
Abstract
Purpose
The prognostic value of the tumor-to-liver uptake ratio (TLR) from 18-fluoro-2-deoxyglucose positron emission tomography/computed tomography (18F–FDG-PET/CT) in the early stage of colorectal cancer (CRC) is unclear. Notably, some stage IIA CRC patients experience early recurrence even after curative resection and might benefit from neoadjuvant or adjuvant chemotherapy. This study aims to evaluate whether elevated TLR from 18F–FDG-PET/CT can predict poor prognosis in stage IIA CRC patients undergoing curative resection.
Methods
From April 2010 to December 2013, 504 consecutive CRC patients with different TNM stages (I-IV) underwent 18F–FDG-PET/CT scans at the 6th Affiliated Hospital of Sun Yat-Sen University. Among the patients, 118 with stage IIA CRC who accepted preoperative 18F–FDG-PET/CT scanning and were treated with curative surgery alone were reviewed retrospectively. The maximum standardized uptake value (SUVmax) in the primary tumor, TLR, and demographic, clinical, histopathological, and laboratory data were analyzed. Receiver operating characteristic (ROC) curve, univariate and multivariate analyses were performed to identify prognostic factors associated with patient disease-free survival (DFS) and overall survival (OS).
Results
ROC curve analysis demonstrated that TLR was superior to primary tumor SUVmax in predicting the risk of recurrence in stage IIA CRC. The optimal TLR cutoff was 6.2. Univariate analysis indicated that elevated TLR, tumor size, and lymphovascular/neural invasion correlated with DFS (P = 0.001, P = 0.002, and P = 0.001, respectively) and OS (P = 0.001, P = 0.003, and P < 0.001, respectively). The 1-, 3-, and 5-year DFS rates were 98.4%, 96.9%, and 96.9% for stage IIA CRC patients with lower TLR (≤6.2) versus 77.8%, 60.6%, and 60.6% for those with elevated TLR (>6.2), respectively. The 1-, 3-, and 5-year OS rates were 100.0%, 100.0%, and 98.3% for the patients with lower TLR versus 98.1%, 83.3%, and 74.3% for those with elevated TLR. Cox regression analysis showed that elevated TLR [>6.2; hazard ratio (HR): 3.109–57.463; P < 0.001] and tumor size (>4.4 cm; HR: 1.636–19.155; P = 0.006) were independent risk factors for DFS. Meanwhile, elevated TLR (>6.2; HR: 1.398–84.945; P = 0.023) and lymphovascular/neural invasion (positive; HR: 1.278–12.777; P = 0.017) were independent risk factors for OS.
Conclusion
Elevated TLR predicted worse DFS and OS for stage IIA CRC patients and might serve as a potential radiological index to identify candidates for neoadjuvant or adjuvant chemotherapy. Stage IIA CRC patients with elevated TLR should be monitored carefully for early detection of possible recurrence.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Colorectal cancer (CRC) is now the fourth leading cause of cancer-related death worldwide [1]. Curative resection is the standard treatment for stage I and II CRC. However, for stage II CRC, 12–20% of patients will develop recurrence within 5 years after curative resection [2, 3]. According to the 7th AJCC classification, stage II CRC is divided into IIA, IIB, and IIC based on peritoneal involvement and invasion to other organs [4]. Adjuvant chemotherapy is recommended for stage II CRC patients with a high risk of recurrence, such as low histological differentiation, vascular or lymphatic invasion, nerve tract invasion, examined lymph node number less than 12, and preoperational intestinal obstruction. The above risk factors are all based on pathological examination after surgery. Currently, neoadjuvant chemotherapy is recommended for stage IIB and IIC CRC patients with T (tumor invasive depth) >5 mm [5]. However, the role of neoadjuvant or adjuvant chemotherapy in stage IIA CRC remains unclear [6]. It is, therefore, critical to identify reliable preoperational prognostic radiological factors for stage IIA CRC to facilitate the identification of patients at high risk of recurrence who might benefit from neoadjuvant or adjuvant chemotherapy.
