
Abstract
Purpose
To perform a comparative analysis of surgically resected mucinous cystic neoplasm (MCN) of pancreas and branch-duct type intraductal papillary mucinous neoplasms (BD-IPMN) considering clinico-radiological high-risk predictors for malignant tumors using the current management guidelines.
Materials and methods
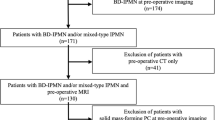
224 patients who underwent surgical resection and had histopathologically confirmed MCNs (benign 73; malignant 17) or BD-IPMNs (benign 110; malignant 24) and had pre-operative CT or MRI were retrospectively reviewed. Tumors classified as either high-grade dysplasia or invasive carcinoma were considered malignant, whereas those with low-grade dysplasia were considered benign. Imaging features were analyzed by two radiologists based on selected high-risk stigmata or worrisome features proposed by prevalent guidelines except tumors with main pancreatic duct dilatation (> 5 mm) were excluded.
Results
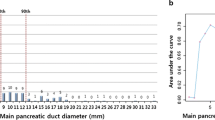
MCNs and BD-IPMNs showed significant differences in aspects like tumor size, location, the presence and size of enhancing mural nodules, the presence of wall or septal thickening, and multiplicity. Multivariate analyses revealed tumor size (OR, 1.336; 95% CI, 1.124–1.660, p = 0.002) and the presence of enhancing mural nodules (OR, 67.383; 95% CI, 4.490-1011.299, p = 0.002) as significant predictors of malignant MCNs. The optimal tumor size differentiating benign from malignant tumor was 8.95 cm, with a 70.6% sensitivity, 89% specificity, PPV of 27.6%, and NPV of 96.9%, demonstrating superior specificity than the guideline-suggested threshold of 4.0 cm. For malignant BD-IPMNs, the presence of enhancing mural nodules (OR, 15.804; 95% CI, 4.439–56.274, p < 0.001) and CA 19 − 9 elevation (OR, 19.089; 95%CI, 2.868-127.068, p = 0.002) as malignant predictors, with a size of enhancing mural nodule threshold of 5.5 mm providing the best malignancy differentiation.
Conclusion
While current guidelines may be appropriate for managing BD-IPMNs, our results showed a notably larger optimal threshold size for malignant MCNs than that suggested by current guidelines. This warrants reconsidering existing guideline thresholds for initial risk stratification and management of MCNs.





Similar content being viewed by others

Data availability
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
References
Gupta A, Chennatt JJ, Mandal C, et al. Approach to Cystic Lesions of the Pancreas: Review of Literature. Cureus 2023; 15
Xie W, Liang H, Guo Y, Xiao S-Y. Update on mucinous cystic neoplasm of the pancreas: a narrative review. Journal of Pancreatology 2021; 4:115–121
Pancreas ESGoCTot. European evidence-based guidelines on pancreatic cystic neoplasms. Gut 2018; 67:789–804
Valsangkar NP, Morales-Oyarvide V, Thayer SP, et al. 851 resected cystic tumors of the pancreas: a 33-year experience at the Massachusetts General Hospital. Surgery 2012; 152:S4-S12
Chang YR, Park JK, Jang J-Y, Kwon W, Yoon JH, Kim S-W. Incidental pancreatic cystic neoplasms in an asymptomatic healthy population of 21,745 individuals: large-scale, single-center cohort study. Medicine 2016; 95:e5535
Farrell JJ. Prevalence, diagnosis and management of pancreatic cystic neoplasms: current status and future directions. Gut and liver 2015; 9:571
Tanaka M, Fernández-del Castillo C, Kamisawa T, et al. Revisions of international consensus Fukuoka guidelines for the management of IPMN of the pancreas. Pancreatology 2017; 17:738–753
Tanaka M, Fernández-del Castillo C, Adsay V, et al. International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology 2012; 12:183–197
Pollini T, Marchegiani G, Facciorusso A, et al. It is not necessary to resect all Mucinous Cystic Neoplasms of the Pancreas: Current guidelines do not reflect the actual risk of malignancy A Systematic review and Meta-Analysis. HPB 2023;
