
Abstract
Purpose
The best treatment for intra-articular fractures of the calcaneus is still debated. The aims of this study were to determine whether intrafocal reduction of thalamic fractures is effective, to evaluate whether a locking nail is able to maintain reduction of the articular surface and to analyse the functional results of this original method.
Methods
This prospective study assessed 69 fractures treated with a locking fracture nail in 63 cases and with primary subtalar fusion in six (Calcanail ®, FH). Articular congruity and global reduction of the calcaneus was assessed in all patients by computed tomography (CT) scan three months postoperatively. Functional results were evaluated according to the American Orthopaedic Foot and Ankle Society Ankle–Hindfoot Score (AOFAS-AHS) and all complications recorded.
Results
For the 63 fracture nails, the average AOFAS score was 85.9 at a mean final follow-up of 12 months. Only three secondary fusions were performed. For the six comminuted fractures requiring primary fusion, the average AOFAS score was 75.9 at the last follow-up.
Conclusions
The posterior intrafocal approach for both reduction and locked nailing of intra-articular calcaneal fractures has been proven as an effective and reliable procedure.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
At present, there is insufficient evidence that surgical treatment is more effective than conservative treatment in displaced intra-articular calcaneal fractures (DIACFs) [1–3]. If decisive improvements have occurred since the 1990s in knowledge and operative techniques that result in better outcomes, postoperative complications remain matter of debate. With the extensile lateral approach, overall wound complication rate was 33 % in a retrospective study [4], while in a prospective randomised trial, a 16 % wound complication rate and a 5 % deep infection rate have been reported [2]. Nevertheless, as with all other articular fractures, DIACFs should be treated by anatomic reduction, internal fixation and early mobilisation; moreover, the global shape of the calcaneal body, i.e. height, width and length, should be restored to provide the best possible walking capacities. So, alternative procedures have been proposed, including two-stage procedures [5, 6], minimally invasive techniques [7–10], balloon reduction and cement fixation [11, 12] and even a tailor-made treatment strategy [13]. Indeed, most minimally invasive techniques achieve reduced primary stability and reduction accuracy is difficult to verify even with arthroscopy or 3D fluoroscopy.
For these reasons, we developed a technique five years ago to perform an intrafocal reduction through a channel created in the calcaneal tuberosity and—more recently—the use of an intramedullary locking nail to provide stable fixation of the reduced fracture [14]. An additional advantage of this procedure is that it allows primary subtalar fusion in cases in which articular surfaces are too damaged for reconstruction using the same approach and the same instrumentation [15]. The aims of this prospective study were to determine whether intrafocal reduction of thalamic fractures is effective and reliable, to evaluate whether a locking nail can maintain articular surface reduction and whether to analyse functional results of this original method.
Patients and methods
All patients operated with the locking nail (Calcanail ®, FH Orthopedics) since device availability in August 2011 were prospectively assessed in three trauma units (Centre hospitalier St Joseph St Luc, Lyon, France; Clinique de l’Union, Toulouse, France; University Hospital, Rostock, Germany). Indication for surgery was a DIACF with loss of subtalar joint congruity on standard X-rays and computed tomography (CT) scans. Oral consent was obtained from all patients for all aspects of this study, including the CT scan taken three months postoperatively.
Procedure
After soft tissue swelling had decreased, surgery was performed. Patients were usually placed in a lateral position, but a prone position was also used, especially in cases of bilateral fractures. The surgical technique was detailed in a previous publication [14]. Briefly, the technique is based on reduction of the depressed articular surface via a channel created through the tuberosity. By lowering the tuberosity, the talocalcaneal distractor facilitates reduction of the depressed articular surface and automatically corrects tuberosity varus. Once reduction is achieved, an intramedullary nail is introduced through the same channel and locked with two screws. The fracture nail is available in three lengths: 45, 50 and 55 mm; and one diameter: 10 mm. The fusion nail is available in three lengths: 75, 80 and 85 mm; and one diameter: 12 mm.
Patient series
Our prospective series consisted of 69 fractures in 63 patients. There were 48 men and 15 women; four men and two women sustained bilateral fracture. Mean patient age was 50.3 years (range 21–88). Trauma resulted from a simple fall from a variable height (27), a fall on the stairs (4), fall from a scaffold or ladder (24) or roof (3), a sport accident (5), a road traffic accident (5) and a hunting accident (1). Of the 63 patients, four were psychiatric, two had drug addictions, three were alcohol abusers and one was homeless. Gait was previously disturbed in two patients (one equinovarus foot, one contralateral ankle arthrodesis). The right side was affected in 28 cases, the left side in 35 and both sides in six. Sixty-seven were closed fractures and two were open (1 Gustilo 3B secondary to hunting trauma, 1 road traffic accident).
