
Abstract
Background
The surgical resection of huge hepatocellular carcinoma (HCC) is still controversial. This study was designed to introduce our experience of liver resection for huge HCC and evaluate the safety and outcomes of hepatectomy for huge HCC.
Methods
A total of 258 hepatic resections for the patients with huge HCC were analysed retrospectively from December 2002 to December 2011. The operative outcomes were compared with 293 patients with HCC >5.0 cm but <10.0 cm in diameter. Prognostic factors for long-term survival were evaluated by univariate and multivariate analyses.
Results
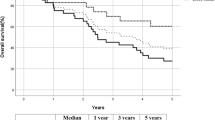
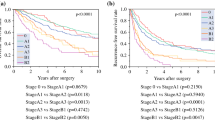
The 1-, 3-, 5-year overall survival rates after liver resection were 84, 62, and 33 %. Overall survival and disease-free survival in huge HCC group and HCC >5.0 cm but <10.0 cm group were similar (P = 0.751, P = 0.493). Solitary huge HCC group has significantly a more longer overall and disease-free survival time than nodular huge HCC (P = 0.026, P = 0.022). Univariate and multivariate analysis revealed that the types of tumour, vascular invasion, and UICC stage were independent prognostic factors for overall survival (P = 0.047, P = 0.037, P = 0.033).
Conclusions
Hepatic resection can be performed safely for huge HCC with a low mortality and favorable survival outcomes. Solitary huge HCC has the better surgical outcomes than nodular huge HCC.

Similar content being viewed by others

References
Jemal A, Bray F, Center MM et al (2011) Global cancer statistics. CA: Cancer J Clin 61:69–90
El-Serag HB (2011) Hepatocellular carcinoma. N Engl J Med 365:1118–1127
Poon RT, Fan ST, Lo CM et al (2002) Long-term survival and pattern of recurrence after resection of small hepatocellular carcinoma in patients with preserved liver function: implications for a strategy of salvage transplantation. Ann Surg 235:373–382
Abdalla EK, Denys A, Hasegawa K et al (2008) Treatment of large and advanced hepatocellular carcinoma. Ann Surg Oncol 15:979–985
Lo CM, Ngan H, Tso WK et al (2002) Randomized controlled trial of transarterial lipiodol chemoembolization for unresectable hepatocellular carcinoma. Hepatology 35:1164–1171
Takayasu K, Arii S, Ikai I et al (2006) Prospective cohort study of transarterial chemoembolization for unresectable hepatocellular carcinoma in 8510 patients. Gastroenterology 131:461–469
Shah SA, Wei AC, Cleary SP et al (2007) Prognosis and results after resection of very large (≥10 cm) hepatocellular carcinoma. J Gastrointest Surg 11:589–595
Liau KH, Ruo L, Shia J et al (2005) Outcome of partial hepatectomy for large (>10 cm) hepatocellular carcinoma. Cancer 104:1948–1955
Hanazaki K, Kajikawa S, Shimozawa N et al (2002) Hepatic resection for hepatocellular carcinoma in diameter of >10 or =10 cm. Hepatogastroenterology 49:518–523
Yang LY, Fang F, Ou DP et al (2009) Solitary large hepatocellular carcinoma: a specific subtype of hepatocellular carcinoma with good outcome after hepatic resection. Ann Surg 249:118–123
Wang W, Yang LY, Huang GW et al (2004) Genomic analysis reveals Rhoc as a potential marker in hepatocellular carcinoma with poor prognosis. Br J Cancer 90:2349–2355
Fan ST, Lai EC, Lo CM et al (1995) Hospital mortality of major hepatectomy for hepatocellular carcinoma associated with cirrhosis. Arch Surg 130:198–203
Lam CM, Fan ST, Lo CM et al (1999) Major hepatectomy for hepatocellular carcinoma in patients with an unsatisfactory indocyanine green clearance test. Br J Surg 86:1012–1017
Imamura H, Sano K, Sugawara Y et al (2005) Assessment of hepatic reserve for indication of hepatic resection: decision tree incorporating indocyanine green test. J Hepatobil Pancreat Surg 12:16–22
Kubota K, Makuuchi M, Kusaka K et al (1997) Measurement of liver volume and hepatic functional reserve as a guide to decision-making in resectional surgery for hepatic tumors. Hepatology 26:1176–1181
Shi J, Lai EC, Li N et al (2010) Surgical treatment of hepatocellular carcinoma with portal vein tumor thrombus. Ann Surg Oncol 17:2073–2080
Kondo K, Chijiiwa K, Kai M et al (2009) Surgical strategy for hepatocellular carcinoma patients with portal vein tumor thrombus based on prognostic factors. J Gastrointest Surg 13:1078–1083
Wang CC, Jawade K, Yap AQ et al (2010) Resection of large hepatocellular carcinoma using the combination of liver hanging maneuver and anterior approach. World J Surg 34:1874–1878. doi:10.1007/s00268-010-0546-9
Wu TJ, Wang F, Lin YS et al (2010) Right hepatectomy by the anterior method with liver hanging versus conventional approach for large hepatocellular carcinomas. Br J Surg 97:1070–1078
Pawlik TM, Delman KA, Vauthey JN et al (2005) Tumor size predicts vascular invasion and histologic grade: implications for selection of surgical treatment for hepatocellular carcinoma. Liver Transplant 11:1086–1092
Wu F, Yang LY, Li YF et al (2009) Novel role for epidermal growth factor-like domain 7 in metastasis of human hepatocellular carcinoma. Hepatology 50:1839–1850