Postlewait LM, Ethun CG, McInnis MR, et al. Association of preoperative risk factors with malignancy in pancreatic mucinous cystic neoplasms: a multicenter study. JAMA surgery 2017; 152:19–25
Park JW, Jang J-Y, Kang MJ, Kwon W, Chang YR, Kim S-W. Mucinous cystic neoplasm of the pancreas: is surgical resection recommended for all surgically fit patients? Pancreatology 2014; 14:131–136
Jang K-T, Park SM, Basturk O, et al. Clinicopathologic characteristics of 29 invasive carcinomas arising in 178 pancreatic mucinous cystic neoplasms with ovarian-type stroma: implications for management and prognosis. The American journal of surgical pathology 2015; 39:179
Goh BK, Tan Y-M, Chung Y-FA, et al. A review of mucinous cystic neoplasms of the pancreas defined by ovarian-type stroma: clinicopathological features of 344 patients. World journal of surgery 2006; 30:2236–2245
Ohtsuka T, Nakamura M, Hijioka S, et al. Prediction of the probability of malignancy in mucinous cystic neoplasm of the pancreas with ovarian-type stroma: a nationwide multicenter study in Japan. Pancreas 2020; 49:181–186
Elta GH, Enestvedt BK, Sauer BG, Lennon AM. ACG clinical guideline: diagnosis and management of pancreatic cysts. Official journal of the American College of Gastroenterology: ACG 2018; 113:464–479
Servin-Rojas M, Fong ZV, Fernandez-Del Castillo C, et al. Identification of high-risk features in mucinous cystic neoplasms of the pancreas. Surgery 2023; 173:1270–1274
Nilsson LN, Keane MG, Shamali A, et al. Nature and management of pancreatic mucinous cystic neoplasm (MCN): a systematic review of the literature. Pancreatology 2016; 16:1028–1036
Le Baleur Y, Couvelard A, Vullierme MP, et al. Mucinous cystic neoplasms of the pancreas: definition of preoperative imaging criteria for high-risk lesions. Pancreatology 2011; 11:495–499
Crippa S, Salvia R, Warshaw AL, et al. Mucinous cystic neoplasm of the pancreas is not an aggressive entity: lessons from 163 resected patients. Annals of surgery 2008; 247:571
Zamboni G, Scarpa A, Bogina G, et al. Mucinous cystic tumors of the pancreas: clinicopathological features, prognosis, and relationship to other mucinous cystic tumors. The American journal of surgical pathology 1999; 23:410–422
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
Conceptualization: Jung Hoon Kim. Data curation: HeeSoo Kim, Jihae An. Formal analysis: HeeSoo Kim, Jin Sol Choi. Funding acquisition: N/A. Investigation: Jihae An, HeeSoo Kim, Jin Sol Choi, Jung Hoon Kim. Methodology: HeeSoo Kim, Jung Hoon Kim. Project administration: HeeSoo Kim, Jung Hoon Kim. Resources: HeeSoo Kim, Jihae An, HeeSoo Kim. Software: HeeSoo Kim, Jihae An, Jin Sol Choi. Supervision: Jung Hoon Kim. Validation: HeeSoo Kim, Jihae An, Jin Sol Choi. Visualization: HeeSoo Kim, Jung Hoon Kim. Writing-original draft: HeeSoo Kim, Jihae An, Jung Hoon Kim. Writing-review & editing: HeeSoo Kim, Jihae An, Jin Sol Choi, Jung Hoon Kim.
Corresponding author
Ethics declarations
IRB statement
This retrospective study was approved by Seoul National University Hospital Institutional our institutional review board (IRB No. No 2210-130-1372), and patient informed consent was waived.
Conflict of interest
The authors of this manuscript have nothing to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kim, H., Kim, J.H., An, J. et al. Comparison with surgically resected mucinous cystic neoplasm of pancreas and branch-duct type intraductal papillary mucinous neoplasm considering clinico-radiological high-risk features: a reassessment of current guidelines. Abdom Radiol (2024). https://doi.org/10.1007/s00261-024-04364-y
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00261-024-04364-y