
Abstract
Background
The main limiting factor for major liver resections is the volume and function of the future remnant liver (FLR). Portal vein embolization (PVE) is now standard in most centers for preoperative hypertrophy of FLR. However, it has a failure rate of about 20–30 %. In these cases, the “Associating Liver Partition and Portal Vein Ligation for Staged Hepatectomy” (ALPPS) may represent a suitable and possibly the only alternative.
Methods
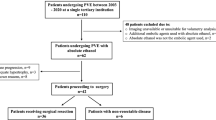
We performed a retrospective analysis of nine patients who had ALPPS following an insufficient hypertrophy after PVE. Computed tomography volumetry were performed before and after PVE as well as the first step of ALPPS. Furthermore, complications, 30-day mortality and outcome were analyzed.
Results
The FLR volume rose significantly by 77.7 ± 40.7 % (FLR/TLV: 34.9 ± 9.7 %) as early as 9 days after the first stage despite insufficient hypertrophy after preoperative portal vein embolization. Major complications (Grade > IIIb) occurred in 33 % of the patients, and 30-day mortality was 11.1 %. The OS at 1 and 2 years was 78 and 44 %. Four patients are presently still alive at a median of 33.4 (range 15–48) months (survival rate 44.4 %).
Conclusion
The ALPPS procedure could be a suitable alternative for patients following insufficient PVE or indeed the last chance of a potentially curative treatment in this situation. Nevertheless, the high morbidity and mortality rates and the lack of data on the long-term oncological outcome must also be taken into account.


Similar content being viewed by others


References
Agrawal S, Belghiti J (2011) Oncologic resection for malignant tumors of the liver. Ann Surg 253:656–665
Clavien PA, Petrowsky H, DeOliveira ML, Graf R (2007) Strategies for safer liver surgery and partial liver transplantation. N Engl J Med 356:1545–1559
Lam VW, Spiro C, Laurence JM, Johnston E, Hollands MJ, Pleass HC, Richardson AJ (2012) A systematic review of clinical response and survival outcomes of downsizing systemic chemotherapy and rescue liver surgery in patients with initially unresectable colorectal liver metastases. Ann Surg Oncol 19:1292–1301
Makuuchi M, Thai BL, Takayasu K, Takayama T, Kosuge T, Gunvén P et al (1990) Preoperative portal embolization to increase safety of major hepatectomy for hilar bile duct carcinoma: a preliminary report. Surgery 107:521–527
Azoulay D, Castaing D, Krissat J, Smail A, Hargreaves GM, Lemoine A et al (2000) Percutaneous portal vein embolization increases the feasibility and safety of major liver resection for hepatocellular carcinoma in injured liver. Ann Surg 232:665–672
Adam R, Laurent A, Azoulay D, Castaing D, Bismuth H (2000) Two-stage hepatectomy: a planned strategy to treat irresectable liver tumors. Ann Surg 232:777–785
Jaeck D, Oussoultzoglou E, Rosso E, Greget M, Weber JC, Bachellier P (2004) A two-stage hepatectomy procedure combined with portal vein embolization to achieve curative resection for initially unresectable multiple and bilobar colorectal liver metastases. Ann Surg 240:1037–1049 (discussion 1049–51)
van Lienden KP, van den Esschert JW, de Graaf W, Bipat S, Lameris JS, van Gulik TM, van Delden OM (2013) Portal vein embolization before liver resection: a systematic review. Cardiovasc Intervent Radiol 36:25–34
Wicherts DA, Miller R, de Haas RJ, Bitsakou G, Vibert E, Veilhan LA et al (2008) Long-term results of two-stage hepatectomy for irresectable colorectal cancer liver metastases. Ann Surg 248:994–1005
Schnitzbauer AA, Lang SA, Goessmann H, Nadalin S, Baumgart J, Farkas SA et al (2012) Right portal vein ligation combined with in situ splitting induces rapid left lateral liver lobe hypertrophy enabling 2-staged extended right hepatic resection in small-for-size settings. Ann Surg 255:405–414
