
Abstract
Purpose
A lack of specific intra-operative markers for accurate positioning of the syndesmotic screw can result in its malpositioning. Knowledge of the axial orientation of the syndesmosis can help in reducing this risk of malpositioning of the syndesmotic screw. In this CT-based study, we investigated the axial relationships of intact syndesmoses with various rigid bony landmarks around the ankle joint that were independent of foot and horizontal plane.
Methods
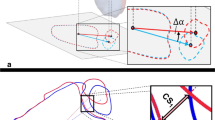
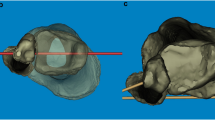
We analyzed 126 CT-based studies of uninjured normal ankle joints and defined the following bony landmarks: posteromedial and posterolateral surface of the distal tibia, bimalleolar tips, and anterior and posterior extents of both malleoli. Axial differences between coronal plane through the central axis of syndesmosis and modified coronal planes through these bony landmarks were then measured. Software-based lateral radiographs were created with the reference coronal plane for each radiograph being kept perpendicular to the plane of the viewing screen.
Results
The mean axial differences parting the syndesmotic axis from the modified coronal planes based on distal tibial posteromedial surface, distal tibial posterolateral surface, bimalleolar tips, anterior bimalleolar extents, and posterior bimalleolar extents were − 3.15°, 13.73°, 4.10°, 11.95°, and 12.24°, respectively. With the exception of the posterolateral surface of the distal tibia, all other bony landmarks were radiologically identifiable in the majority of cases.
Conclusion
Our study attempts to provide a solution to the issues related to malpositioning of the syndesmotic screw by providing new bony landmarks that can be clinically and fluoroscopically used for syndesmotic-screw positioning. The relationships of bimalleolar tips, anterior and posterior bimalleolar extents, and the posteromedial surface can be reliably used as landmarks for directing syndesmotic screws.





Similar content being viewed by others

References
Bekerom MPVD, Hogervorst M, Bolhuis HW, Dijk CNV (2008) Operative aspects of the syndesmotic screw: Review of current concepts. Injury 39:491–498. https://doi.org/10.1016/j.injury.2007.11.425
Dattani R, Patnaik S, Kantak A, Srikanth B, Selvan TP (2008) Injuries to the tibiofibular syndesmosis. J Bone Joint Surg (Br) 90:405–410
Ebraheim NA, Lu J, Yang H, Mekhail AO, Yeasting RA (1997) Radiographic and CT evaluation of tibiofibular syndesmotic diastasis: a Cadaver Study. Foot Ankle Int 18:693–698. https://doi.org/10.1177/107110079701801103
Ebraheim NA, Lu J, Yang H, Rollins J (1998) The fibular incisure of the tibia on CT scan: a cadaver study. Foot Ankle Int 19(5):318–321
Elgafy H, Semaan HB, Blessinger B, Wassef A, Ebraheim NA (2010) Computed tomography of normal distal tibiofibular syndesmosis. Skelet Radiol 39(6):559–564
Gonzalez T, Egan J, Ghorbanhoseini M et al (2017) Overtightening of the syndesmosis revisited and the effect of syndesmotic malreduction on ankle dorsiflexion. Injury 48(6):1253–1257
Hermans JJ, Beumer A, de Jong TA, Kleinrensink GJ (2010) Anatomy of the distal tibiofibular syndesmosis in adults: a pictorial essay with a multimodality approach. J Anat 217(6):633–645
McBryde A, Chiasson B, Wilhelm A, Donovan F, Ray T, Bacilla P (1997) Syndesmotic screw placement: a biomechanical analysis. Foot Ankle Int 18:262–266
Mendelsohn ES, Hoshino CM, Harris TG, Zinar DM (2014) CT characterizing the anatomy of uninjured ankle syndesmosis. Orthopedics 37:E157–E160
Ovaska MT, Mäkinen TJ, Madanat R, Kiljunen V, Lindahl J (2014) A comprehensive analysis of patients with malreduced ankle fractures undergoing re-operation. Int Orthop 38(1):83–88
Park YH, Choi WS, Choi GW, Kim HJ (2017) Ideal angle of syndesmotic screw fixation: a CT-based cross-sectional image analysis study. Injury 48:2602–2605. https://doi.org/10.1016/j.injury.2017.08.067
Pereira DS, Koval KJ, Resnick RB, Sheskier SC, Kummer F, Zuckerman (1996) Tibiotalar contact area and pressure distribution: the effect of mortise widening and syndesmosis fixation. Foot Ankle Int 17:269–274.
Rudloff MI (2013) Fractures of the lower extremity. In: Canale ST, Beaty JH, Campbell WC (eds) Campbell’s operative orthopedics. Elsevier/Mosby, Philadelphia
Schepers T, Linden HVD, Lieshout EMV, Niesten DD, Van der Elst M (2013) Technical aspects of the syndesmotic screw and their effect on functional outcome following acute distal tibiofibular syndesmosis injury. Injury 45:775–779. https://doi.org/10.1016/j.injury.2013.09.035
Van Heest TJ, Lafferty PM (2014) Injuries to the ankle syndesmosis. J Bone Joint Surg Am 96:603–613
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kumar, A., Passey, J., Goel, L. et al. New landmarks for ideal positioning of syndesmotic screw: a computerised tomography based analysis and radiographic simulation. International Orthopaedics (SICOT) 44, 665–675 (2020). https://doi.org/10.1007/s00264-019-04467-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-019-04467-y