
Abstract
Background
In Ghana and most developing countries there has been no standardized study of reduction mammaplasty (RM) in patients with symptomatic macromastia (SM), despite its debilitating effects. This study aimed to analyze the physical and psychological effects associated with female patients who underwent reduction mammaplasty and to develop a guideline for plastic surgeons in developing countries to know the most important signs and symptoms to consider in SM patients.
Methods
From 2003 to 2009, all females with SM who visited Komfo Anokye Teaching Hospital (KATH) in Kumasi, Ghana, for RM were given a questionnaire designed to evaluate SM-related physical and psychological effects. These patients were then provided the same questionnaire at their final visit 5 months postoperatively to assess the effects of RM on SM.
Results
Sixty-three patients who underwent RM were evaluated, with a mean age of 28.5 years. Twenty-seven (42.9%) patients reported that their macromastia started during puberty, with 3 (4.8%) patients associating the onset with pregnancy. Thirty (47.6%) patients reported having SM for more than 10 years. Multiple regression analysis revealed upper- and lower-back pain (p = 0.0005), painful bra strap grooves (p = 0.0041), teasing (p = 0.01), and poor self-image (p = 0.021) to be significant factors for which patients underwent RM. Postoperatively, most of the patients’ physical symptoms resolved, while 2 (3.2%) patients complained of residual psychological effects.
Conclusion
RM offers substantial symptomatic relief for patients with SM and results in significant improvement in the patient’s quality of life. This study conclusively demonstrates that, upper- and lower-back pain, painful bra strap grooves, teasing, and poor self-image should be considered by plastic surgeons before deciding which SM patient to treat when confronted with numerous SM patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Female breast hypertrophy, or macromastia, is the development of abnormally large breasts. This condition can cause significant clinical manifestations when the excessive breast weight adversely affects the supporting structures of the shoulders, neck, and trunk. Symptomatic macromastia (SM) is distinguished from large, normal breasts by the presence of persistent pain and resultant physical signs. This condition and its associated clinical signs and symptoms can be alleviated by reduction mammaplasty (RM) using Wise’s, Skoog’s, Strömbeck’s, or Regnault’s technique or the nipple-areola transplantation technique [1]. Women who suffer from macromastia also frequently present to the plastic surgeon with heightened body image dissatisfaction and maladaptive behavioral changes in response to their breast size and shape.
Numerous investigations have demonstrated improvement in physical and psychological symptoms after RM [2–5]. However, none of these studies used well-validated, standardized measures in Ghana or in other developing countries. Agbenorku et al. [6] reported that 28 out of 70 patients (40%) with breast developmental anomalies had SM in Sogakope, Ghana in 2010. Other studies from Komfo Anokye Teaching Hospital (KATH) revealed an increase in the number of patients presenting with symptomatic macromastia in the plastic surgery unit of KATH [7–9].
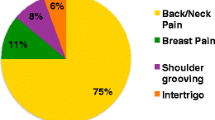
Recognition of SM as a morbid condition has increased in recent decades due to earlier physical development and higher susceptibility to circulating progesterone and estrogen. This early recognition may be due to several factors, including improved access to medical care, increased patient awareness, and acceptance by the medical profession of unique issues pertaining to women’s health. Reduction mammaplasty is one of the most frequently performed operations on the female breast. Puosson and Verchere [1, 10] first described a surgical procedure to reduce breast size but it was not adopted into practice until the 1920s [3, 11]. Today, RM is a routine procedure for which several techniques have been described. Research in the field of RM has focused primarily on the various types of surgical techniques [2, 4–6] rather than on outcomes related to these techniques. Only recently have studies considered the physical and psychosocial implications of RM for SM [1, 4, 10–20]. Efforts to validate objectively the medical necessity for RM have been difficult given that physical and psychosocial morbidity in breast hypertrophy can be very subjective. The physical signs and symptoms noted by patients with macromastia include headache, shoulder pain, upper- and lower-back pain, intertrigo, and shoulder (bra strap) grooving. Psychosocial effects include difficulty in participating in sports, difficulty finding clothes to fit, teasing, and poor self-image.
