
Abstract
Background
A recent study demonstrated remarkable discrepancy between the relapse-free survival (RFS) and overall survival (OS) after pulmonary metastasectomy (PM) in the current era. As the RFS may not be a suitable parameter after PM, a more suitable parameter is needed for PM as a surrogate marker for OS.
Methods
A total of 134 consecutive patients who underwent PM were retrospectively analyzed. In the present study, we introduced a new endpoint, time to local treatment failure (TLTF). This endpoint was defined as the time interval between the first PM and the first untreatable recurrence by local treatment with curative intent or death due to any cause. We analyzed the correlation between the RFS and OS and between the TLTF and OS to validate whether or not the TLTF is a better parameter than the RFS after PM.
Results
Thus far, 78 patients have experienced relapse. Of these, 37 patients (47%) underwent local therapy with curative intent, 29 of whom are alive without local treatment failure. The 5-year OS, RFS and TLTF were 70.9%, 36.5%, and 57.6%, respectively. The concordance proportions for the RFS and OS and for the TLTF and OS were 0.634 and 0.851 for all patients, respectively. The Spearman’s rank correlation coefficient for the RFS and OS was 0.639, while that for the TLTF and OS was 0.875.
Conclusions
The TLTF may be a good surrogate parameter for the OS after PM in the current era.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pulmonary metastasectomy (PM) is an established therapy for pulmonary metastasis from various types of tumors [1,2,3,4]. Since the first report about PM by Thomford et al. [5], the indications for PM have been discussed. Kondo et al. summarized the principle criteria for the indication of PM in the current era. In brief, when a patient has a good general condition and the primary disease or other metastatic disease are resected/controlled, the pulmonary metastases which are deemed completely resectable are indicated for PM [6]. The outcomes of PM are conventionally expressed by the relapse-free survival (RFS) (also called the disease-free survival or progression-free survival [PFS] in this field) and the overall survival (OS).
A recent study revealed a remarkable discrepancy between the RFS and OS after PM for pulmonary metastasis from CRC in the current era. In our institute, the RFS curve and OS curve after PM for pulmonary metastasis from CRC were similar in patients who underwent PM before 2002, while a remarkable discrepancy was noted between the RFS and OS in patients who underwent PM after 2003 [7]. This discrepancy means that patients who experienced relapse after the first PM survive longer in the current era than in the past. Possible reasons for this discrepancy between the RFS and OS in the current era are as follows: First, the rate of patients who undergo local therapy with curative intent, including repeat PM for relapse after the first PM, is increasing [7, 8]. Second, if patients do not receive local therapy with curative intent for the relapse after the first PM, the survival time is prolonged thanks to advancements in systemic therapy in the current era. These advancements for recurrent diseases are not limited to CRC. Repeat PM procedures are performed in various types of tumors [9,10,11,12], and systemic therapy for different tumors is also advancing [13,14,15]. Therefore, the discrepancy between the RFS and OS is likely not limited to CRC.
Considering the phenomenon discussed above, the RFS is not a suitable parameter after PM, and a more suitable one is needed, both as a marker for the effectiveness of PM and as a surrogate marker for the OS. Recently, a remarkable report on this issue was published by surgeons managing hepatic metastases from CRC. Oba et al. proposed a new potential surrogate endpoint, called time to surgical failure (TSF) after hepatectomy [16]. The TSF was defined as the time until unresectable relapse or death. They concluded that the correlation between the TSF and the OS was stronger than that between the RFS and the OS after curative hepatic resection in patients with hepatic metastases from CRC. We expand this concept and herein propose a new endpoint after PM: the time to local therapy failure (TLTF). This endpoint is defined as the time interval between the first PM and the first untreatable recurrence by local therapy with curative intent or death due to any cause.
In the present study, we analyzed the correlation between the RFS and OS and the TLTF and OS in order to validate whether or not the TLTF is a better parameter after PM than the RFS after PM in the current era.
Patients and methods
Patients and treatment
The present study was a retrospective analysis of 134 consecutive patients who underwent complete resection of pulmonary metastasis in our hospital between 2010 and 2016. The study protocol was approved by the Ethical Review Board for Clinical Studies at Osaka University (control number 18373).
Patients with pulmonary metastasis from lung cancer were excluded from this study because it is often difficult to distinguish second primary lung cancer from pulmonary metastasis following primary lung cancer. When pulmonary metastasis from various tumors was detected, the treatment strategy was decided by the cancer board of our hospital.
