
Abstract
Objective
The purpose of this study was to verify the age-, gender- and Arbeitsgemeinschaft für Osteosynthesefragen (AO) type-specific clinical characters of adult tibial plateau fractures in 83 hospitals in China and to investigate whether altitude has potential relationships with adult tibial plateau fractures.
Methods
A retrospective investigation was performed on consecutive patients with tibial plateau fractures treated in 83 hospitals in China between January 2010 and December 2011, data including age, gender and imaging were collected retrospectively through the PACS system and case reports checking system, imaging were classified into six types under fully qualified estimation based on AO classification. To further investigate imparities among different altitudes in China, all data were classified into four groups according to the centre altitudes of each city, G1 = plains group (<500 m), G2 = hills group (500-1000 m), G3 = mountain areas group (1000-2000 m), and G4 = plateau group (>2000 m). Comparison of gender distribution, age distribution and AO type were done.
Results
A total of 6,227 adult tibial plateau fractures were included. Men in the age range of 40–44 years were the most affected patients, and the overall high-risk injury type was 44-B. In four groups, the same peak age showed, namely, 40-44 years in males and 55–59 years in females. Age distribution showed no statistically significant difference in four groups (P > 0.05), while sex distribution and AO type indicated statistically significant differences (P < 0.05). Note an inversion of sex ratio among people over 60 years.
Conclusion
Our study showed that men in the 40–44 year age range are the most affected patients, and different sex distribution as well as injury type of adult tibial plateau fractures differed with various altitudes in China.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Tibial plateau fractures account for 1–2% of the whole body fractures and 8% of geriatric fractures [1]. High-quality epidemiological studies can provide us essential cognitive understanding about its distribution, incidence, related risk factors and dominant affected type, and can further guide clinical treatments and improve the prognosis. China exists within a unique geopolitical context such that its huge, diverse landmass surely leads to various epidemiologic fracture features. Tibial plateau fracture was one of the severe fractures with which millions of patients were reported fully or partially disabled due to traffic injuries during recent decades [2]. Nilson et al. revealed latitude as well as UV radiation had statistically significant correlations with incidence of hip fracture in Sweden, and increased risk of hip fracture in the northern parts of Sweden was higher than the middle and southern parts [3]. Authors in our country hold the view that higher elevation and longer sunlight hours may promote spine fractures [4]. Other articles revealed bone density disparities in males and females at different ages which related to osteoporosis fracture. Some authors even pointed out that lower limbs fractures manifest intensively with regional characteristics and time difference, and we had reasons to suspect a potential relationship between altitude and tibial plateau fracture. However, no research focusing on tibial plateau fractures and altitude was done; moreover, a nationwide epidemiological study has not been demonstrated in China. Thus, our study aimed to identify the overall epidemiology characters of adult tibial plateau fractures and reveal potential epidemiological characteristics of adult tibial plateau fractures in different altitudes in China on a multicentre level.
Methods
This epidemiology study was approved by The Institutional Review Board of the third hospital of Hebei Medical University in compliance with the Helsinki Declaration. And our study was a retrospective study based upon historical X-ray films, no human participants were included. Written informed consent of each participation was not necessary. All adult fractures (≥16 years) were collected through the PACS system and case reports checking system, which were referred to 83 hospitals through multi-stage random sampling from 31 provinces in China between January 2010 and December 2012. A total of 414,935 patients (431,822 cases) were included, from which 6,227 adult tibial plateau fractures were screened and met our final eligibility criteria. For further comparison, we divided all cases into four groups based on the centre altitudes of each city, G1 = plains group (<500 m), G2 = hills group (500–1000 m), G3 = mountain areas group (1000–2000 m), G4 = plateau group (>2000 m). Age was categorized at an interval of five years and a series of 14 units were produced: 16–20 years, 21–25 years, 26–30 years, 31–35 years, 36–40 years, 41–45 years, 46–50 years,51–55 years, 56–60 years, 61–65 years, 66–70 years, 71–75 years,76–80 years and ≥80 years. Initial radiographs were reviewed and classified based on OA/OTA classification. A “41” was assigned for proximal tibial fractures and types A, B, C were classified according to the anatomic location of fractures, thereinto tibial plateau fracture represented type B and type C, and two types were subdivided into three subgroups described as 1,2,3 based on the severity of fracture. Eligibility criteria were patients over 16 years old, and definite tibial plateau fracture, i.e. those with unequivocal imaging data that can be diagnosed with tibial plateau fracture and Arbeitsgemeinschaft für Osteosynthesefragen (AO) type can be confirmed. Exclusive criteria were patients under 16 years old, imaging data absence, obsolete fracture, pathological fracture, periprosthetic fractures, and patients under unambiguous or suspicious diagnosis.