18-fluoro-2-deoxyglucose positron emission tomography/computed tomography (18F–FDG-PET/CT) has been widely used for the initial staging of CRC, for restaging recurrence and for monitoring the response to therapy, and it has become the standard imaging tool for this purpose [7]. Previous studies have shown that the metabolic volumetric parameters in 18F–FDG-PET/CT have prognostic value in various cancers, including CRC, lung cancer, breast cancer, malignant melanoma, and endometrial cancer [8,9,10,11,12,13]. In addition, tumor maximum standardized uptake value (SUVmax) has been reported to be a strong predictor of survival in patients with various types of cancer [14, 15]. SUVmax has also been associated with chemotherapy response. Patients whose SUVmax has been normalized by chemotherapy achieve survival rates similar to patients with normal SUVmax [8]. The tumor-to-liver uptake ratio (TLR) has recently been reported to be more precise in evaluating treatment response [16,17,18,19,20]. However, data regarding the prognostic significance of TLR or SUVmax in stage IIA CRC have not been reported. We, therefore, designed this retrospective study to investigate the prognostic significance of TLR and tumor SUVmax in stage IIA CRC patients who have undergone curative resection without neoadjuvant or adjuvant chemotherapy.
Methods
Patients
From April 2010 to December 2013, 504 patients underwent preoperative 18F–FDG-PET/CT at the 6th Affiliated Hospital of Sun Yat-sen University. Among these patients, 118 patients who were diagnosed with stage IIA (T3N0M0) CRC according to the 7th edition of the AJCC staging system after curative surgery were enrolled in this study [4]. All patients had biopsy-proven CRC by preoperative full colonoscopy. Curative resection was defined as no macroscopic or histological evidence of clearance of the primary tumor and no evidence of distant metastasis. All operations were performed within 15 days after 18F–FDG-PET/CT acquisition. Patients with the following characteristics were excluded: (1) multiple primary malignancies; (2) receipt of neoadjuvant therapy (chemotherapy with or without radiotherapy) or adjuvant chemotherapy; (3) hereditary nonpolyposis colorectal cancer or familial adenomatous polyposis; (4) coexistent preoperative uncontrolled infection. The patients’ demographic, clinical, histopathological, imaging, and laboratory data were collected. All blood tests were performed within 1 week before surgery.
18F–FDG-PET/CT imaging acquisition
All patients fasted for at least 6 h before examination. The blood glucose concentration was managed at less than 150 mg/dL in all patients. Approximately 5.5 MBq of 18F–FDG per kilogram of body weight was administered by intravenous injection. PET/CT scans of all patients were performed within 1–2 h after FDG injection using a Biograph True Point 40-slice CT apparatus (TrueD, Siemens Health Care, Erlangen, Germany). Before the PET scan, for attenuation correction, a low-dose CT scan was obtained without contrast enhancement with the patient supine and breathing quietly. The CT scan was performed from the neck to the pelvis or from the skull to the feet with a voltage of 120 keV and a tube current of 80 mA. PET scans were acquired in three-dimensional mode. PET images were acquired over the corresponding area with a 16.2 cm axial field of view at 2.0 min per bed position using Biograph True Point 40 PET/CT scanners and reconstructed with a 128X128 matrix, an ordered-subset expectation maximum iterative reconstruction algorithm (four iterations, eight subsets), and a Gaussian filter of 5.0 mm. The SUVmax of primary tumors and liver was determined using the volume viewer software on a Siemens Syngo Multi-Modality Workplace (TrueD, Siemens Health Care, Erlangen, Germany). All images were evaluated independently by two experienced radiological doctors.
