2066–2073
Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, Filiberti A, Flechtner H, Fleishman SB, de Haes JC et al (1993) The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 85(5):365–376
Fayers P, Aaronson NK, Bjordal K, Groenvold M, Curran D, Bottomley A (2001) EORTC QLQ-C30 Scoring Manual, 3rd edn. European Organisation for Research and Treatment of Cancer, Brussels
Kauppila JH, Johar A, Lagergren P (2018) Postoperative complications and health-related quality of life 10 years after esophageal cancer surgery. Ann Surg. https://doi.org/10.1097/SLA.0000000000002972
Low DE et al (2015) International Consensus on Standardization of Data Collection for Complications Associated With Esophagectomy: Esophagectomy Complications Consensus Group (ECCG). Ann Surg 262(2):286–294
Viklund P, Lindblad M, Lagergren J (2005) Influence of surgery-related factors on quality of life after esophageal or cardia cancer resection. World J Surg 29(7):841–848. https://doi.org/10.1007/s00268-005-7887-9
Brooks JA, Kesler K, Johnson CS, Ciaccia D, Brown JW (2002) Prospective analysis of quality of life after surgical resection for esophageal cancer: preliminary results. J Surg Oncol 81:185–194
Zieren H, Jacobi CA, Zieren J, Muller JM (1996) Quality of life following resection of oesophageal carcinoma. Br J Surg 83:1772–1775
Schumacher G, Schmidt S, Schlechtweg N, Roesch T, Sacchi M, von Dossow V, Chopra SS, Pratschke J, Zhukova J, Stieler J, Thuss-Patience P, Neuhaus P (2009) Surgical results of patients after esophageal resection or extended gastrectomy for cancer of the esophagogastric junction. Dis Esophagus 22(5):422–426
Lohani KR, Nandipati K, Rollins SE, Fetten K, Lee TH, Pallati PK, Yamamoto SR, Mittal SK (2015) Transthoracic approach is associated with increased incidence of atrial fibrillation after esophageal resection. Surg Endosc 29(7):2039–2045
Brinkmann S, Schroeder W, Junggeburth K, Gutschow CA, Bludau M, Hoelscher AH, Leers JM (2016) Incidence and management of chylothorax after Ivor Lewis esophagectomy for cancer of the esophagus. J Thorac Cardiovasc Surg 1(5):1398–1404
Fransen L, Berkelmans G, Asti E, Van Berge Henegouwen M, Berlth F, Bonavina L, Brown A, Bruns C, Gisbertz S, Grimminger P, Gutschow C, Hölscher A, Kauppi J, Lagarde SM, Mercer S, Moons J, Nafteux P, Nilsson M, Palazzo F, Pattyn P (2018) FA01.02: The effect of postoperative complications after mie on long-term survival: a retrospective, multi-center cohort study. Dis Esophagus 31(13):1
Straatman J, van der Wielen N, Cuesta MA, Daams F, Roig Garcia J, Bonavina L, Rosman C, van Berge Henegouwen MI, Gisbertz SS, van der Peet DL (2017) Minimally invasive versus open esophageal resection: three-year follow-up of the previously reported randomized controlled trial: the TIME trial. Ann Surg 266(2):232–236
Al-Batran SE et al (2017) The RENAISSANCE (AIO-FLOT5) trial: effect of chemotherapy alone vs. chemotherapy followed by surgical resection on survival and quality of life in patients with limited-metastatic adenocarcinoma of the stomach or esophagogastric junction—a phase III trial of the German AIO/CAO-V/CAOGI. BMC Cancer 17(1):893
Coebergh van den Braak RRJ, van Rijssen LB, van Kleef JJ, Vink GR, Berbee M, van Berge Henegouwen MI, Bloemendal HJ, Bruno MJ, Burgmans MC, Busch ORC, Coene PPLO, Coupé VMH, Dekker JWT, van Eijck CHJ, Elferink MAG, Erdkamp FLG, van Grevenstein WMU (2018) Nationwide comprehensive gastro-intestinal cancer cohorts: the 3P initiative. Acta Oncol 57(2):195–202
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
E. Jezerskyte, L.M. Saadeh, E.R.C. Hagens, M.A.G. Sprangers, L. Noteboom, PhD, W.J. Eshuis and S.S. Gisbertz have no conflicts of interest to declare. M.I. van Berge Henegouwen has a consultant role with Mylan, Johnson and Johnson and Medtronic. Research funding from Olympus and Stryker. H.W.M. van Laarhoven has a consultant or advisory role with BMS, Lilly, MSD, Nordic Pharma, Servier and has research funding from Bayer, BMS, Celgene, Janssen, Lilly, Nordic Pharma, Philips, Roche, Servier.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Jezerskyte, E., Saadeh, L.M., Hagens, E.R.C. et al. Long-Term Quality of Life After Total Gastrectomy Versus Ivor Lewis Esophagectomy. World J Surg 44, 838–848 (2020). https://doi.org/10.1007/s00268-019-05281-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-019-05281-8