Most of the previous studies that discuss RM have been retrospective in design, using surveys or chart reviews as information sources. One prospective study by Gonzalez et al. [4] compared the physical symptoms of 39 women undergoing RM with those of a control group of women with “small breasts.” After surgery, their physical symptoms were statistically significant or less than the levels in the control group.
This study is an analysis of the physical and psychological symptoms associated with female patients who underwent RM at KATH in Kumasi, Ghana, so as to establish a guideline for plastic surgeons in similar situations in developing countries to enable them to identify patients with ease when confronted with numerous SM patients.
Materials and Methods
Treatment Center
The Reconstructive Plastic Surgery & Burns Unit is one of the units of the Surgery Directorate in KATH. The unit has three surgeons. KATH is the second-largest hospital in Ghana, a country of an estimated 26 million people, and the only tertiary health institution in the middle belt of the country. It is the main referral hospital for 16 million people in the Ashanti, Brong Ahafo, Northern, Upper East, and Upper West regions. It is accredited for postgraduate training in various surgical and medical disciplines by the West African College of Surgeons, West African College of Physicians, and the Ghana College of Physicians and Surgeons.
Surgical Procedure
A bilateral reduction mammaplasty using the nipple-areola reposition technique, which aims to preserve the nipples and some areolar tissue to retain sensibility and future breastfeeding, was performed [9]. A modified superior pedicle (Pitanguy method) was used, thus preserving the normal embryologic relationship between the skin and the underlying gland, the nipple-areola complex, on a transverse superior dermoglandular pedicle. A standard Wise pattern marking was drawn with the patient in the standing position. After deepithelialization, the glandular parenchyma was resected in an inverted keel form. With the resection, two pillars were created (medial and lateral), which when approximated allowed a mild tension closure of the breast around the superior pedicle. In five cases of gigantic breasts, the nipple-areola complex was harvested and grafted at the predetermined desired site of the breast mound. The distance from the sternal notch to the new nipple position was 21 cm. No blood transfusion was needed. Suction drains were used in all patients and then removed later at an average of 6 days.
Data Collection
The patients for this descriptive study signed an informed consent form and ethical clearance was approved by the KATH Ethics Committee. Breast measurements were taken and recorded before surgery. All patients were given a questionnaire designed to evaluate macromastia-related physical and psychological effects. The questionnaire had three sections: demographic, physical, and psychological effects. The physical section contained a list of physical signs and symptoms noted by patients with macromastia, while the psychosocial effects section included conditions such as difficulty in participating in sports, difficulty finding clothes to fit, teasing, and poor self-image. The patients were then provided the same questionnaire at their final monthly follow-up visit 5 months after the surgery. Pre- and postoperative photographs of the patients were taken (Figs. 1, 2).

A 25-year-old breast hypertrophy patient. a Preoperative view, b after 9 months

A 45-year-old breast hypertrophy patient. a Preoperative view, b after 9 months
Statistical Analysis Methods
Statistical analysis to determine the physical and psychological factors influencing SM patients to undergo RM was performed using the analytical tool multiple regressions from SPSS ver. 18.0 (SPSS, Inc., Chicago, IL, USA). The beta (standardized regression coefficients) and significance level (p) were the parameters needed for such analysis. The beta value is a measure of how strongly each predictor demographic variable influences the criterion variable. The beta is measured in units of standard deviation while p determines which variable is important for the study.
Study Design
This prospective cohort study was designed such that signs and symptoms of SM patients who visited the Reconstructive Plastic Surgery & Burns Unit of KATH from 2003 to 2009 were recorded before and after the RM. Monthly follow-up visits were also included in the study so as to capture any other complaints of the patients. The age of patients ranged between 15 and 55 years. Patients were included in study if they had reported SM at our unit during the study period and had agreed to have RM at our unit. Patients were excluded from the study if they had SM but had reported to a different unit of KATH, would not give written consent for the study, were discharged against medical advice during admission, and could not visit the Reconstructive Plastic Surgery & Burns Unit for follow-up for at least 5 months.