Radiographic evaluation
Based on standard X-rays and pre-operative CT scans, all fractures were evaluated according to the Sanders classification and the modified Utheza classification (Fig. 1); preoperative values of Böhler angle, Gissane angle and Goldzak index were recorded. Postoperative evaluation was based on plain films to evaluate restoration of the shape of the bone, Böhler angle and Gissane angle. Based on 3D volumic reconstructions of three month postoperative CT scans, Goldzak index was recorded to evaluate the height of the reduced thalamus and the accuracy of posterior facet reduction (Fig. 2). Reduction was considered excellent if type A or B and Böhler angle > 20°, as good if type D or E and Böhler angle > 20° and poor type C or Böhler angle < 20°.

Modified Utheza classification of displaced intra-articular calcaneal fractures (DIACFs) . In type I fractures, the surface is displaced but intact. In type II, the articular surface is involved

Assessment of articular surface reduction on anterior and superior views of computed tomography (CT) reconstruction. a Articular surface is preserved. b Articular surface is well reduced without gap or step. c Step through the articular surface without gap. d Gap at the posterosuperior portion of the articular surface. e Gap through the entire articular surface
Follow-up
Patients were followed up at three and six weeks and three, six and 12 months; despite our attempts, five patients were lost to follow-up. Patients were evaluated using the American Orthopedic Foot and Ankle Society Ankle–Hindfoot Score (AOFAS-AHS). Hindfoot position, fibular tendon entrapment and sural nerve injury were also documented.
Statistical analysis
Statistical analysis was performed with Medcalc (Medcalc version 12.7.5.0).
Results
Operative data
Among the 69 fractures were ten type IA, 11 type IB, 27 type IIA and 19 type IIB; in the two open fractures, classification was not possible. Mean preoperative Böhler angle was 6.7° (range −20° to +40°) when mean contralateral was 31°. Most patients were operated in a lateral position; a prone position was used in six and especially for bilateral fractures. A tourniquet was routinely used; procedure time was <1 h in all cases. Most fractures (n = 63) were treated with reduction and fixation with a locking fracture nail; in selected cases of severe articular fracture (n = 6), primary fusion of the subtalar joint was performed and a fusion nail used (Fig. 3).

Distribution of the 69 cases
Outcomes of the 63 internal fixations with a fracture nail
Immediate postoperative radiographs showed restoration of the global shape of the calcaneal body, with a mean Böhler angle of 29.9°, which was not modified at three (29.6°) and six (30.4°) months. Goldzak index rose from 0.6 preoperatively to 0.93. Based on the three month CT reconstructions, posterior facet reduction was analysed as type IIA in 35 % of cases, type IIB in 27 %, type IIC in 11 %, type IID in 16 % and type IIE in 11 % (Fig. 4). Therefore, reduction was rated as excellent in 62.5 % of cases, good in 12.5 % and poor in 25 %.

Fracture type IIA. Pre-operative standard X-rays (above, left) and computed tomography (CT) scan (above, right). Comparison of pre- and postoperative anterior views (below, left); standard X-rays at 1 year fllow-up (below, right). Reduction was rated B
At last follow-up (mean 12.3 months), 54 fractures were assessed (5 were lost to follow-up; 4 required secondary fusion), and average AOFAS-AHS score was 86.5. Mean AOFAS pain score was 32.5: no pain was reported by 22 patients, mild or occasional pain by 23 and moderate and daily pain by nine; no patient reported severe and permanent pain. At that follow-up, 37 patients presented no functional limitations, 12 presented limited recreational activities, three had limited daily activities with the need of a cane and two used crutches. Twenty-four patients walked without difficulty, 25 presented some difficulty on uneven ground and five had severe difficulty on uneven terrain or stairs. Finally, 51 patients had a normal gait and three an obvious limp. Ankle motion was preserved in all cases except two. Subtalar motion was normal or quite normal in 26 patients, 25–75 % normal in 23 and <25 % normal in five. No patient presented hindfoot malalignment. All data improved progressively during the follow-up except in three patients who needed a secondary fusion.
According to modified Utheza classification, types IA and IB fractures (Sanders type 2) obtained a mean AOFAS-AHS score of 87, type IIA (Sanders type 3) a mean of 84 and type IIB (Sanders type 4) a mean of 80; the difference was not significant (p = 0.12). No statistical difference was found in AOFAS score according to reduction type (Fig. 5, p = 0.18).

