
Abstract
Background
Primary aldosteronism (PA) is the most common cause of secondary hypertension. Surgery is the mainstay of treatment for unilateral dominant PA, but reported cure rates varies. The aim of the present study was to investigate contemporary follow-up practices and cure rates after surgery for PA in Sweden.
Methods
Patients operated for PA and registered in the Scandinavian Quality Register for Thyroid, Parathyroid and Adrenal Surgery (SQRTPA) 2009–2015 were identified. Patient data were extracted, and follow-up data (1–24 months) was recorded. Doses of antihypertensive medication and potassium supplementation were calculated using defined daily doses (DDD), and the Primary Aldosteronism Surgical Outcome (PASO) criteria were used to evaluate outcomes.
Results
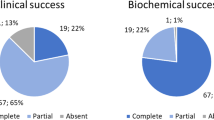
Of 190 registered patients, 171 (47% female, mean age 53 years, median follow-up 3.7 months) were available for analysis. In 75 patients (44%), missing data precluded evaluation of biochemical cure according to the PASO criteria. Minimal invasive approach was used in 168/171 patients (98%). Complication rate (Clavien-Dindo >3a) was 3%. No mortality was registered. Pre/postoperatively 98/66% used antihypertensives (mean DDD 3.7/1.5). 89/2% had potassium supplementation (mean DDD 2.0/0) before/after surgery. Complete/partial biochemical and clinical success according to the PASO criteria were achieved in 92/7% and 34/60%, respectively.
Conclusion
In this study, reflecting contemporary clinical practice in Sweden complete/partial biochemical and clinical success after surgery for PA was 92/7% and 34/60%. Evaluation of biochemical cure was hampered by lack of uniform reporting of relevant outcome measures. We suggest mandatory reporting of surgical outcomes using the PASO criteria for all units performing surgery for PA.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Primary aldosteronism (PA) is a disease caused by an overproduction of aldosterone from the cortex of one or both adrenal glands [1]. The prevalence is reported as 5–13% in the general hypertensive population [2,3,4] making it the most common cause of secondary hypertension, often associated with hypokalaemia [5, 6]. A two to five times increased risk of myocardial infarction, coronary heart disease, heart failure and atrial fibrillation has been reported in patients with PA compared to matched patients with essential hypertension [7]. In the long-term, PA causes fibrosis and remodelling in critical organs which leads to increased risk of cardiovascular, renal and cerebrovascular morbidity and mortality [8,9,10].
In more than 90% of patients, PA is caused by uni- or bilateral idiopathic adrenal hyperplasia or an adrenocortical adenoma [11]. After confirmatory testing, the recommended procedure to differentiate between unilateral and bilateral overproduction is adrenal venous sampling (AVS) [12]. Patients with bilaterally increased aldosterone production and patients with unilateral disease who are not candidates for surgery are best treated with mineralocorticoid receptor antagonists (MRA) [13], whereas unilateral dominant PA is a potentially surgically curable condition [14].
Definitions of cure after surgery for PA have been diverse and reported cure rates from different centres range from 16 to 72% [15,16,17,18,19]. Data from population-based series are scarce. Recently, uniform reporting criteria for outcome after surgery for PA have been proposed. The primary aldosteronism surgical outcome (PASO) study [20] developed consensus criteria for both clinical and biochemical outcomes. In summary, six outcomes were defined in the study: clinical outcome (complete, partial and absent success) and biochemical outcome (complete, partial and absent success). Clinical outcome evaluation is based on blood pressure and use of antihypertensive drugs. Biochemical outcome is based on potassium, aldosterone and renin concentrations. The aim of this register-based study was to investigate actual follow-up routines, and contemporary outcomes of surgical treatment for unilateral dominant PA in Sweden using the PASO criteria.
Methods and materials
All registered patients with PA who underwent unilateral adrenalectomy in Sweden between January 2009 and December 2015 were identified in the Scandinavian Quality Register for Thyroid, Parathyroid and Adrenal Surgery (SQRTPA), https://sqrtpa.se. The SQRTPA started in 2004 and from 2009, it incorporated adrenal procedures. It is recognized by the Swedish National Board for Health and Social Welfare as the national quality registry for endocrine surgical procedures in Sweden. The quality of data is checked by external audit, comparing registered data to hospital medical records. Data quality is overall good, with an error rate of <5%.