All images were identified independently by four orthopaedic specialist registrars on two occasions separated by a one-week interval based on OA/OTA classification. Assessments should maintain consistency. Once disagreement occurred, it would be transferred to a superior physician. To ensure accuracy, three arbiters including two senior orthopaedic surgeons and one senior radiologist regularly sampled radiographs. A questionable imaging would roll back to assessment directly. Quality standards were: misjudgment under 1% of each researcher (500 cases/1 researcher), misclassified ratio under 3%.
Statistical analysis
Statistical analyses were conducted by standard statistical software (SPSS Version 21.0, Chicago, IL, USA). The descriptive analyses are presented in Tables 1, 2 and 3. Continuous variable age was expressed as median and range and the test was performed using Mann-Whitney U-test. Discontinuous variables regarding age, sex and AO type were expressed as count, and chi-square test was performed. P < 0.05 was considered as statistically significant.
Results
A total of 6,227 adult tibial plateau fractures were collected, including 4,275 males and 1,952 females, 2704 were on the right and 3,523 were on the left. These fractures encompassed 56.90% of all proximal tibia fractures and 1.50% of the whole body fractures. The highest proportion of adult tibial plateau fractures were patients in the age of 40 to 44 years, males more than females. Peak age in males was 40–44 years and we should note a different peak age in females of 55–59 years.
Type 41-B was the most common type of adult tibial plateau fractures (3,998 cases, 64.20%), followed by 2,229 cases of type 41-C (35.80%). Incidence detailed in six subgroups were 1,435 cases in type 41-B1 (23.04%), 1375 cases in type 41-B2 (22.08%), 1206 cases in type 41-B3(19.37%), 595 cases in type 41-C1 (9.56%), 747 cases in type 41-C2 (12.00%), and 887 cases in type 41-C3 (14.24%).
Epidemical characteristics of the four groups
There were 3,178 males and 1,340 females in group 1, 632 males and 380 females in group 2, 672 males and 471 females in group 3, and 21 males and four females in group 4. The average ages were 45.37 ± 14.3, 46.33 ± 8.19, 46.50 ± 6.63, and 46.28 ± 8 years old, respectively. Difference were considered statistically significant at p < 0.05 (Table 1).
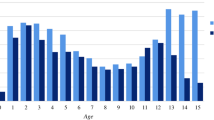
Age distribution showed no statistically significant difference in the four groups (χ2 = 44.439, P = 0.253), while same peak age showed 40–44 years in males and 55–59 years in females. Sex distribution of the four groups had statistically significant difference at 25–29, 30–34, 40–44, 65–69 intervals (P < 0.05). Note an interesting gender-inversion among patients over 60 years in the four groups, indicating an elderly female dominance and suggesting that a number of female patients gradually exceeded male patients with increasing age (Table 2, Figs. 1 and 2). Number of adult tibial plateau fractures, sex ratio as well as age distribution showed downward tendency with increased altitudes.