Correlation between the accuracy of reduction and functional results [American Orthopaedic Foot and Ankle Society Ankle–Hindfoot Score (AOFAS-AHS)]
Outcomes of the six primary fusions
Mean average AOFAS at the last follow-up was 75.6, for a maximal score of 92 points due to loss of subtalar joint motion.
Complications and subsequent surgery
Very few complications were recorded:
-
One psychiatric patient who walked bearing full weight on the immediate postoperative days had to be re-operated upon on day 30. The primary nail was removed and a subtalar arthrodesis performed with a fusion nail, leading to a final AOFAS score of 82.
-
Three secondary subtalar fusions were needed within the first year (3/63 = 5 %): two type IIB with two fracture lines through the articular surface, and one type IA fracture with associated intra-articular fracture of the talus.
-
Three regional pain syndromes resolved within 6 months without aftereffects, and their AOFAS scores at last follow-up were 79, 82 and 89, respectively.
-
Two nerve entrapments resolved spontaneously at six and eight months.
-
Six patients required implant removal: Early nail removal was done in one case in which the nail was too long and caused heel pain. In four patients, locking screws that were too long causing lateral discomfort when wearing shoes, requiring screw removal. One patient without discomfort strongly desired removal of the entire implant. Hardware removal was successful in all patients.
Discussion
There are no randomised controlled trials that demonstrate any advantage for surgical treatment of DIACFs. This is primarily due to the high rates of wound-healing complications and infections. Although good results have been reported when using the extensive lateral approach with plate fixation either with a standard or a locking plate, Sanders [16] reported an 11 % wound-necrosis rate, even in an experienced surgeon’s hands, and concluded that only well-trained surgeons should attempt these reconstructions.
Two-stage treatment of comminuted os calcis fractures have been proposed: primary indirect reduction with medial external fixation and delayed lateral plate fixation seemed to minimise wound-healing problems and reduce the risk for compartment syndrome of the foot [5, 6]. Minimally invasive techniques using a locking plate have become increasingly popular, but despite good anatomical results, with restoration of normal Böhler’s and Gissane’s angles, in all cases, functional results reached only 82 points according to the AOFAS scoring system [17]. This may possibly be explained by trauma to the fibular sheath, with subsequent restriction of subtalar joint mobility.
Implant advantages
The Calcanail technique, including the mini-invasive posterior approach and innovative reduction technique, drastically reduces surgical trauma and complication risk. No wound-healing problems were observed in our series, which is a major advantage when using the posterior approach through the tuberosity versus the extensive lateral approach. Both accurate reduction and stable fixation of the posterior facet are mandatory to ensure good outcomes. We did not evaluate reduction of the posterior facet and as proposed by Sanders [16]: indeed, the location at which the analysis was performed is not stated precisely, and their methodology is not detailed. That means we do not know whether the reduction was accurate on the anterior, mid or posterior portion of the facet or along the entire fracture line; this is a major point of concern. We preferred to analyse our anatomic results on the 3-month-follow-up CT reconstructions, which visualised the thalamus on lateral, medial, front, rear and top views (Fig. 6). The Calcanail technique provided good reduction in three quarter of cases; an intra-articular step persisted in 16 %. Mean Böhler angle rose from 6.9° pre-operatively to 30° postoperatively and did not vary during the follow-up, which is proof of reduction stability. The rear-foot axis was restored in all cases, which confirmed the efficacy of the distractor and prevented severe disability and pain [18]. Secondary displacement was observed in one patient who decided to walk with full weight bearing in the immediate postoperative days. Even in intra-articular fracture type IIA or IIB), reduction was maintained at the final examination.
In our experience, functional results were obtained quickly with our technique and nail fixation. No degradation of results was observed between the 3rd and 12th clinical exams except in the three cases that required a secondary subtalar fusion. This could probably be explained by the strong fixation provided by the nail, with good anchorage within the subchondral bone.