Image interpretation
18F–FDG-PET/CT findings were reviewed on the workstation by two board-certified medical physicians (Dr. Zhanwen Zhang & Dr. Xiaoyan Wang) with more than 10 years of clinical experience in colorectal cancer imaging. The physicians identified visible lesions with high tracer uptake and then quantified the 18F–FDG uptake. SUV was used to determine the activity of 18F–FDG-PET. SUV was determined using the equation SUV = A/(ID/BW), where A is the decay-corrected activity in the tissue (in millicuries per milliliter), ID is the injected dose of FDG (in millicuries) and BW is the patient body weight (in grams). Spherical or ellipsoidal ROIs were placed over the visible lesions and liver on PET images. The ROIs of the malignant lesions and liver that were invisible on PET images were located using the corresponding CT images. The tumor SUVmax was calculated by drawing an ROI over the most intense slice of the visible primary tumor on PET images. The liver SUVmax was calculated by drawing a circular ROI 3.0 cm in diameter over the relatively homogenous intense slice of the right lobe of normal liver parenchyma on PET images, avoiding the partial volume effect (PVE) caused by adjacent organs on the margins of the liver; the liver SUVmax of each patient was measured three times, and the mean value was calculated to further reduce selection bias. TLR was defined as the ratio of primary tumor SUVmax to individual liver SUVmax. All the calculations were performed by the two experienced physicians mentioned above.
Surgical resection and pathological examination
All primary tumor surgical resections and mesenteric lymph node dissections were performed by experienced colorectal surgeons. The resected tumor tissue and lymph nodes were examined by a histopathologist for the presence or absence of malignancy using standard techniques. Two investigators independently evaluated the pathological images. In the small subset of cases in which there were significant differences in the initial interpretations, final diagnoses were assigned by consensus.
Follow-up
All patients underwent follow-up from the day of discharge after surgery. Patients were reexamined every three months within the first year, every 3 to 6 months for the next 2 years, and once annually thereafter. Physical examination and serum carcinoembryonic antigen (CEA) determination were performed routinely at each follow-up. Patients received a full colonoscopy every 6 months from surgery. Enhanced chest and abdominal CT scans, abdominal ultrasound and pelvic MRI were performed at each follow-up. Recurrence was defined as evidence of clinical, radiological or pathological diagnosis of tumor from previous CRC locally or distantly. 18F–FDG-PET/CT was added when clinically indicated. Disease-free survival (DFS) was calculated from the date of surgery to the date of the first confirmation of recurrence or the last clinical contact attesting to recurrence-free status. Follow-up was completed by December 31, 2016.
Statistical analysis
Continuous data were described as the mean ± standard deviation and analyzed using an independent sample T-test. Categorical data are presented as the frequency and percentage and were analyzed using Pearson’s Chi square test. ROC analysis was performed to determine the optimal cutoff of primary tumor SUVmax, TLR and tumor size for the prediction of recurrence. Univariate analysis for DFS was performed using the Kaplan-Meier method. The log-rank test and Cox regression analysis were used to identify factors significantly associated with DFS. Factors found to be statistically significant in the log-rank test were entered into a stepwise Cox regression model to obtain a final model of independent prognostic factors. A P value of less than 0.05 was considered statistically significant (IBM SPSS 23.0 and GraphPad Prism 6.0 for Mac).
Results
Clinicopathological characteristics
Of the 118 stage IIA (pT3N0M0) CRC patients, 70 (59.3%) were male and 48 (40.7%) were female. The median age of the cohort was 63.0 years (range, 28 to 86 years). The primary tumor was located in the right colon in 35 cases (29.7%), left colon in 38 cases (32.2%) and the rectum in 45 cases (38.1%). Regarding the histological differentiation of the tumors, 105 (89.0%) were well/moderately differentiated, and 13 (11.0%) were poorly differentiated carcinomas. Mucinous or signet-ring cell type carcinoma was observed in 11.0% (13/118) of the patients. The tumor size ranged from 1.0 to 8.5 cm with a median size of 4.5 cm. The demographic and biochemical characteristics of the subjects are shown in Table 1.
The patients underwent follow-up for 52.9 ± 22.8 (3.1–81.63) months. Of the 118 patients, recurrence was detected in 23 (19.5%) patients. Among the 23 patients with recurrence, local recurrence occurred in three (13.0%), liver metastasis in 11 (47.8%), lung metastasis in six (26.1%), liver and para-aortic lymph node metastasis in one (4.4%), and peritoneal carcinomatosis in two (8.7%).
