
Abstract
Objective
To investigate the feasibility of using Spectral CT imaging with low contrast medium in abdominal CT angiography (CTA).
Subjects and methods
70 consecutive patients (40 men, 42.6 ± 20.4 years; 30 women, 46.7 ± 18.8 years) with suspected abdominal focal lesions were referred to CTA exam. They were randomly assigned into two groups. Group A: 35 patients underwent conventional CT scan of Tube voltage 120 kVp, automatic current modulation with a Noise Index of 12, ASIR 30%, and injected with Iohexol (350 mgI/ml). Group B: 35 patients underwent Spectral CT Imaging, with Tube current of 600 mA, injected with Iodixanol (270 mgI/ml). The optimal mono-energy keV was achieved using the optimal contrast noise ratio in abdominal aorta at the renal artery level relative to the erector spine muscle. Both groups were injected with an injection rate of 3.5 ml/s, and a contrast volume of 1.5 ml/kg body weight. The Hounsfield units (HU) and noise of the bilateral renal arteries and muscle of both groups, as well as the optimal monochromatic image set of Group B were measured. Two radiologists assessed all images with a 5-points scale. CTDIvol and DLP were recorded. Data were analyzed using student t test.
Results
The total iodine intake of Group B was 28% lower than that of Group A. The CNR of abdomen artery, celiac trunk, superior mesenteric artery, and renal artery in spectral group (at the best mono-energy of 53.0 keV) were higher than those in conventional CTA group (p < 0.001). The subjective image quality score of spectral CTA group was also rated higher than conventional CTA group (p < 0.001). CTDIvol, DLP, and effective dose of spectral group were all lower than conventional group, but there were no significant differences (p > 0.05).
Conclusion
With 28% contrast medium reduction and reduced radiation dose, CT angiography using spectral imaging and lower concentration contrast agent provided better image quality than conventional CTA.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The upper abdominal is rich in blood supply, with the abdominal aorta branches into coeliac trunk, mesenteric artery, and bilateral renal artery. In presurgical evaluations, the blood supply to the focal lesions of abdominal organs needs to be clarified, to avoid potential bleedings during the surgery. Digital subtraction angiography (DSA) is the gold standard of vessel imaging, but DSA is an invasive exam with relative high cost, and it cannot display the lesion at the same time, which limits its usage in clinical practice [1]. CT angiography (CTA) is noninvasive and easy to perform with a short operation time. The hepatic tumor could be assessed with CTA before surgeries [2]. But use of contrast medium in patients with renal disease could induce contrast-induced nephropathy (CIN), which limits the clinical use of contrast medium [3]. With the advent of CT imaging, scanning using low energy could increase the contrast noise ratio (CNR) of the tissue, which makes it possible to further lower the contrast medium intake as well as radiation dose [4]. This study tried to apply dual energy spectral CT imaging, combined with low-concentration contrast medium, to investigate the feasibility of its application in upper abdominal artery CTA.
Materials and methods
Patient characteristics
Between April 2013 and June 2013, 70 consecutive patients (40 M, 30 F, mean age 52.2 ± 18.5, BMI 19.2–27.4) suspected of upper abdominal focal lesion were referred to tri-phase abdominal CTA in this prospective study. This study was approved by Institutional Review Board, and written informed consent was provided by each patient. The patients were randomly assigned into two groups: 35 patients were scanned with conventional CT (conventional group), and injected with Iohexol (350 mgI/ml); 35 patients were scanned with the dual energy gemstone spectral imaging (GSI) (spectral group), with Iodixanol (270 mgI/ml) as shown in Table 1.
Scan protocol
All CT examinations were performed with a 64-slice CT scanner (GE Discovery HD750). The patients were fasting 12 h before the exam. For both groups, patients were scanned in supine position, and the scan range was the entire upper abdomen. Conventional group: tube voltage 120 kVp, automatic tube current (0–500 mA), rotation speed 0.6 s/r, pitch 1.375, non-ionic contrast medium Iohexol (350 mgI/ml) was injected from cubital vein. Spectral group: single source dual energy scan, tube voltage switched between 80 and 140 kVp within 0.5 ms, tube current 600 mAs, rotation speed 0.6 s/r, pitch 1.375, non-ionic contrast medium Iodixanol (270 mgI/ml) was injected through the cubital vein. Both groups were injected with a contrast volume of 1.5 ml/kg body weight at a speed of 3.5 ml/s, followed by a saline flush of 30 mL. Smart Prep technique was used, with the ROI placed on the abdominal aorta, and the arterial phase was started 10 s after the ROI reaching the threshold of 110 HU. The scanning protocol is summarized in Table 2.