The patients who met the following criteria underwent pulmonary metastasis as previously described [7]: (1) the pulmonary nodule was deemed completely resectable; (2) apparent mediastinal lymph node metastasis was absent on a preoperative radiological examination; (3) the metastatic disease was limited to the lungs, or extrapulmonary distant metastasis was controlled or controllable if present; (4) locoregional control of the primary tumor was achieved; and (5) the patient had a good overall general condition, and their respiratory function was sufficient to tolerate lung resection.
The type of resection was selected according to the size and location of the tumor, the overall general condition, and the respiratory function of the patient; lesser resection was preferably selected as long as curative resection was possible as previously described [7]. In terms of the surgical approach, video-assisted thoracoscopic surgery (VATS) was the first choice. Thoracotomy was selected when the preoperative computed tomography (CT) findings suggested that the palpation of the nodule during surgery was necessary for detecting the pulmonary nodule or ensuring a sufficient margin. All of the specimens obtained from pulmonary resection were reviewed by pathologists.
The treatment strategy for re-recurrence after the first PM was decided by the department in which the primary tumor was treated. Repeat PM was proactively performed for recurrent disease with pulmonary metastasis alone [8, 9]. Local treatment with curative intent for recurrence besides lung was decided based on both the general condition of the patients and the number of metastases.
Follow-up was generally based on the findings from chest CT, a physical examination, and laboratory blood tests performed every 6–12 months after treatment. Follow-up information was obtained from the hospital medical records. The time interval between pulmonary resection and the latest follow-up in the present study ranged from 1 to 99 months (median 36 months, mean 44 months).
Definitions of the survival
The OS was defined as the time interval between the first PM and death by any cause, while the RFS was defined as the time interval between the first PM and the first recurrence of primary tumor cancer or death due to any cause. In the present study, we introduced a new endpoint: the TLTF, defined as the time interval between the first PM and the first untreatable recurrence by local treatment with curative intent or death due to any cause (Fig. 1).

Associations between each time-to-event (RFS, TLTF, and OS) in the time course of patients who underwent pulmonary metastasectomy. The TLTF was defined as the time interval between the first PM and the first untreatable recurrence by local treatment with curative intent or death due to any cause. BSC best supportive care, LT local therapy, OS overall survival, PM pulmonary metastasectomy, RFS relapse-free survival, TLTF time to local treatment failure
Statistical analyses
The follow-up and survival periods were estimated using the Kaplan–Meier method. Surviving patients were censored at the time of the last follow-up. The correlations between the RFS and OS events and between the TLTF and OS events were each evaluated using the concordance proportion, as previously described [16]. Spearman’s rank correlation coefficient was used to estimate the correlations between the survival function of the RFS and OS and between the survival function of the TLTF and OS, as predicted using the Cox proportional hazards model in all patients. The statistical analyses were conducted using JMP Pro 13 and SAS 9.4 SAS/STAT 14.3 software programs (SAS Institute, Berkley, CA, USA).
Results
The characteristics of the patients in the two groups are shown in Table 1. The mean age of the patients was 59.1 years. The most frequent type of primary tumor was CRC (n = 50, 37%) followed by soft tissue sarcoma/osteosarcoma (n = 19, 14%) and gynecologic malignancies (n = 16, 12%).
Surgical factors are described in Table 2. One hundred and seven patients (80%) underwent video-assisted thoracic surgery (VATS), and 107 patients (80%) underwent sublobar resection. Lymph node metastasis was pathologically confirmed in 6 patients (4%). Postoperative therapy was performed in 41 patients (31%). Regimens of postoperative therapy are also shown in Table 2.
Thus far, 78 patients have experienced relapse. The sites of relapse were the lung alone in 29 (37%), other sites besides the lung and primary tumor or regional lymph nodes in 22 (28%), lung and other sites in 11 (14%), pleura in 6 (8%), mediastinal lymph nodes in 4 (5%), local relapse of primary tumor or regional lymph nodes in 4 (5%), and surgical margin relapse of pulmonary metastasis in 2 (3%). The clinical course after the first PM is shown in Fig. 2. Of the 78 patients who experienced relapse, 37 (47%) underwent local therapy with curative intent, 21 underwent repeat pulmonary resection, 9 underwent surgery for other organs besides the lung, 6 underwent radiotherapy, and 1 underwent chemoradiotherapy. Of these, 29 patients remain alive without local treatment failure.