Results
A total of 63 patients underwent reduction mammaplasty and were evaluated over the course of 6 years. Ages ranged from 15 to 54 years, with a mean age of 28.5 years (Fig. 3). The majority (47.6%, n = 30) of the patients had a tertiary form of education, while 38.1% (n = 24) and 14.3% (n = 9) had secondary and basic education, respectively. The amount of the breast tissue removed during surgery ranged from 2 to 8 kg (mean = 5.8 kg).

Age distribution of breast hypertrophy patients
Most (42.9%, n = 27) patients reported that SM started during puberty, with a few (4.8%, n = 3) patients associating the onset with pregnancy (Fig. 4). Psychological distresses outnumbered physical signs and symptoms, with difficulty finding clothes to fit being the second most common discomforting psychological factor reported after poor self-image (Table 1). Postoperative patient responses showed significant relief from both physical and psychological distresses. The follow-up period lasted 5 months for the study, although some patients still visited the facility after that period. Few physical symptoms of SM were reported, while 2 (3.2%) patients complained of psychological effects such as poor self-image (Table 1).

Onset of breast hypertrophy among patients
Preoperatively, 28.6% (n = 18), 38.1% (n = 24), 23.8% (n = 15), and 9.5% (n = 6) of the patients complained of one, two, three, and more than three SM-related symptoms, respectively. In terms of duration of symptoms, 47.6% (n = 30) reported to have lived with SM for more than 10 years, while the remainder of the patients (52.4%, n = 33) lived with it for less than 10 years (Fig. 5).

Duration of breast hypertrophy reported by patients
Results of the analysis show that predictor variables such as back pain (upper and lower), painful bra strap grooves, and psychological distress (teasing, poor self-image) had a greater impact on the criterion variable (Table 2). There was no significance associated with the number of symptoms (p > 0.05), as shown in Table 3.
Discussion
Several studies have already demonstrated the beneficial effects of breast reduction on symptom relief and health-related quality of life in the Western world [4, 12–21], including the psychological and social consequences of breast reduction surgery. With respect to the contemporary debate on financial restraints in developed countries [21–24], RM for symptomatic macromastia in Ghana is covered by the National Health Insurance Scheme (NHIS). Nevertheless, patients with symptomatic macromastia in Ghana find it difficult to obtain health care due to long waiting lists and the paucity of plastic surgeons. Also, plastic surgery is done only in KATH and Korle-Bu Teaching Hospital, hence access to these facilities is difficult. Despite the high prevalence of symptomatic macromastia in Ghana [6–9], there has been no standard study on the effect of RM in patients with SM and quality-of-life factors. This study is an analysis of the physical and psychological symptoms associated with female patients who underwent RM at KATH so as to establish a guideline for plastic surgeons in similar situations, especially in developing countries; to identify which SM patients need immediate attention.
Agbenorku et al. [6–9] previously reported macromastia in the southern (Sokagope in 2010) and central (KATH in 2007, 2006, and 2001) parts of Ghana, with the age of patients ranging from 12 to 30 years. The mean age of patients in our study was 28.5 years and Figs. 1 and 2 show photos of patients with SM. Results of this study revealed that 47.6% of the patients suffered with SM for more than 10 years. The studies of Davis et al. [13] and Goin et al. [4, 15] also reveal the physical trauma that SM patients go through, and its psychological effect. Throughout their formal education, these females would be teased by others and eventually develop a negative self-image, which postoperatively prevailed for some. Delays in the treatment of SM may be associated with many factors, including ignorance that SM can be surgically treated, superstition that people with SM have been cursed by gods or supernatural forces, public shyness including the hospital, and long waiting lists to be seen by a plastic surgeon.
