
Abstract
Purpose
The aim of this study was to assess the stress level and depression among orthopaedic surgeons in Saudi Arabia. In addition, to evaluate orthopedic training programs related factors that might have a critical role in the development of depression among orthopaedic surgeons.
Methods
The study adopted a cross-sectional study design. Two validated questionnaires were utilized, the Patient Health Questionnaire 9 (PHQ-9) and the Perceived Stress Scale (PSS-10) for assessing depressive symptoms and stress levels. Data was collected by sending the survey to the Saudi Commission for Health Specialties so they could be distributed throughout all registered orthopaedic surgeons.
Results
The study sample consisted of 325 participants. The results revealed that the severity of depression varied across the different groups. As per the PHQ-9 criteria, 74 (22.8%) were initially diagnosed with major depression. Among assistant consultants, 39.5% reported severe depression, while 34.9% reported mild depression. Consultants predominantly reported moderate perceived stress (82.9%) with a notable proportion experiencing high perceived stress (12.4%). Assistant consultants showed a balanced distribution, with 93.0% reporting moderate perceived stress and 4.7% reporting high perceived stress. Demographic variables gender, relationship status and having children revealed statistically significant relationship with PHQ-9 scores (p-value < 0.05) but not with PSS-10 scores.
Conclusion
The study highlights pressing need to address mental health concerns within orthopaedic surgeons. To address these challenges, healthcare institutions should implement comprehensive mental health support programs offering resources for stress management, counseling services, and peer support groups.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Burnout and depression have recently been looked at differently due to its critical role and influence that it might have, not only on physicians themselves but also the quality of care provided to the patients [1, 4]. At time of increasing risk of suicidal thoughts and burnout among health care personnel [1]. Screening for burnout and depression among health care workers has recently received more attention lately. Surgical training, in comparison to medical training, has long been regarded as demanding, but its unique mental health challenges are rarely addressed. In addition to having negative psychological and physical effects on individuals, depression has been linked to decreased patient care and an increase in medical errors [2, 3].
There is increased risk of burnout and depression among medical personnel at different levels compared to their peers in non-medical field [5]. All specialties are affected even though they may vary in extinct based on level of training, gender, or the presence of social and personal support [10]. However, for orthopaedic surgery residents there was only one study conducted that looked at the burnout and quality of life [6], other studied the mental health among orthopedic residents [7]. Recent study showed that burnout among orthopaedic surgery residents reached 52% in addition to depression which was found to be in 13% [8]. In addition, stress which is a situation that disturbs or is likely to disturb a person’s normal psychological or physiological functioning [10]. Considered to be an important issue that have to be studied among medical personnel, one study conducted recently showed that around 80% of the doctors had moderate level of stress [11].
Using the patient health questionnaire-9 (PHQ-9) which is a 9-questions survey which has been validated and wildly used to assess for depression among participants, it has been reliable and accepted as well [9, 12, 13]. Moreover, Utilizing the perceived stress scale-10 (PSS-10) have been used to evaluate the stress level, a 10-questions survey that have been used in multiple studies to assess perception of stress [14].
Limited number of studies looked at the mental health in terms of stress level and depression among orthopaedic surgeons internationally, no studies conducted locally. Therefore, we aimed to assess the stress level and depression among orthopaedic surgeons in Saudi Arabia.
Materials and methods
A cross sectional study was carried out across Saudi Arabia to assess the depression and stress level among orthopaedic surgeons at different levels, by sending a questionnaire that was prepared by the research team to the Saudi Commission for Health Specialties (SCFHS).
The questionnaire prepared included four main parts, participants’ demographics, program characteristics, and the two validated tests utilized in the study including patient health questionnaire-9 (PHQ-9) and the perceived stress scale-10 (PSS-10). The scoring of items in the PHQ-9 ranges from “0” (not at all) to “3” (nearly everyday). Moreover, a total PHQ-9 score of 0 to 4 points is considered “normal” or “minimal” depression. A score of 5 to 9 indicates mild depression, 10 to 14 for moderate depression, 15 to 19 for moderately severe depression, and 20 or more for severe depression [13, 15]. Regarding the scoring of items in the PSS-10 ranges from “0” (never) to “4” (very often). Furthermore, a total of PSS-10 score of 0 to 13 points is considered “low stress”, a score of 14 to 26 points is considered “moderate stress”, and a score of 27 to 40 is considered “high stress”.
Initial diagnosis of major depressive disorder could be made if the following criteria were met in the PHQ-9, five questions or more are checked as more than half the days, and either questions 1 or 2 should be checked with at least more than half the days.