Frequency distribution of age range of 6,227 adult tibial plateau fractures (five-year interval)

Sex–age distribution of 6,227 cases and four groups
Gender-AO type distribution
Our conclusions from the 6,227 cases were that 41-B was the predominant type, and the most affected subgroup type was 41-C2 in males and 41-B2 in females (Table 3). Ratio of gender in type 41-B was higher than type 41-C, demonstrating males prone to be severely damaged.
There were statistically significant differences in AO types in the four groups, and a comparison between 41-B and 41-C was χ2 = 8.563, P = 0.036, while intergroup comparison among the six subgroups showed χ2 = 66.145, P = 0.000. Dominant AO types the of four groups were 41-B1 in group 1, 41-B2 in group 2 and 3, 41-C2 in group 4, respectively. Sex distribution of the six subgroups was statistically significant (p < 0.05), and all involved specific bimodal distribution (Figs. 3 and 4).

Gender-AO type distribution of four groups

AO type distribution of four groups
Discussion
The first tibial plateau fracture was reported by Sir Astley Cooper in 1825. In 1990, Donaldson et al. reported an average incidence of 26/100,000/year in a 1981 census of three years [5]. Court-Brown and Caesar revealed a higher incidence of 13.3/100,000/year in 2000 [1]. Similarly, the incidence in the North Denmark region was 10.3/100,000/year from 2005 to 2010 [6]. Court-Brown and Caesar also concluded that prevalence of fractures was changing rapidly resulting from diverse injury mechanism and aging population and revealed a 1.2% proportion of proximal tibial fractures in whole body fractures [1]. Incidence in other articles was approximately 1.3% compared to 1.5% in our study [7]. There was a slight discrepancy stated in these articles basically due to small sample size and limited single centre research.
A systematic retrospective review conducted by Tian ye et al. investigated 1,033 tibial plateau fractures in the Third Hospital of Hebei Medical University from 2003 to 2007. It demonstrated an occupation of 54.11% in all proximal tibia fractures, 10.09% of tibial and fibular fractures and 1.86% of whole body fractures [3].
Our study indicated a male predominance of tibial plateau fractures, and the same result was proven by Albuquerque et al., which referred a male predominance (70%) of tibial plateau fractures [8]. But controversy existed in Rasmus Elsoe’s cohort study, which found that a female predominance accounted for 53% [6]. Another important finding of our study was that tibial plateau fracture was primarily present in men at 40–44 years. Whereas in 1979, Schatzker et al. reported the most affected ages were 60–70; a possible explanation for this change, we believe, is the increased number of vehicles and traffic problems [9].
Number of tibial plateau fractures in the four groups in descending order were G1, G2, G3, G4. Negative correlation occurred between altitudes and the dominant fracture type, which can be explained by the restricted hospitals and few admitted patients in the plateau group; it also related to a lagging economy, less urban construction and poor communications compared to the plains group. In our four groups, age distributions were similar, while gender distribution and AO type were statistically significantly different. Frequency of severe fracture type increased along with evaluated altitude, whereby possible reasons might be altitudes have impact on bone density, daily diet, lifestyle, sunlight hours, communications, and finally, different injury mechanisms were generated, but no study had been firmly established.
Same peak ages were observed both in the overall cases and the four groups, i.e. males in the 40–44 year age group and females in the 55–59 year group. The most relevant factor we were concerned about was bone density. One research in Yunnan demonstrated that bone density of lumbar vertebrae of the general population in Kunming was higher than that in Chengdu [4]. The authors hold the view that higher elevation and longer sunlight hours may promote this occasion; when comparing it to people of north China, it was slightly lower. The researchers also did a preliminary analysis and suggested that high elevation created a depression and oxygen-deprived environments, so local population tend to have average lower body height and weight with such longer-term exposure, all of which can contribute to the lower bone density.