A comparison of the pre- and postoperative symptoms of SM patients reveals a few physical complications endured after surgical treatment. Although some patients still affirm having psychological distress postoperatively, the general outcome of the surgeries was satisfactory to both patient and surgeon. Studies demonstrate that women seeking breast reduction have a similar preoperative symptom burden across a wide range of breast sizes. Furthermore, Spector and Karp [23, 24] reported that the symptomatic improvement derived from RM is not significantly different among women with different breast sizes. The findings of our study corroborate the fact that RM plays a significant role in the relief of pain and psychological distress of SM patients, irrespective of available resources, technology, and country.
Multiple regression analysis of the symptomatic burden reveals that upper- and lower-back pain (p = 0.0005), painful bra strap grooves (p = 0.0041), teasing (p = 0.01), and poor self-image (p = 0.021) are significant factors for patients undergoing RM. However, no significant level was shown to be associated with the number of symptoms reported by a patient (p > 0.05). Also, Spector et al. [23] showed that RM resulted in significant improvement in all SM and quality-of-life factors analyzed (p < 0.000001). There were no significant differences (p > 0.05) in pre- and postoperative macromastia-related symptoms with the exception of lower-back pain (preoperative p = 0.026), shoulder pain (preoperative p = 0.014), and painful bra strap grooves (preoperative p = 0.0059). Analysis of the symptomatic burden of macromastia on several quality-of-life factors showed no significant differences (p > 0.05) in either the pre- or the postoperative symptom scores across all groups in any of the categories assessed [23]. Again, other statistical analyses, such as that of the study of Spector and Karp [24], parallel this present study. On the other hand, Elenie et al. [22] reported that the risk differences (RD) (95% confidence intervals) for eight signs and symptoms experienced by the patient with SM (Table 1) were statistically significant for the reduction or elimination postoperatively of signs and symptoms experienced preoperatively. However, there was a significant study design effect (p < 0.01 for analysis of variance test) for the RD for pre- and postoperative shoulder grooving, with a higher RD.
Thus, from the statistical analysis of our data, compared with others, it was deduced that for immediate and effective intervention by the plastic surgeon when confronted with deciding which severe SM patients to treat, the statistically significant symptoms (upper- and lower-back pain and painful bra strap grooves) and psychological distress (teasing and poor self-image) should be taken into consideration, especially in countries such as Ghana where there are only a few specialized plastic surgeons. In other developing countries with a shortage of plastic surgeons, where there is no form of health insurance to cover treatment of SM, the delay situation will be worse than in Ghana where the issue of financing treatment does not contribute much to the delay in seeking medical care due to NHIS. This guideline could help alleviate the burden of severe SM patients by aiding the plastic surgeon in Ghana and other developing countries in triaging SM patients by taking into consideration important signs and symptoms proposed by this study.
Conclusion
Reduction mammaplasty offers substantial relief of SM and results in significant improvement in a patient’s quality of life. This study conclusively demonstrates that plastic surgeons in developing countries, when confronted with numerous SM patients in unbearable pain, should consider the important signs and symptoms proposed by this study, such as upper- and lower-back pain, painful bra strap grooves, teasing, and poor self-image, before deciding who to treat.