The SQRTPA has a variable for preoperative aldosterone-to-renin ratio (ARR) but does not contain detailed data on case finding and confirmatory testing for PA. In Sweden during the time period, case finding was performed in risk groups with the aldosterone-to-renin ratio (ARR), confirmatory testing was performed with the intravenous saline suppression test at all but one centre which used the fludrocortisone suppression test [2].
Data were extracted from SQRTPA and additional patient data collection was performed at each reporting centre with the use of a standardized case report form. The selected variables were pre/postoperative serum potassium, ARR (increased/normal/subnormal), systolic/diastolic blood pressure, use of antihypertensive medication, potassium substitution, reported histologic diagnosis, surgical complications and follow-up time. Moreover, lateralization ratio at preoperative adrenal venous sampling (AVS) calculated according to standard practice [12, 21,22,23,24] was collected. Selectivity index for right vein cannulation was >2/>3 without (one centre)/with ACTH stimulation according to local protocol. For analysis of follow-up routines, the complete dataset was used, if data were missing for either analysis of clinical or biochemical success, patients were excluded form that analysis (Fig. 1).

Flow chart, identified patients
Follow-up data were recorded from 1 through 24 months after surgery. If the selected variables were measured multiple times after surgery, the last known data were registered. Regarding antihypertensive medication and potassium supplementation, the names and dosages used pre- and postoperative were collected. Hypertension grade was defined using the European Society of Hypertension Guidelines [25]. In some cases, a deliberate change in antihypertensive medication was carried out to facilitate diagnostic work-up. If so, the registered data were collected before that change was made. Doses of antihypertensive medication or potassium substitution were calculated using defined daily doses (DDD) according to the World Health Organization Anatomical Therapeutic Chemical Index 2018 [26]. AVS lateralisation ratio was registered as cortisol-adjusted lateralisation ratio between the left and right adrenal vein. The Clavien-Dindo classification [27] was used to register surgical complications.
To define the outcome of adrenalectomy, the PASO criteria [20] for clinical and biochemical outcomes was used. Complete clinical success was defined as normal blood pressure without the aid of antihypertensive medication. For partial clinical success, the blood pressure was the same as before surgery but with less antihypertensive medication, or there was a reduction in blood pressure with either the same amount or less antihypertensive medication. Absent clinical success was unchanged or increased blood pressure with either the same amount or an increase in antihypertensive medication. Complete biochemical success was reached when there was a correction of hypokalemia (if present pre-surgery) and normalization of the ARR. In patients with a raised ARR post-surgery, aldosterone secretion should be suppressed in a confirmatory test. Partial biochemical success was defined as correction of hypokalemia and a raised ARR with one or both of the following (compared with pre-surgery); ≥50% decrease in baseline plasma aldosterone concentration, or abnormal but improved post-surgery confirmatory test result. Finally, absent biochemical success was defined as a persistent hypokalemia or persistent raised ARR, or both, with failure to suppress aldosterone secretion with a post-surgery confirmatory test.
Normal distribution was assessed with the Shapiro–Wilks test. Unless otherwise noted, all quantitative normally distributed variables are reported as mean (SD). Not normally distributed quantitative variables are reported as median (range). Categorical variables are presented as absolute numbers and percentages. One-way ANOVA with post hoc Bonferroni analysis was used for quantitative normally distributed variables. The Kruskal–Wallis test was used for non-normally distributed variables. Chi-squared or Fisher’s exact tests were used for categorical variables. IBM SPSS software version 25 was used for all statistical analyses. The study was approved by the regional medical ethics board of Western Sweden (Dnr 086-2017).
Results
In total, 190 patients underwent unilateral adrenalectomy for PA in Sweden between January 2009 and December 2015 according to the SQRTPA. Six different centres were responsible for the treatments. In 19 patients, outcome analysis was impossible as no postoperative medical records could be obtained (14 patients) or incomplete postoperative data regarding blood pressure or use of antihypertensive medication (5 patients) (Fig. 1). Therefore, 171 patients were available for clinical outcome analysis. However, in 75 of these patients (44%), missing data precluded evaluation of biochemical cure according to the PASO criteria (Fig. 1). The cohort of 171 patients included 80 women (47%) and the mean age at the time of surgery was 53 years. Median follow-up time was 3.7 months (range 1.7–9.7). 39 of 171 patients (23%) were registered using mineralocorticoid receptor antagonist (MRA) before surgery. A minimal invasive approach was used in 168/171 patients (98%). Further baseline characteristics are reported in Table 1. The overall complication rate (Clavien-Dindo >3a) was 3%. No mortality was registered.