An very interesting inversion of sex ratio was noted among people over 60 years in our study, and we believed it had a relationship with the prevalence of osteoporosis, especially in elderly females [10, 11]. Evidence in Shanghai accessed density of tibia using quantitative ultrasound (QUS) bone measurement and concluded that SOS reached maximum at 30–39 years both in males and females. But in females, it fell rapidly at their fifth decade, while in males, SOS still sustained consistency over 50 years. This distinguished discrepancy can well explain the higher incidence of female osteoporosis fracture. Furthermore, menopause intensified this tendency [12]. Hung et al. depicted a bimodal curve of tibial cortical porosity (Ct.Po) during an adult life, abundant cortical bone was lost during people’s middle age, and cortical porosity sharply increased at the beginning of the fifth decade [13]. Indeed, elderly females became the most affected population of tibial plateau fractures .
Our study had certain limits in that the whole study was mainly based on X-ray films, and no comparisons were done with advanced imaging, i.e. CT or MRI. Elsoe reviewed the first epidemiology characters of tibial fractures according to CT [6]. Khan et al. concluded better diagnosis of plateau fractures using CT or MRI [14,15,16,17,18]. Another shortage was the lack of efficient information, i.e. injury mechanism, associated complications, intra-articular lesions of the knee, spinal cord injuries and other high-energy musculoskeletal system diseases, causing our study to only offer less useful evidence for clinics. Limitation also occurred in using the AO principle, Hohl’s [19, 20], Schatzker’s [21] and the recent “three column” concepts all have their own unique approach and may have better clinical benefits. Albuquerque et al. merged Hohl’s classification with the other two and identified a new classification presents greater interobserver accordance [8]. Yang et al. suggested a three-column classification can provide better understanding of fracture morphology and injury mechanism of tibial plateau fracture [22]. For further evaluation, a well-designed prospective cohort study is needed.
Abbreviations
- PACS system:
-
Picture achieving and communication system
- SD:
-
Standard deviation
- AO/OTA:
-
Association for the Study of Internal Fixation /Orthopaedic Trauma Association
- SPSS:
-
Standard statistical software
- QUS:
-
Quantitative ultrasound
- SOS:
-
Speed of sound
- Ct.Po:
-
Cortical porosity
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
Reference
Court-Brown CM, Caesar B (2006) Epidemiology of adult fractures: A review. Injury 37(8):691–697
Souza ER, Minayo M, Franco LG (2007) Avaliação do processo de implantação e implementação do Programa de Redução da Morbimortalidade por Acidentes de Trânsito. Epidemiol Serv Saúde 16(1):19–31
Tian Y (2015) Epidemiological analysis of adult tibial plateau fractures in the Third Affiliated Hospital to Hebei Medical University from 2003 through 2012. Chin J Orthop Trauma 05(17):424–427 (Chinese)
Xiaopeng K (2003) Research of human bone density in Yun nan. J Yun Man Mend Coll 01(24):1614–1618 (Chinese)
Donaldson LJ, Cook A, Thomson RG (1990) Incidence of fractures in a geographically defined population. J Epidemiol Community Health 44(3):241–245
Elsoe R, Larsen P, Nielsen NP, Swenne J, Rasmussen S, Ostgaard SE (2015) Population-based epidemiology of tibial plateau fractures. Orthopedics 38(9):e780–e786
Thomas C, Athanasiov A, Wullschleger M, Schuetz M (2009) Current concepts in tibial plateau fractures. Acta Chir Orthop Traumatol Cechoslov 76(5):363–373
Albuquerque RP, Hara R, Prado J, Schiavo L, Giordano V, do Amaral NP (2013): Epidemiological study on tibial plateau fractures at a level I trauma center. Acta Ortop Bras 21(2):109–115