References
Baker SB, Burkey BA, Thornton P, LaRossa D (2001) Juvenile gigantomastia: presentation of four cases and review of the literature. Ann Plast Surg 46:517–526
Atterhem H, Holmner S, Janson PE (1998) Reduction mammaplasty: symptoms, complications, and late results. A retrospective study on 242 patients. Scand J Plast Reconstr Surg Hand Surg 32(3):281-286
Bostwick J (1983) Breast reduction in aesthetic and reconstructive surgery. C.V. Mosby, St. Louis
Gonzalez F, Walton RL, Shafer B (1993) Reduction mammaplasty improves symptoms of macromastia. Plast Reconstr Surg 91:1270–1276
Schnur PL, Hoehn JG, Ilstrup DM (1991) Reduction mammaplasty: cosmetic or reconstructive procedure? Ann Plast Surg 27:232–237
Agbenorku P, Agbenorku M, Iddi A et al (2010) Incidence of breast developmental anomalies: a study at Sogakope, Ghana. Nig J Plast Surg 6(1):1–5
Agbenorku P, Addae-Mensah L (2001) Management of juvenile macromastia: our experience at the Komfo Anokye Teaching Hospital (KATH), Kumasi, Ghana. Indian J Clin Pract 2(6):13–16
Agbenorku P, Akpaloo J, Turkson E, Agbenorku M (2007) Breast diseases including breast developmental anomalies in Kumasi, Ghana. Nig J Plast Surg 3(1):11–16
Agbenorku P (2006) Nipple-areolar complex (NAC) composite grafts in the management of macromastia: review of complications. Nig J Surg Res 8(1):77–80
Berg A, Stark B, Malec E (1994) Reduction mammaplasty: a way helping females with neck, shoulder and back pain symptoms. Eur J Plast Surg 17:84–86
Thorek M (1989) Possibilities in the reconstruction of the human form 1922. Aesthetic Plast Surg 13:55–58
Boschert MT, Barone CM, Puckett CL (1996) Outcome analysis of reduction mammaplasty. Plast Reconstr Surg 98:451–454
Davis GM, Ringler SL, Short K, Sherrick D, Bengtson BP (1995) Reduction mammaplasty: long-term efficacy, morbidity, and patient satisfaction. Plast Reconstr Surg 96:1106–1110
Glatt BS, Sarwer DB, O’Hara DE, Hamori C, Bucky LP, LaRossa D (1999) A retrospective study of changes in physical symptoms and body image after reduction mammaplasty. Plast Reconstr Surg 103:76–82
Goin MK, Goin JM, Gianini MH (1977) The psychic consequences of a reduction mammaplasty. Plast Reconstr Surg 59:530–534
Goin MK (1982) Psychological reactions to surgery of the breast. Clin Plast Surg 9:347–354
Harris DL (1983) Self-consciousness of disproportionate breast size: a primary psychological reaction to abnormal appearance. Br J Plast Surg 36:191–195
Hollyman JA, Lacey JH, Whitfield PJ, Wilson JS (1986) Surgery for the psyche: a longitudinal study of women undergoing reduction mammaplasty. Br J Plast Surg 39:222–224
Raispis T, Zehring RD, Downey DL (1995) Long-term functional results after reduction mammaplasty. Ann Plast Surg 34:113–116
Schnur PL, Schnur DP, Petty PM, Hanson TJ, Weaver AL (1997) Reduction mammaplasty: an outcome study. Plast Reconstr Surg 100:875–883
Borkenhagen A, Röhricht F, Prei S, Schneider W, Brähler E (2007) Changes in body image and health-related quality of life following breast reduction surgery in German macromastia patients: a new tool for measuring body image changes. Ann Plast Surg 58(4):364–370
Elenie BC, Shuhuan Z, Matthew JG (2001) Clinical outcomes in reduction mammaplasty: a systematic review and meta-analysis of published studies. Mayo Clin Proc 76:504–510
Spector JA, Singh SP, Karp NS (2008) Outcomes after breast reduction: does size really matter? Ann Plast Surg 60(5):505–509
Spector JA, Karp NS (2007) Reduction mammaplasty: a significant improvement at any size. Plast Reconstr Surg 120(4):845–850
Acknowledgment
Our gratitude goes to the KATH theatre nursing staff, especially Ms. Vida Rose Frimpong, Mercy Lanyoh-Bruce, and Stella Mintah, and the many surgical assistants who helped in the management of these patients. We also thank Mr. Thomas Diby who typed the manuscript.
Conflict of interest
The authors declare that they have no conflicts of interest to disclose. No funding was received for this work.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Agbenorku, P., Agamah, G., Agbenorku, M. et al. Reduction Mammaplasty in a Developing Country: A Guideline for Plastic Surgeons for Patient Selection. Aesth Plast Surg 36, 91–96 (2012). https://doi.org/10.1007/s00266-011-9750-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-011-9750-8