Preoperatively 168/171 patients (98%) used antihypertensive medication with a mean DDD of 3.7 (range 0–16). Mean (SD) systolic blood pressure (SBP) and diastolic blood pressure (DBP) were 156 (22) and 91(11) mm Hg. After surgery, mean DDD was reduced to 1.5 (range 0–7), whereas mean SBP and DBP decreased to 135 (15) and 84 (10) mm Hg. Regarding potassium supplementation, 89% used it before surgery with a mean DDD of 2.0 (range 0–9). Postoperatively, only 4/170 patients (2%) needed supplementation. Moreover, three of these patients could reduce the number of pills, thus a single patient had to continue with the same amount of potassium supplementation after surgery.
Cure rates according to PASO criteria
Complete clinical success according to the PASO criteria [20] was achieved in 58 (34%) patients, partial success in 103 (60%) patients and absent success in 10 (6%) patients (Table 2). Patients with complete success did not need any antihypertensive medication after surgery, and the mean SBP and DBP were 128 (12) and 82 (9) mm Hg. Before surgery, the same subgroup had a mean blood pressure of 149 (19)/89 (9) mm Hg. Patients with partial success reduced antihypertensive medication mean DDD from 4.4 to 2.0, and the blood pressure was improved from 159 (23)/92 (12) to 136 (15)/84 (9) mm Hg. The mean decrease in DDD was similar (2.4) for patients with complete and partial success (p = 0.92). In patients with absent clinical success, antihypertensive medication use increased from a mean DDD of 3.7 before to 4.3 after surgery. 39 patients (23%) used MRA before surgery and three continued with MRA after surgery. Out of the three patients who continued, two of them had absent clinical success and one of them had partial clinical success. Age, female sex, BMI, preoperative systolic blood pressure, AVS lateralisation index and histologic diagnosis were associated with clinical cure at univariate analysis (see Table 2).
In the total cohort of 171 patients, 75 patients were not eligible for biochemical analysis according to PASO criteria due to lack of postoperative data, especially missing postoperative ARR. Excluding these patients, 96 patients were left with complete data (Fig. 1). In this cohort of 96 patients, complete biochemical success was achieved in 88 (92%) patients, partial success in 7 (7%) patients, and absent success in 1 (1%) patient (Table 3). In the total cohort, 3/169 (2%) patients were registered with hypokalemia after surgery, which correlates with the number of patients in need of postoperative potassium supplementation reported earlier. The only patient with absent biochemical success was also the only patient with bilateral adrenal adenoma.
AVS lateralisation ratio and clinical success according to PASO
Preoperative AVS data were available in 140 patients. Median left-to-right (LR) ratio was 13.2. Median LR ratio was 14.2, 13.3, and 5.7 in patients with complete, partial and absent clinical success, respectively (p = 0.004).
Discussion
This register-based study describes contemporary clinical practice and outcomes of surgery for unilateral dominant PA in Sweden, at short-term follow-up. Interestingly, clinical outcome data could only be obtained for 90% of patients. In 44% of these, evaluation of biochemical success was hampered by lack of uniform reporting of relevant outcome measures. Based on available data, we report a complete clinical success after surgery in 34% of the patients and partial clinical success in 60% of the patients. Thus, only 6% of the patients had no clinical benefit of surgery. Based on the 56% of the total cohort with complete postoperative data regarding biochemical outcome, complete and partial biochemical success was achieved in 92 and 7% of the patients, respectively.
The PASO criteria provide relevant and clinically applicable definitions of both clinical and biochemical outcomes, and the classification system has shown advantages in terms of the ability to stratify outcomes [28], which made it the obvious choice in our study. In this study using quality register data, outcome data were only available for 171 (90%) of patients and of these data on biochemical outcome according to the PASO criteria were only available for 56% (96/171). This probably reflects clinical practice in Sweden during the study period, and may in part be explained by lack of uniform reporting criteria during the study period (2009-2015), the suggested PASO criteria being published in 2017. However, this finding underlines the need for uniform reporting criteria and accountability for all health service systems offering surgery for PA.