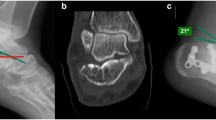
Fracture type IIB. a Intraoperative views showing guide-wire insertion, reduction using a bone pusher and locking nail insertion. b Comparison of pre- and postoperative computed tomography (CT) reconstructions: lateral (above) and anterior (below) views. Reduction was rated B. c Standard X-rays at 1-year follow-up
Involvement of the calcaneocuboid joint
The calcaneocuboid joint is involved in more than half the cases of DIACF [19]. Most often, pre-operative CT scans show a fracture separation line extending to the calcaneocuboid joint with or without minimal displacement, whereas comminution of the anterior part of the calcaneus with or without lateral joint subluxation is rather rare. Restoring calcaneus height and width using distraction contributes to restoring calcaneocuboid joint congruity; if needed, direct limited access to the calcaneocuboid joint is always possible, even if the Calcanail technique does not consider the anterior part of the calcaneal body. Moreover, calcaneocuboid involvement does not correlate with late outcomes [19]. The finite element analysis of calcaneal stress distributions [20] showed that when calcaneal height decreased by 5, 10, 15 or 20 mm, the maximal calcaneal stress increased by 10.4, 15.6, 35.4 and 54.7 %, with a gradual concentration towards the centre of the posterior articular facet. Stress concentration in the calcaneocuboid joint disappeared when calcaneal height decreased. This is why the authors claimed that calcaneal height should be restored to the normal level [20].
Biomechanical testing
Primary stability of the intramedullary calcaneal nail was compared with that of an angular stable calcaneal plate in an experimental model of standardised calcaneal fracture [21]. Results of using the bionic plate were not published at that time, and that plate cannot be used for comparison [22]. Stiffness in the calcaneal nail group was three times higher than in the calcaneal plate group. Moreover, Böhler angle was preserved in all nailed specimens but only in half of the plated specimens [21]. This emphasises the notion that an intramedullary calcaneal interlocking nail provides an utmost stable construct under clinical conditions, as well.
Primary subtalar fusion
Rammelt et al. [23] reported that fracture severity has a predictive value for functional outcome. Csizy et al. [24] showed that initial injury severity is the most predictive factor for late subtalar fusion. In our series, two of the three secondary fusions were necessary in two type IIB fractures, and satisfactory results were obtained within 12 months, which is 6 months later than primary subtalar arthrodesis. Primary fusion for severely comminuted intra-articular calcaneal fractures is an old idea that today has again gained acceptance. In six multifragment fractures (type IIB), we performed a primary subtalar arthrodesis (6 of 63; 9.5 %). Our results, with a mean AOFAS score of 75.6 (92 points), are similar to those in the Holm series [25], at an average of 78 points.
Study strengths and limitations
Strengths of this study are that data were collected continuously and prospectively, and patients were operated on by one of three experienced surgeons. Conversely, our study has several limitations. The first is the number of patients lost to follow-up; the second is the short follow-up period. However, it seems useful to report the preliminary results of this study and a new method for reduction and fixation of articular calcaneal fractures that has a very low complication rate. Moreover, functional results were obtained quickly, usually within six months, with no deterioration over time.
Conclusions
Decisive advantages are provided by this procedure and innovative implant: intrafocal reduction of thalamic fractures is effective and reliable; a locking calcaneal nail is able to maintain reduction of the subtalar articular surface; midterm functional results were satisfactory, and the complication rate was minimal. Long-term studies from other surgeons are needed to confirm these results and determine whether degenerative changes occur in the subtalar joint with longer follow-up.
References
Buckley RE, Tough S, Mc Cormack R et al (2002) Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: a prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 84-A:1733–1744
Howard JL, Buckley R, Mc Cormack R, Pate G, Leighton R, Petrie D, Galpin R (2003) Complications following management of displaced intra-articular calcaneal fractures: a prospective randomized trial comparing open reduction internal fixation with nonoperative management. J Orthop Trauma 17:241–249
Griffin D, Parsons N, Shaw E, Kulikov Y, Hutchinson C, Thorogood M, Lamb SE, UK Heel Fracture Trial Investigators (2014) Operative versus non-operative treatment for closed, displaced, intra-articular fractures of the calcaneus: randomised controlled trial. BMJ 349:g4483