Image quality evaluation
Objective image assessment
One experienced radiologist post-processed the images of arterial phase on AW 4.5 Workstation using GSI Image browser. ROI was selected on the abdominal aorta on the same slice of coeliac trunk, and the background was selected on the erector spinae. The best mono-energy was computed as the one with the Optimal CNR. Measurements were made on abdominal aorta, coeliac trunk, mesenteric artery, and bilateral renal arteries (Each ROI was measured 3 times, and an average was computed). The ROI location, size, and shapes were as similar as possible, and on the same slice in both the spectral group and the conventional group. The CNR was computed as CNR = (CTartery − CTmuscle)/SDfat, in both groups, where CTmuscle was the HU value of the erector spinae muscle, and the noise was selected as the standard deviation of the abdominal subcutaneous fat [5].
Qualitative image analysis was performed on a workstation for the volume-rendering, three (axial, coronal, sagittal) orthogonal maximum intensity projections (MIP) and curved multiplanar reconstruction of the renal arteriography images. Two radiologists, with 6 and 3 years of experience, respectively, in visceral vascular imaging, assessed the over-all diagnostic image quality for the arteries using the following 5-point scale: 1, nondiagnostic image quality; 2, substandard image quality; 3, standard image quality; 4, better-than-standard image quality; or 5, excellent image quality. Arterial enhancement and the sharpness of the artery boundary were recorded using the following 5-point scale: 1, bad; 2, poor; 3, moderate; 4, good; or 5, excellent. The CT datasets were randomized, and the readers were blinded to the scanning parameters. If the readers’ scores were different, they would discuss to make agreements on the final scores. Before their assessments, the readers were also instructed on the criteria for image grading, and as a group they assessed five test cases that were not included in the study to reduce interobserver variability [6].
The CTDIvol and dose-length product (DLP) were recorded, and the effective dose (ED = DLP × k, where k = 0.0166 for male, 0.0146 for female [7]) was calculated for every patient.
Statistical analysis
All statistical analyses were performed using statistics software (SPSS, version 16.0, SPSS, Chicago, IL). The characteristics of the two patient groups (age, height, weight, and body mass index), the CTDIvol, DLP, ED, and the HU values and CNR of the upper abdominal major arteries were compared using the Student t test for unpaired samples. Wilcoxon Test was used to evaluate the difference between subjective image scores. Differences were considered significant when the p < 0.05.
Results
Characteristics of patients
There were no significant differences with respect to patient age, height, weight, and body mass index between the two groups (Table 1). Thus, further analysis and comparison of attenuation measurements and radiation exposure were considered to be feasible and valid.
Objective image quality
The optimal mono-energy keV with the best CNR image was 53 ± 1.8 keV, range 49–54 keV, with the best CNR selected across different energies as illustrated in Fig. 1. The attenuation values of the spectral group were higher than the conventional group (p < 0.001), while the image noise was higher as well (p < 0.001). CNR of Abdominal aorta, coeliac trunk, mesenteric artery, and renal arteries were 34.89, 30.58, 30.47, and 30.25, respectively, in the spectral group, which were significantly higher than the CNR of conventional group (24.36, 23.08, 21.50, and 21.18).with all p < 0.001) (Table 3).

Optimal keV selection: ROI was selected on the abdominal aorta on the same slice of coeliac trunk, and the background was selected on the erector spinae. Left image CNR vs. the mono-energy keV curve, X axis is keV, Y axis is the CNR. The best CNR was achieved at 53 keV marked by the red vertical line. Right image CT image of the optimal mono-energy 53 keV.
Subjective image quality
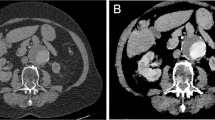
The subjective image quality score in artery enhancement or boundary sharpness of the spectral group was significantly higher than that of the conventional group, with p < 0.001 (Table 3). While in lesion diagnosis, the two groups showed no significant differences, with mean image score of 4.53 and 4.52, respectively. This result showed that spectral group had equal diagnostic value in lesion detection, but much higher values in showing the vasculature in upper abdominal (Fig. 2).

Comparison of MIP images using the conventional CT scanning and GSI spectral scanning mode. The upper row is the MIP image of the abdominal aorta at 52 keV in GSI mode (Window Level 400, Window Width 600). The lower row is the MIP image of the abdominal aorta in conventional scanning mode (Window Level 220, Window Width 210). GSI mode achieved better image quality and contrast than the conventional scanning mode.