The clinical course after the first PM. PM pulmonary metastasectomy, RFA radiofrequency ablation
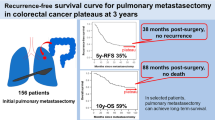
The 5-year OS, RFS, and TLTF were 70.9%, 36.5%, and 57.6%, respectively (Fig. 3). Table 3 shows the concordance proportions for RFS and OS, and TLTF and OS, and Spearman’s rank correlation coefficient for RFS and OS, and TLTF and OS in each patient group [all patients (n = 134), colorectal cancer (n = 50), carcinoma (n = 105), and sarcoma (n = 22)]. These results show that the correlation between TLTF and OS was stronger than that between RFS and the OS in all patient groups.

Kaplan–Meier plots of the RFS, TLTF, and OS in all patients (n = 134). OS overall survival, RFS relapse-free survival, TLTF time to local treatment failure
Discussion
The present study showed that the correlation between the TLTF and the OS was stronger than that between the RFS and the OS. The TLTF may be a good surrogate parameter for the OS after PM in the current era.
Local therapy with curative intent, including repeat PM, stereotactic radiotherapy, and radiofrequency ablation, is increasingly frequently indicated for relapse after initial PM in the current era [9,10,11,12, 17,18,19]. In our recent report, the rate of patients who received local therapy with curative intent for isolated relapses was significantly higher in patients treated after 2003 than in those treated before 2003 who underwent PM for CRC (64% vs 31%, p = 0.04) [7]. When patients underwent successful local therapy for relapse after the first PM, they were free from disease, and a proportion achieved a survival without disease. The presence of these patients subsequently results in a discrepancy between the RFS and OS. In the present study, of the 78 patients who experienced relapse after the first PM, 37 (47%) underwent local therapy with curative intent. Of those patients, 29 remain alive without local therapy failure. Therefore, a remarkable discrepancy between the RFS and the OS is observed (concordance proportion 0.634, Spearman’s rank correlation coefficient 0.639).
Some authors have noted that there is a discrepancy between the RFS and the OS after resection of metastatic diseases. Matsuguma et al. proposed the modified PFS [10]. In that parameter, when the disease-free status continues for longer than 2 years after repeated resection at the last follow-up, the first recurrence is not considered an event. The authors analyzed the outcomes of patients who underwent PM for urinary transitional cell carcinoma, and the 5-year OS and PFS rates were 50% and 26%, respectively, including 3 patients who underwent a second PM for recurrence, 9 patients survived without recurrence for more than 5 years, resulting in a modified 5-year PFS rate of 40%. Therefore, the modified PFS is considered to represent the effects of PM well. However, while the modified PFS seems like a useful parameter, the limitation is that the judge of timing should be 2 years after the repeat PM. This parameter can therefore only be applied in retrospective reviews, not for patients who might undergo repeat PM in the future.
In the present study, we demonstrated that the correlation between the TLTF and the OS was stronger than that between the RFS and the OS in patients who underwent PM for pulmonary metastases from various tumors. The results from the total patients, CRC, carcinoma, and sarcoma have the same tendency. The differences between the TSF proposed by Oba et al. [16] and the TLTF are as follows: local therapy for relapse after the first resection for metastasis is not limited to surgery in TLTF, and the type of tumor is not limited to CRC. However, despite these minor differences, the concepts are similar and seem to be viable in both fields.
Two points concerning the newly proposed endpoint of TLTF should be noted. First, the TLTF is a parameter concerning the effectiveness of PM. Second, the TLTF is a surrogate marker for the OS. Recently, stereotactic body radiation therapy (SBRT) has come to be widely performed for the treatment of pulmonary metastasis, and provides a favorable local control rate. Some radiation oncologists use “freedom from failure of local control,” which is similar to TLTF, as an endpoint for SBRT for pulmonary metastasis [19]. We believe that TLTF will be useful in studies comparing pulmonary metastasectomy and SBRT. On the other hand, it is difficult to validate the effectiveness of PM, partly because a large proportion of patients receive systemic therapy before and/or after PM, and the effects of such therapy and PM cannot be completely distinguished. Therefore, the TLTF is actually considered to reflect the effects of multidisciplinary treatment, including PM. However, the prediction of the prognosis is important for preparing for palliative treatment in cases requiring terminal care [20]. The present study showed that the TLTF correlates well with the OS, suggesting that it may be useful for predicting the prognosis.
Several limitations associated with the present study warrant mention. First, this was a single-institution study, and the number of patients was limited. There may be differences among physicians or institutions concerning the criteria for deciding whether or not local therapy with curative intent is indicated for relapse after the first PM. Therefore, the TLTF may not correlate with the OS well in other institutions. This point should be analyzed at another institution or in a multi-institutional setting. Second, the present study was a retrospective study. The usefulness of the TLTF must therefore be validated in a prospective cohort in the future.