Abidi NA, Dhawan S, Gruen GS et al (1998) Wound-healing risk factors after open reduction and internal fixation of calcaneal fractures. Foot Ankle Int 19:856–861
Baumgaertel FR, Gotzen L (1993) Two-stage treatment of comminuted os calcis fractures: primary indirect reduction with medial external fixation and delayed lateral plate fixation. Clin Orthop Relat Res 290:132
Bégué T, Mebtouche N, Auregan JC, Saintyves G, Levante S, Cottin P (2014) External fixation of the thalamic portion of a fractured calcaneus : a new surgical technique. Orthop Trauma Surg Res 100:429–432
Schepers T, Vogels LM, Schipper IB, Patka P (2008) Percutaneous reduction and fixation of intra-articular calcaneal fractures. Oper Orthop Traumatol 20:168–175
Walde TA, Sauer B, Degreif J, Walde HJ (2008) Closed reduction and percutaneous Kirschner wire fixation for the treatment of dislocated calcaneal fractures: surgical technique, complications, clinical and radiological results after 2-10 years. Arch Orthop Trauma Surg 128:585–591
Arastu M, Sheehan B, Buckley R (2014) Minimally invasive reduction and fixation of displaced calcaneal fractures: surgical technique and radiographic analysis. Int Orthop 38(3):539–545. doi:10.1007/s00264-013-2235-4
Abdelazeem A, Khedr A, Abousayed M, Seifeldin A, Khaled S (2014) Management of displaced intra-articular calcaneal fractures using the limited open sinus tarsi approach and fixation by screws only technique. Int Orthop 38(3):601–606. doi:10.1007/s00264-013-2203-z
Jacquot F, Atchabahian A (2011) Balloon reduction and cement fixation in intra-articular calcaneal fractures: a percutaneous approach to intra-articular calcaneal fractures. Int Orthop 35:1007–1014
Vittore D, Vicenti G, Caizzi G, Abate A, Moretti B (2014) Balloon-assisted reduction, pin fixation and tricalcium phosphate augmentation for calcanear fracture. Inj Suppl 6:S72–S79
Schepers T (2014) Towards uniformity in communication and a tailor-made treatment for displaced intra-articular calcaneal fractures. Int Orthop 38(3):663–665. doi:10.1007/s00264-013-2220-y
Goldzak M, Mittlmeier T, Simon P (2012) Locked nailing for the treatment of displaced articular fractures of the calcaneus: description of a new procedure with calcanail®. Eur J Orthop Surg Traumatol 22:345–349
Simon P, Goldzak M, Mittlmeier T (2013) Internal fixation or primary fusion in displaced articular fractures of the calcaneus: a new procedure with calcanail. Med Chir Pied 29:100–104
Sanders R, Vaupel ZM, Erdogan M, Downes M (2014) Operative treatment of displaced intra-articular calcaneal fractures: long-term (10-20 years) results in 108 fractures using a prognostic CT classification. J Orthop Trauma 28:551–563
Pan A, Chatterjee D, Garg AK, Mukhopadhyay KK, Banerjee K, Kumar S (2011) Percutaneous fixation of displaced intra-articular calcaneal fracture. J Indian Med Assoc 109:412–414
Rammelt S, Zwipp H (2013) Corrective arthrodeses and osteotomies for post-traumatic hindfoot malalignment: indications, techniques, results. Int Orthop 37(9):1707–1717. doi:10.1007/s00264-013-2021-3
Gallino RM, Gray AC, Buckley RE (2009) The outcome of displaced intra-articular calcaneal fractures that involve the calcaneocuboid joint. Injury 40:146–149
Wang YM (2014) Finite element analysis of calcaneus stress distributions with variant heights. Zhongguo Zuchi Gongcheng Yanjiu 18:6742–6746
Goldzak M, Simon P, Mittlmeier T, Chaussemier M, Chiergatti R (2014) Primary stability of an intramedullary calcaneal nail and an angular stable calcaneal plate in a biomechanical testing model of intra-articular calcaneal fracture. Injury 45S:S49–S53
Kinner B, Kerschbaum M, Bley C, Spiegel A, Roll C (2015) Bionic plate design for calcaneal fracture treatment. A biomechanical analysis and first clinical results. Int Orthop 39(1):111–117. doi:10.1007/s00264-014-2561-1
Rammelt S, Zwipp H, Schneiders W et al (2013) Severity of injury predicts subsequent function in surgically treated displaced intra-articular calcaneal fractures. Clin Orthop Relat Res 471:2885–2898
Csizy M, Buckley R, Tough S, Leighton R, Smith J, McCormack R, Pate G, Petrie D, Galpin R (2003) Displaced intra-articular calcaneal fractures. Variables predicting late subtalar Fusion. J Orthop Trauma 17:106–112
Holm JL, Laxson SE, Schuberth JM (2014) Primary subtalar joint arthrodesis for comminuted fractures of the calcaneus. J Foot Ankle Surg. doi:10.1053/j.fas.2014.07.013
Conflict of interest
The authors declare that they are co-owners of the patent of the device Calcanail®. No funds were received for editing this paper.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Simon, P., Goldzak, M., Eschler, A. et al. Reduction and internal fixation of displaced intra-articular calcaneal fractures with a locking nail: a prospective study of sixty nine cases. International Orthopaedics (SICOT) 39, 2061–2067 (2015). https://doi.org/10.1007/s00264-015-2816-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-015-2816-5