Radiation dose and iodine intake
The average contrast medium intake of the spectral group (23,495.6 ± 57.39 mg) decreased 28% compared with the conventional group (32,565.3 ± 89.69 mg), with a statistical significance of 0.001. CTDIvol of the spectral group and conventional group in arterial phase were 14.99 ± 2.91 and 16.21 ± 5.27 mGy, respectively; DLP of the two groups were 497.6 ± 38.63 and 516.33 ± 157.27 mGy cm, respectively, and ED of the two groups were 7.61 ± 0.59 mSv and 8.05 ± 2.45, respectively. CTDIvol, DLP, or ED were lower in spectral group than in conventional group, but neither of them had statistically significant differences, with p = 0.238, 0.496, and 0.257, respectively.
Discussions
Our results showed that, better image quality and lower radiation dose were achieved using Dual Energy Spectral imaging than the conventional 120 kVp in abdominal CTA. Dual Energy Spectral Scanning with lower concentration Contrast Medium showed better image quality, with CNR of all arteries significantly higher in spectral group than in conventional group. HU values were also significantly higher in spectral group. Although the image noise increased, the subjective image score still increased about 16% in arteries due to the increased contrast.
Tube potential of 120 kVp was used in the conventional group, and 80/140 kVp switching was used in GSI spectral group. The best mono-energy was achieved at 53 keV with the highest CNR on different spectral energies. The CTDI, DLP, and ED were all lower in spectral group than in conventional group. Although there were no statistical differences between the radiation doses, the GSI spectral group had lower radiation than the conventional group.
Traditional CT used hybrid energy X-ray, when it goes through human body, low-energy radiation would be absorbed and generates beam hardening artifact, which makes the HU values “Drifting” [8], and affects the image quality. GSI uses single source fast kVp switching technique, with the two different energies of 40 and 140 kVp switching instantly, and could acquire paired images at the same time and the same projection angle. Mono-energy images have different characteristics on different energy levels. Low keV X-ray is less penetrable, with high contrast on tissue, but with higher noise; High keV X-ray is more penetrable, with less beam hardening effect, but lower contrast as well. HU values of iodine change significantly on different X-ray energies, while soft tissue HU values change much less. Thus under low keV, the HU values of artery with contrast medium increase significantly, while HU values of surrounding soft tissue remains relatively unchanged [9], which increase the contrast. Ren et al. [10] showed that 70 keV mono-energy image could increase the contrast between tumor and hepatic parenchyma, which is helpful to the detection of small lesions.
For patient safety, the amount of iodine dose and radiation dose should be minimized with adequate diagnosis. Although with the lowering of radiation energy, the image noise increases, GSI CT could automatically compute the best CNR of a ROI relative to the background, and select the optimal mono-energy image with high contrast as well as acceptable image noise. Matsumoto et al. [11] showed that under a given radiation dose, images of 70 keV using Spectral CT had relatively lower image noise and higher CNR than those of traditional 120 kVp. Our study showed that (53 ± 1.8) keV achieved the optimal CNR, which showed best contrast between coeliac trunk and erector spine muscle, without too much noise using the GSI viewer. Under this mono-energy, the CNR using the low-concentration contrast media could be 30% higher than the conventional group in abdominal aorta, coeliac trunk, mesenteric artery, and renal artery. Although the image noise increased slightly, the subjective image score still increased 16% due to the increased contrast.
CTA is noninvasive, inexpensive and easy to perform compared with DSA [12], and could display the surrounding organs. In CTA Blood vessels, soft tissue, and lesions were enhanced differently, which helped diagnosis [13]. Iodine concentration is one of the most important factors affecting the tissue enhancements [14]. To increase the image quality of arteries, higher contrast agent concentration, volume as well as injection rate are used traditionally, but higher iodine intake could also introduce adverse effects, such as CIN. CIN is the 3rd most common cause of hospital-acquired acute renal failure [15]. The occurrence rate of CIN is 3.3–8% for patients without previous renal dysfunction [16]. Rihal et al. in a prospective study of 7586 patients, found out that the higher the base SCR level, the higher the occurrence of CIN [17]. Abujudeh et al. showed that large volume (>5 ml/kg) or repetitive use of contrast media could increase the occurrence of CIN [18]. Some patients could bear permanent damage of kidney after contrast injection, like patients having severe kidney diseases. Study showed that the incidence of CIN after CT in hospitalized oncological patients could be as high as 20% due to recent chemotherapy or hypertension [19]. Thus, it is important to reduce the iodine intake without affecting image quality. In our study, the iodine volume of spectral group was 28% lower than the conventional group, which could greatly increase the renal safety in abdominal CTA.