All data collected from Microsoft Excel sheet was transferred to statistical software SPSS file for analysis. Data were checked for any missing information and new variables were recorded and computed based on the data extracted. The categorical data were presented by percentages and frequencies such as gender. Whereas the numerical data were prescribed as mean and standard deviation such as age. For inferential statistics, Chi square was used to find the association between the categorical variable. The test was considered significant if p-value is less than 0.05.
Ethical approval
was obtained by King Abdullah International Medical Research Center (KAIMRC). Consent was obtained from participants before being involved in this cross-sectional study. All data were kept confidential with no identifications being asked or presented. The privacy of all participants was assured, and access to research data was limited to the study group members.
Results
Table 1 below represents a demographic characteristic of the participants of the study where an overall of 325 surgeons participated in this research. Among the surgeons the average age and standard deviation was 40.0 ± 10.8. Moreover, 295 (90.8%) of the surgeons were male and 30 (9.2%) were females. In addition, the average and the standard deviation of BMI of the participants was 28.67 ± 4.6. 240 (73.8%) of the surgeons had children while 85 (26.2%) did not have children. 261 (80.3%) of the participants were married, 59 (18.2%) were single and 5(1.5%) were divorced. On the other hand, 254 (78.2%) of the participants lived with the family, 66 (20.3%) of the participants lived alone and 5 (1.5%) lived with friends. 220 (67.7%) of the participants were smokers 105 (32.3%) were not smokers. Work center distribution shows that the majority of respondents work in the Ministry of Health (43.4%), followed by private hospitals (29.5%), and university hospitals (6.2%). Finally, the regional distribution of respondents indicates a diverse geographic spread, with the central region having the highest representation at 28.9%, followed closely by the western region at 28.6%.
Table 2 bellow presents the program characteristics responses of the individuals that participated on the stress assessment and depression among the orthopaedic surgeons in Saudi Arabia. Majority 110 (33.8%) agreed that surgical independence was excellent while 15 (4.6%) of the surgeons said surgical independence was poor. Most 120 (36.9%) of the surgeons claimed that the faculties reputation was very good while 13 (4.0%) claimed that it was poor. Majority 112 (34.5%) reported that the volume of cases was very good while 11 (3.4%) reported that they were poor. 93 (28.6%) of the surgeons indicated that variety of cases was good while only 13 (4.0%) indicated they were poor. Majority 107 (32.9%) reported that educational support was poor while 26 (8.0%) indicated they were excellent. In addition, 96 (29.5%) indicated that the satisfaction level was good. Also, 114 (35.1%) indicated that their quality of life was good. Similarly, majority 118 (36.3%) of the surgeons reported that the on-call amount was good.
Table 3 gives an illustration on the patient health questionnaire. Majority 147 (45.2%) showed little interest or pleasure in doing things in several days while 41 (12.6%) showed little interest or pleasure in doing things in nearly every day. Most 142 (43.7%) of participant felt down, depressed or hopeless in several days, 40 (12.3%) showed similar characteristics in nearly every day. Majority 110 (33.8%) did not at all experience trouble in falling or staying asleep or sleeping too much. Most 134 (41.2%) felt tired or had little energy in several days, 53 (16.3%) had trouble falling or staying asleep or sleeping too much in nearly every day. 120 (36.9%) did not have poor appetite or overeating, 43 (14.8%) had poor appetite or overeating nearly every day. Majority 137 (42.2%) did not at all feel bad about themselves or that seeing themselves as failures or letting their family down. 118 (36.3%) did not at all got Trouble in concentrating on things, such as reading the newspaper or watching television. More than a half 194 (59.7%) did not at all move or speaking so slowly that other people could have noticed or the opposite. A super majority 257 (79.1%) did not at all have thoughts that they would be better off dead or of hurting themselves in some way.
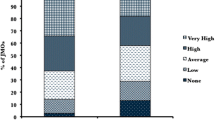
The Table (4) provided depicts the depression levels among medical professionals across different training levels. Among the total respondents, the majority were consultants, totaling 105, followed by residents with 99 respondents, and assistant consultants with 43 respondents. The severity of depression varied across the different groups. Among assistant consultants, 39.5% reported severe depression, while 34.9% reported mild depression. Similarly, among associate consultants, 40.0% reported mild depression, and 26.7% reported moderate depression. Notably, among fellows, the distribution was more evenly spread, with 31.3% reporting mild depression and 25.0% reporting moderately severe depression. Among residents (R1-R5), the prevalence of depression varied, with R2 residents having the highest percentage of mild depression at 38.9%, while 50% of R3 residents reported the highest percentage of moderately severe to severe depression and R4 residents having the highest percentage of moderate to moderately severe depression at 60.0%.
