
Abstract
Purpose
The purpose of this study was to compare the clinical outcomes of patients undergoing total hip arthroplasty (THA) who had been using narcotic medications prior to surgery to those who had not used them.
Methods
Fifty-four patients (62 hips) who had required opioid analgesia for hip pain in the three months prior to THA were compared to a matched group of opioid-naïve patients. Narcotic consumption was converted to a standardized morphine equivalent dose and compared between both groups of patients during their hospital stay, after six weeks, and at final follow-up. Other outcome measures included clinical outcome scores and the proportion of patients remaining on narcotic pain medication at final follow-up.
Results
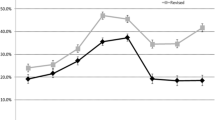
The narcotic group required significantly higher total daily opioid doses as inpatients had a longer hospital stay and a higher proportion of patients who remained on opioids at six weeks and at final follow-up. Of the patients who were taking opioids pre-operatively, 81 % were able to wean off opioids at final follow-up. At a mean post-operative follow-up of 58 months (range, 24–258 months), Harris hip scores were lower in the narcotic group, with a mean of 84 compared to 91 points in the matching group. However, in both cohorts, there were significant improvements in Harris hip scores compared to pre-operative outcomes.
Conclusions
Patients who use narcotics prior to total hip arthroplasty may be more likely to suffer from opioid-induced hyperalgesia after surgery and have worse clinical outcomes. When possible, efforts should be made to use other modes of analgesia or wean patients from their use prior to total hip arthroplasty.



Similar content being viewed by others
References
Lawrence RC, Felson DT, Helmick CG et al (2008) Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum 58(1):26
Helmick CG, Felson DT, Lawrence RC et al (2008) Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part I. Arthritis Rheum 58(1):15
American Geriatrics Society Panel on the Pharmacological Management of Persistent Pain in Older Persons (2009) Pharmacological management of persistent pain in older persons. Pain Medicine 10(6):1062
Gloth FM (2011) Pharmacological management of persistent pain in older persons: focus on opioids and nonopioids. J Pain 12(3 Suppl 1):S14
Zhang W, Moskowitz RW, Nuki G et al (2008) OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis Cartilage 16(2):137
Jordan KM, Arden NK, Doherty M et al (2003) Standing Committee for International Clinical Studies Including Therapeutic Trials E. EULAR Recommendations 2003: an evidence based approach to the management of knee osteoarthritis: Report of a Task Force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann Rheum Dis 62(12):1145
Glauser TA, Salinas GD, Roepke NL et al (2011) Management of mild-to-moderate osteoarthritis: a study of the primary care perspective. Postgrad Med 123(1):126
Webster BS, Verma SK, Gatchel RJ et al (2007) Relationship between early opioid prescribing for acute occupational low back pain and disability duration, medical costs, subsequent surgery and late opioid use. Spine (Phila Pa 1976) 32(19):2127
Lawrence JT, London N, Bohlman HH et al (2008) Preoperative narcotic use as a predictor of clinical outcome: results following anterior cervical arthrodesis. Spine (Phila Pa 1976) 33(19):2074
Lee M, Silverman SM, Hansen H et al (2011) A comprehensive review of opioid-induced hyperalgesia. Pain Physician 14(2):145
Guignard B, Bossard AE, Coste C et al (2000) Acute opioid tolerance: intraoperative remifentanil increases postoperative pain and morphine requirement. Anesthesiology 93(2):409
Chia YY, Liu K, Wang JJ et al (1999) Intraoperative high dose fentanyl induces postoperative fentanyl tolerance. Can J Anaesth 46(9):872
Ready LB (1996) Postoperative pain management–beyond basics. Can J Anaesth 43(2):193
Jamison RN, Taft K, O'Hara JP et al (1993) Psychosocial and pharmacologic predictors of satisfaction with intravenous patient-controlled analgesia. Anesth Analg 77(1):121
Lee A, Tsang CK, Siu HK et al (2008) Management of osteoarthritic pain in Hong Kong. Aust Fam Physician 37(10):874
