
Abstract
Background
Treatment of peripherally located liver tumors with diaphragmatic invasion is technically demanding but does not preclude resection for cure. The aim of the present study was to compare patients undergoing combined liver and diaphragmatic resection with those submitted to hepatectomy alone so as to evaluate the safety, effectiveness, and value of this complex surgical procedure.
Methods
From January 2000 to September 2011, 36 consecutive patients underwent en bloc liver-diaphragm resection (group A). These were individually matched for age, gender, tumor size, pathology, and co-morbitidies with 36 patients who underwent hepatectomy alone during the same time (group B). Operative time, warm ischemia time, blood loss, required transfusions, postoperative complications, and long-term survival were evaluated.
Results
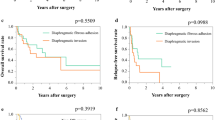
Mean operative time was significantly longer in group A than in group B (165 vs 142 min; P = 0.004). The two groups were comparable regarding warm ischemia time, intraoperative blood loss, required transfusions, and postoperative laboratory value fluctuations. Some 33 % of group A patients developed complications postoperatively as opposed to 23 % of group B patients (P = 0.03). The mortality rate was 2.8 % in group A compared to 0 % in group B. Postoperative follow-up demonstrated 60 % 1-year survival for group A patients as opposed to 80 % 1-year survival for group B patients, a difference that is practically eliminated the longer the follow-up period is extended (35 vs 40 % 3-year survival and 33 vs 37 % 5-year survival for group A and group B patients, respectively).
Conclusions
En bloc diaphragmatic and liver resection is a challenging but safe surgical procedure that is fully justified when diaphragmatic infiltration cannot be ruled out and the patient is considered fit enough to undergo surgery.
Similar content being viewed by others


References
DuBray BJ Jr, Chapman WC, Anderson CD (2011) Hepatocellular carcinoma: a review of the surgical approaches to management. Mo Med 108:195–198
Karoui M, Tayar C, Laurent A et al (2007) En bloc stapled diaphragmatic resection for local invasion during hepatectomy: a simple technique without opening the pleural cavity. Am J Surg 193:786–788
Elias D, Sideris L, Pocard M et al (2004) Results of R0 resection for colorectal liver metastases associated with extrahepatic disease. Ann Surg Oncol 11:274–280
Lin MC, Wu CC, Chen JT et al (2005) Surgical results of hepatic resection for hepatocellular carcinoma with gross diaphragmatic invasion. Hepatogastroenterology 52:1497–1501
Yamashita Y, Morita K, Iguchi T et al (2011) Surgical impacts of an en bloc resection of the diaphragm for hepatocellular carcinoma with gross diaphragmatic involvement. Surg Today 41:101–106
Smyrniotis V, Arkadopoulos N, Theodosopoulos T et al (2007) Transdiaphragmatic approach facilitates resection of large (>12 cm) liver tumors. J Hepatobiliary Pancreat Surg 14:383–386
Smyrniotis V, Farantos C, Kostopanagiotou G et al (2005) Vascular control during hepatectomy: review of methods and results. World J Surg 29:1384–1396. doi:10.1007/s00268-005-0025-x
Lau WY, Leung KL, Leung TW et al (1995) Resection of hepatocellular carcinoma with diaphragmatic invasion. Br J Surg 82:264–266
Leung KF, Chui AK, Leung KL et al (2001) Clinicopathological study of hepatocellular carcinoma with diaphragmatic involvement. Br J Surg 88:681–682
Lordan JT, Riga A, Worthington TR et al (2009) Early and long-term outcomes of patients undergoing liver resection and diaphragm excision for advanced colorectal liver metastases. Ann R Coll Surg Engl 91:483–488
Tung WY, Chau GY, Loong CC et al (1996) Surgical resection of primary hepatocellular carcinoma extending to adjacent organ(s). Eur J Surg Oncol 22:516–520
Jeng KS, Chen BF, Lin HJ (1994) En bloc resection for extensive hepatocellular carcinoma: is it advisable? World J Surg 18:834–839. doi:10.1007/BF00299079
Li GZ, Turley RS, Lidsky ME et al (2012) Impact of simultaneous diaphragm resection during hepatectomy for treatment of metastatic colorectal cancer. J Gastrointest Surg 16:1508–1515
Conflict of interest
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Arkadopoulos, N., Kyriazi, M.A., Perelas, A. et al. Should Diaphragmatic Involvement Preclude Resection of Large Hepatic Tumors?. World J Surg 37, 2197–2201 (2013). https://doi.org/10.1007/s00268-013-2083-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-013-2083-9