Complete clinical success was achieved in 34% after surgery, which is in the lower range of previously published data [14], but almost equivalent with the PASO investigators result at 37% [20]. Compared to the PASO cohort, our patients had a slightly higher preoperative use of antihypertensive medication with a mean DDD of 2.4, compared to 2.0. Other baseline characteristics, for example age and BMI, were similar between studies. In total, 60% had a partial clinical success in our study. This is higher compared to 47% reported in the PASO study, but the baseline characteristics do not display any significant differences between data that can help explain this inequality. Absent clinical success at 6% is much lower compared to the PASO study (16%). In general, use of antihypertensive medication (mean DDD) is higher in our study compared to the PASO study, both in the total cohort and in each subgroup. Factors associated with clinical success in the present study (age, sex, BMI, blood pressure, AVS lateralisation ratio and histologic subtype) correspond with previous studies [19, 20, 29, 30], Unfortunately, we were not able to investigate known duration of hypertension before surgery, due to difficulties in obtaining data.
In this cohort of surgically treated patients, the proportion of patients with preoperative hypokalemia was 89% which is slightly higher than the 74 to 80% [19, 20] reported in other recent surgical series, but notably higher than in series reported from diagnostic units with rates of hypokalemia in PA ranging from 9 to 45% [5, 31]. This suggests that hypokalemia in clinical practice is an important factor in selecting candidates for surgery.
During the study period, the Swedish population above 45 years of age increased from 4.1 to 4.4 million (Statistics Sweden, scb.se). The prevalence of hypertension in the adult population in Sweden has been estimated at 27% [32]. Reported prevalence of PA among Swedish hypertensive patients ranges from 1.4 to 8.5% [33,34,35] in primary health care to 14.5% [33] in dedicated hypertensive care units. Consequently, even a conservative prevalence estimate would indicate some 15 000 individuals with PA in the Swedish adult population. The fact that there are only 190 registered patients in SQRTPA who underwent surgery for PA between 2009 and 2015 suggest that PA is underdiagnosed and undertreated in Sweden.
AVS was performed and registered in 140 patients, and the data display a correlation between lateralisation ratio and clinical outcome. AVS is known to be technically challenging and dependent on the operator [36]. In particular, the right adrenal vein is more difficult to cannulate than the left. Suppressed aldosterone production sampled in a successfully cannulated adrenal vein on a non-dominant side can be used as a predictor of unilateral contralateral disease [37, 38]. The higher proportion of left- compared to right-sided tumours in the present study (63 vs 37%, see Table 1) may reflect these technical difficulties and emphasizes the importance of combining imaging data, clinical data and high volume experience in AVS interpretation for optimal surgical selection.
A strength of the present study is the register-based approach giving an overview of contemporary practice and clinical outcomes in a geographically defined region. Data were validated at each centre, however, some under-reporting to the register may be present, especially in the early part of the study period. Using available real-life follow-up data confers a high validity in the analysis of contemporary follow-up practices. However, missing data limit the interpretation of biochemical outcomes. Another limitation of the study is the relatively short follow-up time of median 3.7 months which may underestimate the clinical success rate [14]. Furthermore, cure rates in adenoma patients may be underestimated as immunohistochemical analysis of aldosterone and cortisol synthase [39] was not routine in Sweden during the study period.
In conclusion, this population-based series continues to show the benefit from surgery for unilateral dominant primary aldosteronism. Complete or partial biochemical and clinical outcomes are high in Sweden at short-term follow-up, and overall complication rate is low. We suggest mandatory reporting of surgical outcomes using the PASO criteria for all units performing surgery for PA.