de Santibañes E, Clavien PA (2012) Playing Play-Doh to prevent postoperative liver failure: the “ALPPS” approach. Ann Surg 255:415–417
Khan AZ, Morris-Stiff G, Makuuchi M (2009) Patterns of chemotherapy-induced hepatic injury and their implications for patients undergoing liver resection for colorectal liver metastases. J Hepatobiliary Pancreat Surg 16:137–144
Lehmann K, Rickenbacher A, Weber A, Pestalozzi BC, Clavien PA (2012) Chemotherapy before liver resection of colorectal metastases: friend or foe? Ann Surg 255:237–247
van der Vorst JR, van Dam RM, van Stiphout RS, van den Broek MA, Hollander IH, Kessels AG, Dejong CH (2010) Virtual liver resection and volumetric analysis of the future liver remnant using open source image processing software. World J Surg 34:2426–2433
Lang SA, Loss M, Schlitt HJ (2013) “In-situ Split” (ISS) liver resection: new aspects of technique and indication. Zentralbl Chir 139:212–219
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Balzan S, Belghiti J, Farges O, Ogata S, Sauvanet A, Delefosse D, Durand F (2005) The, “50–50 criteria” on postoperative day 5: an accurate predictor of liver failure and death after hepatectomy. Ann Surg 242:824–828 (discussion 828–9)
Kinoshita H, Sakai K, Hirohashi K, Igawa S, Yamasaki O, Kubo S (1986) Preoperative portal vein embolization for hepatocellular carcinoma. World J Surg 10:803–808
de Graaf W, van Lienden KP, van den Esschert JW, Bennink RJ, van Gulik TM (2011) Increase in future remnant liver function after preoperative portal vein embolization. Br J Surg 98:825–834
Abulkhir A, Limongelli P, Healey AJ, Damrah O, Tait P, Jackson J et al (2008) Preoperative portal vein embolization for major liver resection: a meta-analysis. Ann Surg 247:49–57
Kishi Y, Madoff DC, Abdalla EK, Palavecino M, Ribero D, Chun YS, Vauthey JN (2008) Is embolization of segment 4 portal veins before extended right hepatectomy justified? Surgery 144:744–751
Nagino M, Kanai M, Morioka A, Yamamoto H, Kawabata Y, Hayakawa N, Nimura Y (2000) Portal and arterial embolization before extensive liver resection in patients with markedly poor functional reserve. J Vasc Interv Radiol 11:1063–1068
Kokudo N, Tada K, Seki M, Ohta H, Azekura K, Ueno M et al (2001) Proliferative activity of intrahepatic colorectal metastases after preoperative hemihepatic portal vein embolization. Hepatology 34:267–272
Shindoh J, Vauthey J-N, Zimmitti G, Curley SA, Huang SY, Mahvash A et al (2013) Analysis of the efficacy of portal vein embolization for patients with extensive liver malignancy and very low future liver remnant volume, including a comparison with the associating liver partition with portal vein ligation for staged hepatectomy approach. J Am Coll Surg 217:126–133
de Graaf W, van den Esschert JW, van Lienden KP, van Gulik TM (2009) Induction of tumor growth after preoperative portal vein embolization: is it a real problem? Ann Surg Oncol 16:423–430
Elias D, De Baere T, Roche A, Ducreux M, Leclere J, Lasser P (1999) During liver regeneration following right portal embolization the growth rate of liver metastases is more rapid than that of the liver parenchyma. Br J Surg 86:784–788
Heinrich S, Jochum W, Graf R, Clavien PA (2006) Portal vein ligation and partial hepatectomy differentially influence growth of intrahepatic metastasis and liver regeneration in mice. J Hepatol 45:35–42
Wicherts DA, de Haas RJ, Andreani P, Sotirov D, Salloum C, Castaing D et al (2010) Impact of portal vein embolization on long-term survival of patients with primarily unresectable colorectal liver metastases. Br J Surg 97:240–250
Alvarez FA, Ardiles V, de Santibañes E (2013) The ALPPS approach for the management of colorectal carcinoma liver metastases current colorectal cancer reports 9:168–177