Table 5 presents the response of the participants on the perceived stressed scale-10. More than half 163 (50.2%) have been sometimes upset because of something that happened unexpectedly, 23 (7.1%) were never upset. Majority122 (37.5%) almost never felt unable to control the important things in your life. Most 136 (41.8%) of the participants in the study sometimes in the past month felt nervous or stressed. 112 (34.5%) of the surgeons in the past month fairly often felt confident about their ability to handle personal problems. 151 (46.5%) of the participants sometimes in the past month, often felt that things were going their way. 134 (41.2%) sometimes in the past month often had been able to control irritations in their life. Majority 142 (43.7%) sometimes in the past month, often felt that they were on top of things. Majority 151 (46.5%) sometimes in the last month, often had been angered because of things that were outside their control. 127 (39.1%) of participants sometimes in the past month they often felt that difficulties were piling up so high that you could not overcome them.
The Table (6) below shows the stress level of the 325 individuals that participated in the study. Among consultants, 82.9% reported moderate perceived stress, while 12.4% reported high perceived stress. Assistant consultants, while fewer in number, demonstrated a relatively balanced distribution, with 93.0% reporting moderate perceived stress and 4.7% reporting high perceived stress. Notably, fellows exhibited a higher prevalence of moderate perceived stress at 68.8%, with 18.8% reporting high perceived stress. Among residents, particularly R1 and R2, there was a noticeable trend towards higher levels of perceived stress, with 70.6% and 83.3% reporting moderate perceived stress, respectively. Additionally, 17.6% of R1 residents reported low perceived stress, indicating less responsibility and challenges at the early stages of their training. Among all orthopedic surgeons that participated in the study, a high percentage of surgeons reported having moderate perceived stress at 81.2%, with 6.1% reported having low perceived stress and 12.6% reported having high perceived stress. Indicating an increased stress demand among other specialties at all levels.
Table 7 below shows that females had a significantly higher mean PHQ-9 score compared to males (13.8 vs. 8.7), indicating a higher level of depressive symptoms. Participants who were single had a significantly higher mean PHQ-9 score compared to those who were married or divorced. Participants with children had a significantly lower mean PHQ-9 score compared to those without children. In summary, gender, relationship status, having children, number of children, living status, and smoking status were associated with differences in depressive symptoms (PHQ-9 scores), but not perceived stress (PSS-10 scores).
Discussion
The study aimed to access the stress level and depression among orthopaedic surgeons in Saudi Arabia. The study examined important aspects like the demographic variables and program characteristics to determine potential correlation with perceived stress or depressive symptoms. Most surgeons in the study give positive feedback regarding the program characteristics with 36.9% of surgeons rating the reputation of their faculties as very good, with 27.7% rating it as excellent. Additionally, 35.1% of the surgeons reported very good satisfaction levels, 29.5% rated their quality of life as good. According to a similar study conducted among surgeons in Pakistan the program characteristics was a significant stressor with surgeons working in reputable faculties have low levels of stress or depression [16].
The PHQ-9 responses provide valuable insights into the prevalence of depressive symptoms among surgeons. A significant portion of the surgeons reported experiencing little interest or pleasure in doing things, with 45.2% experiencing this symptom several days and 19.7% experiencing it more than half the days. Similarly, feelings of depression or hopelessness were prevalent, with 43.7% experiencing them several days and 18.8% experiencing them more than half the days. Sleep disturbances were also common, with 33.8% reporting trouble falling or staying asleep or sleeping too much, and 32.6% experiencing this symptom several days. Feelings of tiredness or low energy were reported by 41.2% of surgeons several days and 24.0% more than half the days. In a study that aimed to check the level of depression among high students in Florida, the feeling of being sad or helpless was quite prevalent with about 28% of the students with about 9.6% contemplating suicide [17]. This comparison highlights the widespread nature of depressive symptoms across different demographics.