Chu LF, Clark DJ, Angst MS et al (2006) Opioid tolerance and hyperalgesia in chronic pain patients after one month of oral morphine therapy: a preliminary prospective study. J Pain 7(1):43
Pereira J, Lawlor P, Vigano A et al (2001) Equianalgesic dose ratios for opioids. a critical review and proposals for long-term dosing. J Pain Symptom Manage 22(2):672
American Pain Society (2003) Principles of analgesic use in the treatment of acute pain and cancer pain. American Pain Society, Glenview, p 74
Chou R, Fanciullo GJ, Fine PG et al (2009) American Pain Society-American Academy of Pain Medicine Opioids Guidelines P. Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain. J Pain 10(2):113
Pergolizzi J, Boger RH, Budd K et al (2008) Opioids and the management of chronic severe pain in the elderly: consensus statement of an International Expert Panel with focus on the six clinically most often used World Health Organization Step III opioids (buprenorphine, fentanyl, hydromorphone, methadone, morphine, oxycodone). Pain Pract 8(4):287
Amstutz HC, Thomas BJ, Jinnah R et al (1984) Treatment of primary osteoarthritis of the hip. A comparison of total joint and surface replacement arthroplasty. J Bone Joint Surg Am 66(2):228
Harris WH (1986) Etiology of osteoarthritis of the hip. Clin Orthop Rel Res 213:20
Carragee EJ, Alamin TF, Miller JL et al (2005) MRI and psychosocial determinants of low back pain disability and remission: a prospective study in subjects with benign persistent back pain. Spine J 5(1):24
Buer N, Linton SJ (2002) Fear-avoidance beliefs and catastrophizing: occurrence and risk factor in back pain and ADL in the general population. Pain 99(3):485
IJzelenberg W, Burdorf A (2005) Risk factors for musculoskeletal symptoms and ensuing health care use and sick leave. Spine (Phila Pa 1976) 30(13):1550
Singh JA, Lewallen D (2009) Age, gender, obesity, and depression are associated with patient-related pain and function outcome after revision total hip arthroplasty. Clin Rheumatol 28(12):1419
Jordan JM, Linder GF, Renner JB et al (1995) The impact of arthritis in rural populations. Arthritis Care Res 8(4):242
Franklin PD, Karbassi JA, Li W et al (2010) Reduction in narcotic use after primary total knee arthroplasty and association with patient pain relief and satisfaction. J Arthroplasty 25(6 Suppl):12
Post ZD, Restrepo C, Kahl LK et al (2010) A prospective evaluation of 2 different pain management protocols for total hip arthroplasty. J Arthroplasty 25(3):410
Busch CA, Whitehouse MR, Shore BJ et al (2010) The efficacy of periarticular multimodal drug infiltration in total hip arthroplasty. Clin Orthop Rel Res 468(8):2152
Kahl L, Parvizi J, Viscusi ER et al (2010) Lessons learned with extended-release epidural morphine after total hip arthroplasty. Clin Orthop Rel Res 468(4):1082
Frassanito L, Rodola F, Concina G et al (2008) The efficacy of the psoas compartment block versus the intrathecal combination of morphine, fentanyl and bupivacaine for postoperative analgesia after primary hip arthroplasty: a randomized single-blinded study. Eur Rev Med Pharmacol Sci 12(2):117
Kidner CL, Mayer TG, Gatchel RJ et al (2009) Higher opioid doses predict poorer functional outcome in patients with chronic disabling occupational musculoskeletal disorders. J Bone Joint Surg Am 91(4):919
Disclosures
RP is a paid consultant for DJO.
BHK is a consultant for Sage products Inc.
PMB receives royalties from Arthrocare; Stryker; Synthes; Biomet; Joint Active Systems, Inc., Acacia Research Group, LLC, is a consultant for Stryker and Biomet, and has Stock or Stock options in Joint Active Systems, Inc.
MAM receives royalties from Stryker Orthopaedics; is a paid consultant for Johnson & Johnson, Sage Products, Medtronic, TissueGene, Stryker Orthopaedics, OnGoing Care Solutions, Inc. and Wright Medical Technologies, Inc.; and receives research support from National Institutes of Health (NIAMS and NICHD), Sage Products, Stryker Orthopaedics, TisseGene, and Wright Medical Technologies, Inc.
KI and QN have no disclosures.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pivec, R., Issa, K., Naziri, Q. et al. Opioid use prior to total hip arthroplasty leads to worse clinical outcomes. International Orthopaedics (SICOT) 38, 1159–1165 (2014). https://doi.org/10.1007/s00264-014-2298-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-014-2298-x