Fang F, Chang RM, Yang LY (2012) Heat shock factor 1 promotes invasion and metastasis of hepatocellular carcinoma in vitro and in vivo. Cancer 118:1782–1794
Fang F, Yang LY, Tao Y et al (2012) FBI-1 promotes cell proliferation and enhances resistance to chemotherapy of hepatocellular carcinoma in vitro and in vivo. Cancer 118:134–146
Yang LY, Tao YM, Ou DP et al (2006) Increased expression of Wiskott-Aldrich syndrome protein family verprolin-homologous protein 2 correlated with poor prognosis of hepatocellular carcinoma. Clin Cancer Res 12:5673–5679
Pawlik TM, Poon RT, Abdalla EK et al (2005) Critical appraisal of the clinical and pathologic predictors of survival after resection of large hepatocellular carcinoma. Arch Surg 140:450–457
Schindl MJ, Redhead DN, Fearon KC et al (2005) The value of residual liver volume as a predictor of hepatic dysfunction and infection after major liver resection. Gut 54:289–296
Gruttadauria S, Vasta F, Minervini MI et al (2005) Significance of the effective remnant liver volume in major hepatectomies. Am Surg 71:235–240
Shi M, Guo RP, Lin XJ et al (2007) Partial hepatectomy with wide versus narrow resection margin for solitary hepatocellular carcinoma: a prospective randomized trial. Ann Surg 245:36–43
Yeh CN, Lee WC, Chen MF (2003) Hepatic resection and prognosis for patients with hepatocellular carcinoma larger than 10 cm: two decades of experience at Chang Gung memorial hospital. Ann Surg Oncol 10:1070–1076
Chen XP, Qiu FZ, Wu ZD et al (2004) Chinese experience with hepatectomy for huge hepatocellular carcinoma. Br J Surg 91:322–326
Liu P, Yang J, Niu W et al (2011) Surgical treatment of huge hepatocellular carcinoma in the caudate lobe. Surg Today 41:520–525
Taniai N, Yoshida H, Tajiri T (2008) Adaptation of hepatectomy for huge hepatocellular carcinoma. J Hepatobil Pancreat Surg 15:410–416
Choi GH, Han DH, Kim DH et al (2009) Outcome after curative resection for a huge (≥10 cm) hepatocellular carcinoma and prognostic significance of gross tumor classification. Am J Surg 198:693–701
Yamashita YI, Taketomi A, Shirabe K et al (2011) Outcomes of hepatic resection for huge hepatocellular carcinoma (≥10 cm in diameter). J Surg Oncol 104:292–298
Fan ST, Yang ZF, Ho DW et al (2011) Prediction of post hepatectomy recurrence of hepatocellular carcinoma by circulating cancer stem cells: a prospective study. Ann Surg 254:569–576
Acknowledgment
Supported by National High Technology Research and Development Program of China (2006AA02Z4B2), National Science and Technology Major Projects (2009ZX09103-681), Clinical Subjects’ Key Project of Ministry of Health (2007–2009), and National Natural Science Foundation of China (81172018).
Conflict of interest
The authors have no conflicts of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
268_2013_2095_MOESM1_ESM.tif
Supplementary-Figure 1. Computed tomography scan and human HCC tumor specimens from hepatectomy. (A-C) show solitary huge HCC, 19.0 × 15.0 cm, expansive growth within an intact capsule. (D-F) show nodular huge HCC, 12.0 × 8.0 cm, multiple nodules, without capsules. (TIFF 1402 kb)
268_2013_2095_MOESM2_ESM.tif
Supplementary-Figure 2. (A) Liver parenchyma was transected using a combining techniques with a straight iron suction and the high frequency electrical knife. After selective hemihepatic inflow occlusion, incision was made along the liver-cutting line, using the scraping, suction, stir, coagulation, ligation technology. (B) To dissect and ligate the right anterior branche of the portal trunk. (C) The remnant liver was sutured by mattres apposition suture. (D) A solitary huge HCC was removed, tumor size 12.0 ×9.0 cm. (TIFF 1683 kb)
268_2013_2095_MOESM3_ESM.tif
Supplementary-Figure 3. Anterior resection for left hemihepatectomy: liver hanging maneuver combined with selective hemihepatic inflow occlusion. (A) CT scan demonstrated a nodular HCC in left lobe with thrombus, tumor size 13.0 × 8.0 cm. (B) Selective hemihepatic inflow occlusion, the white arrow to the left portal pedicle occlusion belt. The blue arrow to the right portal pedicle occusion belt and yellow one to Pringle manuver occlusion belt. (C) liver hanging maneuver: to establish retrohepatic inferior retrohepaticvena cava tunnel. The arrow show that the vascular clamp had pass through the tunnel and reached the suprahepatic vena cava lacunae. (D) Two liver hanging belts were placed through the tunnel. Ischemia boundary which indicate the cutting-line appeared after left portal pedicle occlusion. The white arrows show the liver hanging belts. The yellow arrow show the ischemia boundary (TIFF 843 kb)
Rights and permissions
About this article
Cite this article
Yang, L., Xu, J., Ou, D. et al. Hepatectomy for Huge Hepatocellular Carcinoma: Single Institute’s Experience. World J Surg 37, 2189–2196 (2013). https://doi.org/10.1007/s00268-013-2095-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-013-2095-5