References
Conn JW (1955) Presidential address. I. Painting background. II. Primary aldosteronism, a new clinical syndrome. J Lab Clin Med 45:3–17
Funder JW, Carey RM, Fardella C et al (2008) Case detection, diagnosis, and treatment of patients with primary aldosteronism: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. https://doi.org/10.1210/jc.2008-0104
Hannemann A, Wallaschofski H (2012) Prevalence of primary aldosteronism in patient’s cohorts and in population-based studies--a review of the current literature. Horm Metab Res 44:157–162. https://doi.org/10.1055/s-0031-1295438
Young WF (2007) Primary aldosteronism: renaissance of a syndrome. Clin Endocrinol (Oxf) 66:607–618. https://doi.org/10.1111/j.1365-2265.2007.02775.x
Douma S, Petidis K, Doumas M et al (2008) Prevalence of primary hyperaldosteronism in resistant hypertension: a retrospective observational study. Lancet. https://doi.org/10.1016/S0140-6736(08)60834-X
Born-Frontsberg E, Reincke M, Rump LC et al (2009) Cardiovascular and cerebrovascular comorbidities of hypokalemic and normokalemic primary aldosteronism: results of the German conn’s registry. J Clin Endocrinol Metab. https://doi.org/10.1210/jc.2008-2116
Savard S, Amar L, Plouin PF, Steichen O (2013) Cardiovascular complications associated with primary aldosteronism: a controlled cross-sectional study. Hypertension. https://doi.org/10.1161/HYPERTENSIONAHA.113.01060
Milliez P, Girerd X, Plouin PF et al (2005) Evidence for an increased rate of cardiovascular events in patients with primary aldosteronism. J Am Coll Cardiol. https://doi.org/10.1016/j.jacc.2005.01.015
Mulatero P, Monticone S, Bertello C et al (2013) Long-term cardio- and cerebrovascular events in patients with primary aldosteronism. J Clin Endocrinol Metab. https://doi.org/10.1210/jc.2013-2805
Rossi GP, Bernini G, Desideri G et al (2006) Renal damage in primary aldosteronism: results of the PAPY study. Hypertension. https://doi.org/10.1161/01.HYP.0000230444.01215.6a
Chao C-T, Wu V-C, Kuo C-C, et al (2013) Diagnosis and management of primary aldosteronism: an updated review. Ann Med 45:375–383. https://doi.org/10.3109/07853890.2013.785234
Funder JW, Carey RM, Mantero F et al (2016) The management of primary aldosteronism: case detection, diagnosis, and treatment: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. https://doi.org/10.1210/jc.2015-4061
Williams TA, Reincke M (2018) MANAGEMENT OF ENDOCRINE DISEASE: Diagnosis and management of primary aldosteronism: the Endocrine Society guideline 2016 revisited. Eur J Endocrinol 179:R19–R29. https://doi.org/10.1530/EJE-17-0990
Muth A, Ragnarsson O, Johannsson G, Wängberg B (2015) Systematic review of surgery and outcomes in patients with primary aldosteronism. Br J Surg 102:307–317. https://doi.org/10.1002/bjs.9744
Proye CAG, Mulliez EAR, Carnaille BML et al (1998) Essential hypertension: first reason for persistent hypertension after unilateral adrenalectomy for primary aldosteronism? Surgery. https://doi.org/10.1067/msy.1998.93108
Sechi LA, Novello M, Lapenna R et al (2006) Long-term renal outcomes in patients with primary aldosteronism. J Am Med Assoc. https://doi.org/10.1001/jama.295.22.2638
Steichen O, Zinzindohoué F, Plouin P-F, Amar L (2012) Outcomes of adrenalectomy in patients with unilateral primary aldosteronism: a review. Horm Metab Res 44:221–227. https://doi.org/10.1055/s-0031-1299681
Rossi GP, Bolognesi M, Rizzoni D et al (2008) Vascular remodeling and duration of hypertension predict outcome of adrenalectomy in primary aldosteronism patients. Hypertension. https://doi.org/10.1161/HYPERTENSIONAHA.108.111369
Vorselaars WMCM, Nell S, Postma EL et al (2019) Clinical outcomes after unilateral adrenalectomy for primary aldosteronism. JAMA Surg. https://doi.org/10.1001/jamasurg.2018.5842
Williams TA, Lenders JWM, Mulatero P et al (2017) Outcomes after adrenalectomy for unilateral primary aldosteronism: an international consensus on outcome measures and analysis of remission rates in an international cohort. Lancet Diabetes Endocrinol 5:689–699. https://doi.org/10.1016/S2213-8587(17)30135-3
Webb R, Mathur A, Chang R et al (2012) What is the best criterion for the interpretation of adrenal vein sample results in patients with primary hyperaldosteronism? Ann Surg Oncol 19:1881–1886. https://doi.org/10.1245/s10434-011-2121-5
Nwariaku FE, Miller BS, Auchus R et al (2006) Primary hyperaldosteronism. Arch Surg 141:497. https://doi.org/10.1001/archsurg.141.5.497