Schadde E, Ardiles V, Slankamenac K, Tschuor C, Sergeant G, Amacker N et al (2014) ALPPS offers a better chance of complete resection in patients with primarily unresectable liver tumors compared with conventional-staged hepatectomies: results of a multicenter analysis. World J Surg 38:1510–1519
de Santibañes E, Alvarez FA, Ardiles V (2012) How to avoid postoperative liver failure: a novel method. World J Surg 36:125–128
Knoefel WT, Gabor I, Rehders A, Alexander A, Krausch M, Schulte am Esch J et al (2013) In situ liver transection with portal vein ligation for rapid growth of the future liver remnant in two-stage liver resection. Br J Surg 100:388–394
Nadalin S, Capobianco I, Li J, Girotti P, Königsrainer I, Königsrainer A (2014) Indications and limits for associating liver partition and portal vein ligation for staged hepatectomy (ALPPS). Lessons learned from 15 cases at a single centre. Z Gastroenterol 52:35–42
Hernandez-Alejandro R, Bertens KA, Pineda-Solis K, Croome KP (2015) Can we improve the morbidity and mortality associated with the associating liver partition with portal vein ligation for staged hepatectomy (ALPPS) procedure in the management of colorectal liver metastases? Surgery 157:194–201
Truant S, Scatton O, Dokmak S, Regimbeau JM, Lucidi V, Laurent A et al (2015) Associating liver partition and portal vein ligation for staged hepatectomy (ALPPS): impact of the inter-stages course on morbi-mortality and implications for management. Eur J Surg Oncol 41:674–682
Schlegel A, Lesurtel M, Melloul E, Limani P, Tschuor C, Graf R et al (2014) ALPPS: from human to mice highlighting accelerated and novel mechanisms of liver regeneration. Ann Surg 260:839–846 (discussion 846–7)
Dokmak S, Belghiti J (2012) Which limits to the “ALPPS” approach? Ann Surg 256:e6 (author reply e16–e6; author reply e17)
Kokudo N, Shindoh J (2013) How can we safely climb the ALPPS? Updates Surg 65:175–177
Schadde E, Ardiles V, Robles-Campos R, Malago M, Machado M, Hernandez-Alejandro R et al (2014) Early survival and safety of ALPPS: first report of the international ALPPS registry. Ann Surg 260:829–838
Brouquet A, Abdalla EK, Kopetz S, Garrett CR, Overman MJ, Eng C et al (2011) High survival rate after two-stage resection of advanced colorectal liver metastases: response-based selection and complete resection define outcome. J Clin Oncol 29:1083–1090
Alvarez FA, Ardiles V, de Santibañes M, Pekolj J, de Santibañes E (2015) Associating liver partition and portal vein ligation for staged hepatectomy offers high oncological feasibility with adequate patient safety: a prospective study at a single center. Ann Surg 261:723–732
Petrowsky H, Györi G, de Oliveira M, Lesurtel M, Clavien PA (2015) Is partial-ALPPS safer than ALPPS? A single-center experience. Ann Surg 261:e90–e92
Oldhafer KJ, Donati M, Jenner RM, Stang A, Stavrou GA (2013) ALPPS for patients with colorectal liver metastases: effective liver hypertrophy, but early tumor recurrence. World J Surg 38:1504–1509
Schadde E, Schnitzbauer AA, Tschuor C, Raptis DA, Bechstein WO, Clavien PA (2014) Systematic review and meta-analysis of feasibility, safety, and efficacy of a novel procedure: associating liver partition and portal vein ligation for staged hepatectomy. Ann Surg Oncol 22:3109–3120
Lam VW, Laurence JM, Johnston E, Hollands MJ, Pleass HC, Richardson AJ (2013) A systematic review of two-stage hepatectomy in patients with initially unresectable colorectal liver metastases. HPB (Oxford) 15:483–491
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors reported no conflicts of interest.
Rights and permissions
About this article

Cite this article
Ulmer, T.F., de Jong, C., Andert, A. et al. ALPPS Procedure in Insufficient Hypertrophy After Portal Vein Embolization (PVE). World J Surg 41, 250–257 (2017). https://doi.org/10.1007/s00268-016-3662-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-016-3662-3