To summarize, compared with conventional CT scanning, GSI CT spectral scanning used fewer iodine contrast media (with an average drop of 28%) and less radiation dose, and came out with better image quality in abdominal imaging. CT spectral scanning should be recommended in patients with kidney disease.
Some limitations of this study: the sample sizes were not big enough, more samples with larger range of BMI (>28) will be collected in our future study. Also, with the development of CT spectral scanning technology, the tube current could be lowered further to reduce more radiation dosage.
References
Li J, Tang GS, Huang Y, et al. (2009) Application of digital subtraction angiography and interventional treatment in gastrointestinal arterial hemorrhage. Chin J Gastrointest 12(3):252–256
Huang L, Zheng P, Mao J, Li F, Zheng Y., Cheng Z (2014) Application value of three-dimensional surgery planning system in the preoperative evaluation of primary liver cancer resection. Chin J Hepat Surg 3(2), 79–83
Mehran R, Nikolsky E (2006) Contrast-induced nephropathy: definition, epidemiology, and patients at risk. Kidney Int Suppl 100:S11–S15
Yuan R, Shuman WP, Earls JP, et al. (2012) Reduced iodine load at CT pulmonary angiography with dual-energy monochromatic imaging: comparison with standard CT pulmonary angiography—a prospective randomized trial. Radiology 262(1):290–297
Marin D, Nelson RC, Schindera ST, et al. (2010) Low-tube-voltage, high-tube-current multidetector abdominal CT: improved image quality and decreased radiation dose with adaptive statistical iterative reconstruction algorithm-initial clinical experience. Radiology 254(1):145–153
Cho E-S, Yu J-S, et al. (2012) CT angiography of the renal arteries: comparison of lower-tube-voltage CTA with moderate-concentration iodinated contrast material and conventional CTA. Genitourin Imaging 199:96–102
Liu B, Bai M (2010) Variations of effective dose for head, thoracic, abdomen and coronary CT examinations according to new ICRP publication. Chin Med Equip J 31(03):27–31
Stolzmann P, Scheffel H, Rentsch K, et al. (2008) Dual-energy computed tomography for the differentiation of uric acid stones: exvivo performance evaluation. Urol Res 36(3–4):133–138
Zhang Z, Lu G (2007) Dual source computed tomography and its clinical application. J Med Postgrad 20(4):416–418
Ren Q, Hua Y, Li J (2011) The basic principle and clinical applications of CT spectral imaging. Int J Med Radiol 34(6):16
Matsumoto K, Jinzaki M, Tanami Y, et al. (2011) Virtual monochromatic spectral imaging with fast kilovoltage switching: improved image quality as compared with that obtained with conventional 120-kVp CT. Radiology 259(1):257–262
Sun Y, Mao D, Li M, et al. (2013) The value of CT angiography before transchatheter in the use of chemoembolization of hepatocellular carcinoma using dual-energy CT. J Med Imaging 23(11):1718–1723
Fenchel S, Fleeter TR, Aschoff AJ, et al. (2004) Effect of iodine concentration of contrast media on contrast enhancement in multislice CT of the pancreas. Br J Radiol 77:821–830
Chen X, Xie Q, Wei C, et al. (2009) Comparison of two iodine concentration of contrast media on contrast enhancement in multislice CT of kidney. Prog Mod Biomed 9(13):2528–2530
Wong GT, Irwin MG (2007) Contrast-induced nephrohathy. Br J Anaesth 99:474–483
Bickham P, Golembiewski J (2010) Contrast media use in the operation room. J Perianestbesia Nurs 25:94–103
Rihal CS, Textor SC, Grill DE, et al. (2002) Incidence and prognostic importance of acute renal failure after percutaneous coronary intervention. Circulation 105(19):2259–2264
Abujudeh HH, Gee MS, Kaewlai (2009) In emergency situations, should serum creatinine be checked in all patients before performing second contrast CT examinations within 24 hours. J Am Coll Radiol 6(4):268–273
Balemans CEA, Reichert LJM, van Schelven BIH, van den Brand JAJG, Wetzels JFM (2012) Epidemiology of contrast material-induced nephropathy in the era of hydration. Radiology 263(3):706–713
Acknowledgments
The study was partly supported by the research project “Application of Low Concentration Contrast Agent (Iodixanol 270) and Gemstone Spectral CT in abdominal arteries and organs,” under grant no. 201301090, from the Shanxi Province Minister of Health.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Xin, L., Yang, X., Huang, N. et al. The initial experience of the upper abdominal CT angiography using low-concentration contrast medium on dual energy spectral CT. Abdom Imaging 40, 2894–2899 (2015). https://doi.org/10.1007/s00261-015-0462-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-015-0462-4