Rossi GP, Barisa M, Allolio B et al (2012) The adrenal vein sampling international study (AVIS) for identifying the major subtypes of primary aldosteronism. J Clin Endocrinol Metab 97:1606–1614. https://doi.org/10.1210/jc.2011-2830
Ragnarsson O, Wängberg B, Muth A et al (2015) [The importance of adrenal vein sampling in primary aldosteronism. Necessary examination for many patients as computed tomography can lead to errors]. Lakartidningen 112:
Mancia G, Fagard R, Narkiewicz K et al (2013) 2013 Practice guidelines for the management of arterial hypertension of the European Society of Hypertension (ESH) and the European Society of Cardiology (ESC): ESH/ESC Task Force for the Management of Arterial Hypertension. J Hypertens 31:1925–1938. https://doi.org/10.1097/HJH.0b013e328364ca4c
Vander Stichele RH, Elseviers MM, Ferech M et al (2004) European surveillance of antimicrobial consumption (ESAC): data collection performance and methodological approach. Br J Clin Pharmacol. https://doi.org/10.1111/j.1365-2125.2004.02164.x
Dindo D, Demartines N, Clavien P-A et al (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213. https://doi.org/10.1097/01.sla.0000133083.54934.ae
Miller BS, Turcu AF, Nanba AT et al (2018) Refining the definitions of biochemical and clinical cure for primary aldosteronism using the primary aldosteronism surgical outcome (PASO) classification system. World J Surg 42:453–463. https://doi.org/10.1007/s00268-017-4311-1
Pasquier L, Kirouani M, Fanget F et al (2017) Assessment of the Aldosteronona resolution score as a predictive resolution score of hypertension after adrenalectomy for aldosteronoma in French patients. Langenbeck’s Arch Surg. https://doi.org/10.1007/s00423-017-1557-x
Zarnegar R, Young WF, Lee J et al (2008) The aldosteronoma resolution score. Ann Surg. https://doi.org/10.1097/sla.0b013e318165c075
Mulatero P, Stowasser M, Loh KC et al (2004) Increased diagnosis of primary aldosteronism, including surgically correctable forms, in centers from five continents. J Clin Endocrinol Metab. https://doi.org/10.1210/jc.2003-031337
Assessment SC on HT (2004) Moderately elevated blood pressure: a systematic review. Swedish Council on Health Technology Assessment (SBU), Stockholm
Sigurjonsdottir HA, Gronowitz M, Andersson O et al (2012) Unilateral adrenal hyperplasia is a usual cause of primary hyperaldosteronism. Results from a Swedish screening study. BMC Endocr Disord. https://doi.org/10.1186/1472-6823-12-17
Westerdahl C, Bergenfelz A, Isaksson A et al (2006) High frequency of primary hyperaldosteronism among hypertensive patients from a primary care area in Sweden. Scand J Prim Health Care. https://doi.org/10.1080/02813430600830931
Westerdahl C, Bergenfelz A, Isaksson A et al (2011) Primary aldosteronism among newly diagnosed and untreated hypertensive patients in a Swedish primary care area. Scand J Prim Health Care. https://doi.org/10.3109/02813432.2011.554015
Jakobsson H, Farmaki K, Sakinis A et al (2018) Adrenal venous sampling: the learning curve of a single interventionalist with 282 consecutive procedures. Diagnostic Interv Radiol. https://doi.org/10.5152/dir.2018.17397
Harvey A, Pasieka JL, Kline G, So B (2012) Modification of the protocol for selective adrenal venous sampling results in both a significant increase in the accuracy and necessity of the procedure in the management of patients with primary hyperaldosteronism. Surgery (United States). https://doi.org/10.1016/j.surg.2012.07.007
Kline GA, Chin A, So B et al (2015) Defining contralateral adrenal suppression in primary aldosteronism: implications for diagnosis and outcome. Clin Endocrinol (Oxf). https://doi.org/10.1111/cen.12669
Volpe C, Hamberger B, Höög A et al (2015) Primary aldosteronism: functional histopathology and long-term follow-up after unilateral adrenalectomy. Clin Endocrinol (Oxf). https://doi.org/10.1111/cen.12645
Acknowledgements
Open access funding provided by University of Gothenburg. This study was supported by research funds at the Department of Surgery, Sahlgrenska University Hospital, Gothenburg, Sweden.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interests or disclosures.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Sellgren, F., Koman, A., Nordenström, E. et al. Outcomes After Surgery for Unilateral Dominant Primary Aldosteronism in Sweden. World J Surg 44, 561–569 (2020). https://doi.org/10.1007/s00268-019-05265-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-019-05265-8