The distribution of PHQ-9 scores among orthopaedic surgeons reveals a concerning prevalence of depressive symptoms within the population. The data reveals that most consultants experienced either none or mild levels of depression, comprising 32.4% and 26.7% of the group, respectively. However, there were still significant proportions reporting moderate (23.8%) and moderately severe (10.5%) depression. This suggests a substantial portion of consultants facing challenges in managing their mental health. Similarly, associate consultants, assistant consultants, and board-certified professionals also exhibited varying levels of depression across the severity spectrum. While the majority in each group reported none or mild depression, there were notable percentages experiencing moderate to moderately severe depression, emphasizing the prevalence of mental health struggles among these professionals. A study among 467 adult population in Riyadh, Saudi Arabia revealed that 3.6% (17 patients) showed no signs of depression, while 22.1% (103 patients) had minimal depression. Additionally, 34.3% (160 patients) experienced mild depression, 24.2% (113 patients) reported moderate depression, and 10.1% (47 patients) exhibited moderately severe depression. Furthermore, 5.8% (27 patients) were classified as having severe depression [18].
The distribution of PSS-10 scores among orthopaedic surgeons highlights the prevalence of perceived stress within the training levels group. The majority of consultants reported experiencing moderate perceived stress (82.9%), followed by 12.4% reporting high perceived stress and only 4.8% indicating low perceived stress. Similar patterns were observed among assistant consultants, associate consultants, and board-certified professionals, with the majority reporting moderate perceived stress levels. Notably, fellows displayed a higher prevalence of high perceived stress (18.8%) compared to other groups, indicating potential challenges or pressures specific to that stage of their training. Among residents (R1-R5), there was a notable proportion reporting high perceived stress (11.8–25.0%), suggesting the demanding nature of residency programs. Interestingly, while R2 residents showed a high proportion reporting moderate perceived stress (83.3%), there was no reported low perceived stress within this group. In another study conducted by Nazir et al., among doctors revealed the majority of participants, accounting for 79.8%, reported experiencing moderate levels of stress, with 13.8% indicating low stress levels [19].
The study further sort to find the association between stress and depression scores and various demographic characteristics among orthopaedic surgeons. The was gender disparities, with female surgeons exhibiting a significantly higher mean PHQ-9 score (13.8) compared to males (8.7), indicating a greater prevalence of depressive symptoms among female surgeons. Similarly, single surgeons reported a higher mean PHQ-9 score (12.4) compared to their married, or divorced counterparts, suggesting that relationship status may influence depressive symptoms. Furthermore, surgeons without children had a significantly higher mean PHQ-9 score (11.9) compared to those with children, indicating a potential protective effect of parenthood against depression. Additionally, living alone was associated with a higher mean PHQ-9 score (9.7), suggesting that social support and living arrangements may impact depressive symptoms. However, the association between stress scores (PSS-10) and demographic characteristics was not statistically significant. These findings underscore the importance of addressing gender-specific, familial, social, and lifestyle factors in mental health interventions for orthopaedic surgeons, particularly targeting vulnerable subgroups such as female surgeons and those living alone. A study conducted in China among physicians that gender and social support (marriage or staying with family or friends) gave a statistically significant relationship with having perceived stress [20].
A significant limitation of the study stemmed from its use of a cross-sectional study design. While cross-sectional studies excel at identifying relationships between variables at a specific moment, they inherently lack the capacity to establish causality or track changes over time. Therefore, future research efforts should consider employing longitudinal or mixed-methods approaches to provide deeper insights into factors that contribute to stress and depression among surgeons over time.
In conclusion, this study highlights the significant prevalence of perceived stress and depressive symptoms among orthopedic surgeons in Saudi Arabia. The findings from this study emphasize on the importance of mental health issues among orthopaedic surgeons. The association between gender, relationship status, and parenthood with depressive symptoms shows the importance of tailored interventions targeting vulnerable subgroups, such as female surgeons and those living alone. To mitigate the impact of stress and depression on orthopedic surgeons, healthcare institutions should implement comprehensive mental health support programs that offer resources for stress management, counseling services, and peer support groups. It would also be important to encourage a culture of open communication and destigmatizing mental health issues within the medical community can encourage early intervention and promote overall well-being among surgeons.
Data availability
All data generated or analyzed during this study are included in this published article.