References
Higashiyama M, Tokunaga T, Nakagiri T et al (2015) Pulmonary metastasectomy: outcomes and issues according to the type of surgical resection. Gen Thorac Cardiovasc Surg 63:320–330
Kanzaki R, Higashiyama M, Fujiwara A et al (2010) Outcome of surgical resection of pulmonary metastasis from urinary tract transitional cell carcinoma. Interact CardioVasc Thorac Surg 11:60–64
Kanzaki R, Inoue M, Minami M et al (2014) Surgery for pulmonary malignancies in patients with a previous history of head and neck squamous cell carcinoma. Surg Today 44:646–652
Kanzaki R, Kimura T, Kawamura T et al (2017) Surgery for malignant pulmonary nodules in patients with a history of oesophageal cancer. Interact CardioVasc Thorac Surg 24:418–424
Thomford NR, Woolner LB, Clagett OT (1965) The surgical treatment of metastatic tumors in the lungs. J Thorac Cardiovasc Surg 49:357–363
Kondo H, Okumura T, Ohde Y et al (2005) Surgical treatment for metastatic malignancies. Pulmonary metastasis: indications and outcomes. Int J Clin Oncol 10:81–85
Kanzaki R, Inoue M, Kimura T et al (2017) Role of pulmonary metastasectomy in colorectal cancer in the era of modern multidisciplinary therapy. Surg Today 47:1111–1118
Kanzaki R, Higashiyama M, Oda K et al (2011) Outcome of surgical resection for recurrent pulmonary metastasis from colorectal carcinoma. Am J Surg 202:419–426
Kanzaki R, Higashiyama M, Fujiwara A et al (2011) Long-term results of surgical resection for pulmonary metastasis from renal cell carcinoma: a 25-year single-institution experience. Eur J Cardio Thorac Surg 39:167–172
Matsuguma H, Yoshino I, Ito H et al (2011) Is there a role for pulmonary metastasectomy with a curative intent in patients with metastatic urinary transitional cell carcinoma? Ann Thorac Surg 92:449–453
Chudgar NP, Brennan MF, Tan KS et al (2017) Is repeat pulmonary metastasectomy indicated for soft tissue sarcoma? Ann Thorac Surg 104:1837–1845
Treasure T, Mineo T, Ambrogi V et al (2015) Survival is higher after repeat lung metastasectomy than after a first metastasectomy: too good to be true? J Thorac Cardiovasc Surg 149:1249–1252
Signoretti S, Flaifel A, Chen Y-B et al (2018) Renal cell carcinoma in the era of precision medicine: from molecular pathology to tissue-based biomarkers. J Clin Oncol 36:3553–3559
Abufaraj M, Dalbagni G, Daneshmand S et al (2018) The role of surgery in metastatic bladder cancer: a systematic review. Eur Urol 73:543–557
Martin-Liberal J, Perez E, Garcia Del Muro X (2019) Investigational therapies in phase II clinical trials for the treatment of soft tissue sarcoma. Expert Opin Investig Drugs 28:39–50
Oba M, Hasegawa K, Matsuyama Y et al (2014) Discrepancy between recurrence-free survival and overall survival in patients with resectable colorectal liver metastases: a potential surrogate endpoint for time to surgical failure. Ann Surg Oncol 21:1817–1824
Hasegawa H, Ninomiya M, Honbou T et al (2011) A case of long-term survival by combined modality therapy for liver and pulmonary metastasis of rectal cancer. Jpn J Cancer Chemother 38:2310–2312
Hiraki T, Gobara H, Iguchi T et al (2014) Radiofrequency ablation as treatment for pulmonary metastasis of colorectal cancer. World J Gastroenterol 20:988–996
Lodeweges JE, Klinkenberg TJ, Ubbels JF et al (2017) Long-term outcome of surgery or stereotactic radiotherapy for lung oligometastases. J Thorac oncol 12:1442–1445
Gwilliam B, Keeley V, Todd C et al (2015) Development of prognosis in palliative care study (PiPS) predictor models to improve prognostication in advanced cancer: prospective cohort study. BMJ Support Palliat Care 5:390–398
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest in association with the present study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Kanzaki, R., Kanou, T., Ose, N. et al. Proposal of a Useful Surrogate Endpoint of the Overall Survival in Patients Undergoing Pulmonary Metastasectomy: The Time to Local Therapy Failure. World J Surg 43, 2640–2646 (2019). https://doi.org/10.1007/s00268-019-05071-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-019-05071-2