Schatzker J, McBroom R, Bruce D (1979) The tibial plateau fracture. The Toronto experience 1968--1975. Clin Orthop Relat Res 138:94–104
Dhanwal DK, Cooper C, Dennison EM (2010) Geographic variation in osteoporotic hip fracture incidence: the growing importance of Asian influences in coming decades. J Osteoporos 2010:757102
Dhanwal DK, Dennison EM, Harvey NC, Cooper C (2011) Epidemiology of hip fracture: worldwide geographic variation. Indian J Orthop 45(1):15–22
Zhu G, Wang L, Wang H (1999) Quantitative ultrasound assessment of tibia in normal subjects in Shanghai and its clinical application. Chin J Osteoporos 04(5):52–55 (Chinese)
Hung VW, Zhu TY, Cheung WH, Fong TN, Yu FW, Hung LK, Leung KS, Cheng JC, Lam TP, Qin L (2015) Age-related differences in volumetric bone mineral density, microarchitecture, and bone strength of distal radius and tibia in Chinese women: a high-resolution pQCT reference database study. Osteoporos Int 26(6):1691–1703
Khan RM, Khan SH, Ahmad AJ, Umar M (2000) Tibial plateau fractures. A new classification scheme. Clin Orthop Relat Res 375:231–242
Gardner MJ, Yacoubian S, Geller D, Suk M, Mintz D, Potter H, Helfet DL, Lorich DG (2005) The incidence of soft tissue injury in operative tibial plateau fractures: a magnetic resonance imaging analysis of 103 patients. J Orthop Trauma 19(2):79–84
Shepherd L, Abdollahi K, Lee J, Vangsness CT Jr (2002) The prevalence of soft tissue injuries in nonoperative tibial plateau fractures as determined by magnetic resonance imaging. J Orthop Trauma 16(9):628–631
Conesa X, Minguell J, Cortina J, Castellet E, Carrera L, Nardi J, Caceres E (2013) Fracture of the anteromedial tibial plateau associated with posterolateral complex injury: case study and literature review. J Knee Surg 26(Suppl 1):S34–S39
Stannard JP, Lopez R, Volgas D (2010) Soft tissue injury of the knee after tibial plateau fractures. J Knee Surg 23(4):187–192
Luo CF, Sun H, Zhang B, Zeng BF (2010) Three-column fixation for complex tibial plateau fractures. J Orthop Trauma 24(11):683–692
Hohl M, Luck JV (1956) Fractures of the tibial condyle; a clinical and experimental study. J Bone Joint Surg Am 38-a(5):1001–1018
Schulak DJ, Gunn DR (1975) Fractures of tibial plateaus. A review of the literature. Clin Orthop Relat Res 109:166–177
Yang G, Zhai Q, Zhu Y, Sun H, Putnis S, Luo C (2013) The incidence of posterior tibial plateau fracture: an investigation of 525 fractures by using a CT-based classification system. Arch Orthop Trauma Surg 133(7):929–934
Acknowledgements
The authors wish to thank Dr. Wenjuan Wu and Dr. Jianling Cui, Radiologist, for their assistance and cooperation in this study.
This study was supported by the National Natural Science Foundation of China (Grant No. 81401789).
Author information
Authors and Affiliations
Contributions
Yingze Zhang and Wei Chen designed the study; Song Liu, Tao Zhang, Pan Hu, Jialiang Guo, Haili Wang, Bing Yin made substantial contributions to collect and judge all data from participated hospitals; Peizhi Yuwen, Wei Chen, and Hongzhi Lv analyzed data and performed statistical analysis; Peizhi Yuwen and Wei Chen drafted the manuscript; Jiandong Hao, Yanling Su, and Chen Feng gave specific suggestions about the writing; YZ had primary responsibility for final content. All authors had read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare that they have no competing interests.
Additional information
Availability of data and materials
The datasets supporting the conclusions of this article are included in an additional file.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Yuwen, P., Lv, H., Chen, W. et al. Age-, gender- and Arbeitsgemeinschaft für Osteosynthesefragen type-specific clinical characters of adult tibial plateau fractures in eighty three hospitals in China. International Orthopaedics (SICOT) 42, 667–672 (2018). https://doi.org/10.1007/s00264-018-3769-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-018-3769-2