References
Menon NK, Shanafelt TD, Sinsky CA, Linzer M, Carlasare L, Brady KJ, Trockel MT (2020) Association of physician burnout with suicidal ideation and medical errors. JAMA Netw open 3(12):e2028780–e2028780
West CP, Huschka MM, Novotny PJ, Sloan JA, Kolars JC, Habermann TM, Shanafelt TD (2006) Association of perceived medical errors with resident distress and empathy: a prospective longitudinal study. JAMA 296(9):1071–1078
West CP, Tan AD, Habermann TM, Sloan JA, Shanafelt TD (2009) Association of resident fatigue and distress with perceived medical errors. JAMA 302(12):1294–1300
Lin DT, Liebert CA, Esquivel MM et al (2017) Prevalence and predictors of depression among general surgery residents. Am J Surg 213:313–317
Dyrbye LN, West CP, Satele D et al (2014) Burnout among US medical students, residents, and early career physicians relative to the general US population. Acad Med 89:443–451
Sargent MC, Sotile W, Sotile MO, Rubash H, Barrack RL (2009) Quality of life during orthopaedic training and academic practice, part 1: orthopaedic surgery residents and faculty. J Bone Joint Surg - Am Volume 91:2395–2405
Gosselin MM, Alolabi B, Dickens JF, Li X, Mesfin A, Spraggs-Hughes A, Miller AN (2019) Cross-sectional survey results on mental health among orthopedic surgery residents across North America. J Surg Educ 76(6):1484–1491
Lichstein PM, He JK, Estok D, Prather JC, Dyer GS, Ponce BA, Collaborative Orthopaedic Educational Research Group (2020) What is the prevalence of burnout, depression, and substance use among orthopaedic surgery residents and what are the risk factors? A collaborative orthopaedic educational research group survey study. Clin Orthop Relat Research® 478(8):1709–1718
Abdulrahman M, Nair SC, Farooq MM, Kharmiri A, Al Marzooqi A, F., Carrick FR (2018) Burnout and depression among medical residents in the United Arab Emirates: a multicenter study. J Family Med Prim Care 7:435–441
Sadock BJ, Sadock VA (2011) Kaplan & Sadock’s synopsis of Psychiatry: behavioral Sciences/Clinical Psychiatry, 10th edn. Wolters Kluwer, Lippincott Williams & Wilkins
Chakraborti A, Ray P, Sanyal D, Thakurta RG, Bhattacharayya AK, Mallick AK, Ali SN (2013) Assessing perceived stress in medical personnel: in search of an appropriate scale for the Bengali population. Indian J Psychol Med 35(1):29–33
Asch DA, Jedrziewski MK, Christakis NA (1997) Response rates to mail surveys published in medical journals. J Clin Epidemiol 50(10):1129–1136
Kroenke K, Spitzer RL, Williams JB (2001) The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 16(9):606–613
Cohen S, Kamarck T, Mermelstein R (1983) A global measure of perceived stress. J Health Soc Behav 24:385–396
PHQ-9 Depression Test Questionnaire. (n.d.). Retrieved February 2 (2021) from https://patient.info/doctor/patient-health-questionnaire-phq-9
Khurshied S, Hisam A, Khurshid N, Khurshid M (2020) Burnout among surgeons; depression, anxiety, and stress between consultant versus post-graduate trainee. Pakistan J Med Sci 36(7):1745
Gunderson J, McDaniel K, DiBlanda A (2023) Association between insufficient sleep, depressive symptoms, and suicidality among Florida high school students. Prev Chronic Dis, 20
AlHamad NS, AlAmri K (2021) The association between social media use and depressive symptoms among adults in Riyadh, Saudi Arabia. J Family Med Prim Care 10(9):3336
Nazir N, Hussain HA, Ahmed U, Sabri AA, Ahmad N, Rasool AG (2021) Perceived stress score among doctors serving at various government and private hospitals in Faisalabad. J Pakistan Med Association 71(5):1424–1427
Fu C, Wang G, Shi X, Cao F (2021) Social support and depressive symptoms among physicians in tertiary hospitals in China: a cross-sectional study. BMC Psychiatry 21(1):217
Acknowledgements
Not Applicable.
Funding
No funding was obtained for this research.
Author information
Authors and Affiliations
Contributions
WJ, MA, AA, and ZJ developed the idea and designed the methods. ZJ, KH collected the data. ZJ, KH, and AH analyzed, interpreted, and presented the results. All authors wrote the manuscript. WJ, MA, ZJ, and AH critically revised the manuscript for content and finalization. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by King Abdullah International Medical Research Center (KAIMRC). Institutional review board number NRC23R/045/01.
Consent for publication
Applicable.
Consent to participate
The informed consent was given and provided for all participants in the study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Aljuhani, W.S., Aljaafri, Z.A., Alhadlaq, K.H. et al. Assessment of stress level and depression among orthopaedic surgeons in Saudi Arabia. International Orthopaedics (SICOT) (2024). https://doi.org/10.1007/s00264-024-06288-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00264-024-06288-0