
Abstract
Background
The goal of the present research was to study patients who underwent laparoscopic total extraperitoneal repair using slit and non-slit mesh placement.
Methods
Patients who underwent laparoscopic inguinal hernia repair in our hospital between 2005 and 2009 were interviewed and examined. Surgery outcome, hernia recurrence, postoperative pain and time to return to normal physical activities, and surgery satisfaction were compared.
Results
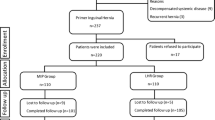
During the study period 389 consecutive patients underwent laparoscopic groin hernia repair: 387 by the total extraperitoneal (TEP) approach and 2 by the TAPP approach. Six of the TEP patients were converted to TAPP. Eighty-seven patients in the TEP group had slit mesh placement and 300 had non-slit mesh placement. Mean follow-up was 36 months (range: 6–66 months). At follow-up, 387 patients responded to a request for interview and 277 were examined. The overall recurrence rate was 4.7%, the incidence of constant postoperative pain was 1.3%, the presence of permanent testicular pain was 2.8%, and patient satisfaction with the surgery was 94.5%. A significantly lower recurrence rate was found in the slit mesh group than in the non-slit group (0.6% versus 5.9%; p < 0.003). There was no difference in the length of time until return to normal activities, patient satisfaction, and postoperative pain between the groups. Surgery time and the occurrence of testicular pain were significantly greater in the anatomic group.
Conclusions
Total extraperitoneal inguinal hernia repair with slit mesh placement is a safe technique with a very low recurrence rate and is superior to non-slit mesh positioning.


Similar content being viewed by others


References
Rives J, Stoppa R, Fortesa L et al (1968) Dacron patches and their place in surgery of groin hernia. 65 cases collected from a complete series of 274 hernia operations. Ann Chir 22:159–171 [in French]
Korman JE, Hiatt JR, Feldmar D et al (1997) Mesh configurations in laparoscopic extraperitoneal herniorrhaphy. A comparison of techniques. Surg Endosc 11:1102–1105
Ger R (1982) The management of certain abdominal herniae by intra-abdominal closure of the neck of the sac. Preliminary communication. Ann R Coll Surg Engl 64:342–344
Schultz LS, Graber JN, Pietrafitta J et al (1990) Early results with laparoscopic inguinal herniorrhaphy are promising. Clin Laser Mon 8:103–105
Dulucq JL (1992) Treatment of inguinal hernia by insertion of a subperitoneal patch under pre-peritoneoscopy. Chirurgie 118:83–85 [in French]
Arregui ME, Young SB (2005) Groin hernia repair by laparoscopic techniques: current status and controversies. World J Surg 29:1052–1057. doi:10.1007/s10029-008-0341-9
Barrat C, Surlin V, Bordea A et al (2003) Management of recurrent inguinal hernias: a prospective study of 163 cases. Hernia 7:125–129
Lo Menzo E, Spector SA, Iglesias A et al (2009) Management of recurrent inguinal hernias after total extraperitoneal (TEP) herniorrhaphies. J Laparoendosc Adv Surg Tech A19:475–478
Chowbey PK, Pithawala M, Khullar R et al (2006) Complications in groin hernia surgery and the way out. J Minim Access Surg 2:174–177
Quilici PJ, Greaney EM Jr, Quilici J et al (2000) Laparoscopic inguinal hernia repair: optimal technical variations and results in 1700 cases. Am Surg 66:848–852
Bell RC, Price JG (2003) Laparoscopic inguinal hernia repair using an anatomically contoured three-dimensional mesh. Surg Endosc 17:1784–1788
Ersin S, Aydin U, Makay O et al (2006) Is testicular perfusion influenced during laparoscopic inguinal hernia surgery? Surg Endosc 20:685–689
Celik AS, Memmi N, Celebi F et al (2009) Impact of slit and nonslit mesh technique on testicular perfusion and volume in the early and late postoperative period of the totally extraperitoneal preperitoneal technique in patients with inguinal hernia. Am J Surg 198:287–291
Author information
Authors and Affiliations
Corresponding author
Additional information
This study fulfilled part of the requirements for the MD degree of the first author.
Rights and permissions
About this article
Cite this article
Domniz, N., Perry, Z.H., Lantsberg, L. et al. Slit versus Non-slit Mesh Placement in Total Extraperitoneal Inguinal Hernia Repair. World J Surg 35, 2382–2386 (2011). https://doi.org/10.1007/s00268-011-1251-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-011-1251-z