PET metabolic parameters
The primary tumor SUVmax had no significant relationship with TNM stage in CRC. The comparison of the primary tumor SUVmax in all 504 CRC patients with different TNM stages who underwent 18F–FDG-PET/CT examination is shown in Fig. 1.

Primary tumor SUVmax comparison among different stages of CRC according to the 7th Edition of AJCC
SUVmax in stage IIA CRC ranged from 4.2 to 37.3, with a median value of 15.10 ± 7.85. The liver SUVmax value ranged from 1.4 to 3.6, with a median of 2.45 ± 0.40. TLR ranged from 1.8 to 22.2, with a median value of 5.68 ± 3.25. Tumor SUVmax and TLR were significantly higher in patients with recurrence than in those without (P < 0.001 and P < 0.001, respectively). The comparison of the clinicopathological features of patients with and without elevated TLR is shown in Table 2.
ROC curve analysis
The ability of primary tumor SUVmax, TLR, and tumor size to predict recurrence was depicted by the ROC curve. The optimal cutoff values of 15.85 for SUVmax (95% CI: 0.650–0.868, AUC, 0.759), 6.2 for TLR (95% CI: 0.674–0.885, AUC, 0.779), and 4.4 cm for tumor size (95% CI: 0.613–0.816, AUC, 0.714) were determined using ROC curve analysis. Consequently, SUVmax, TLR, and tumor size were examined as prognostic parameters for predicting recurrence. SUVmax and TLR quantification had qualitatively equal results in 91.5% (108/118) of the patients, but there were contrary identifications in 8.5% (10/118) of the patients. The ROC curve showed that TLR had better predictive performance than tumor SUVmax for predicting recurrence (Fig. 2).

Comparison of TLR and tumor SUVmax in stage IIA CRC patients by ROC (receiver operating characteristic) curves. ROC curves were used to determine the cutoff values for TLR, tumor SUVmax and tumor size in stage IIA CRC patients. a: AUC 0.759 (P < 0.001, 95% CI 0.650–0.868), cutoff value 15.85 for SUVmax; b: AUC 0.779 (P < 0.001, 95% CI 0.674–0.885), cutoff value 6.2 for TLR; c: AUC 0.714 (P = 0.001, 95% CI 0.613–0.816), cutoff value 4.4 cm for tumor size; d: plot of SUVmax vs. TLR in individual patients (0 indicates cases with SUVmax/TLR lower than the cutoff value, and 1 indicates cases with SUVmax/TLR higher than the cutoff value)
Univariate and multivariate analysis of survival
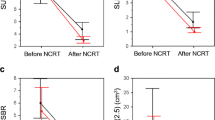
The 1-, 3-, and 5-year DFS rates were 98.4%, 96.9%, and 96.9% for stage IIA CRC patients with lower TLR (≤6.2) versus 77.8%, 60.6%, and 60.6% for those with elevated TLR (>6.2), respectively (Fig. 3a). The 1-, 3-, and 5-year overall survival (OS) rates were 100.0%, 100.0%, and 98.3% for patients with lower TLR versus 98.1%, 83.3%, and 74.3% for those with elevated TLR (Fig. 3).

Disease-free survival and overall survival of patients with stage IIA CRC stratified by TLR, tumor size and lymphovascular/neural invasion
Univariate analyses showed that TLR, tumor size and lymphovascular/neural invasion were independent risk factors for both DFS and OS in stage IIA CRC. There were no significant differences in age, gender, tumor site, mucinous carcinoma, number of lymph nodes sampled, histological differentiation, and tumor markers (CEA, CA125, and CA199) between patients with recurrence and those without (Table 3).
Multivariate Cox regression analysis identified elevated TLR (>6.2) and tumor size (>4.4) as independent prognostic factors associated with DFS, whereas elevated TLR (>6.2) and lymphovascular/neural invasion (positive) were independent risk factors for OS stage IIA CRC. The hazard ratios (HRs) calculated for each of these variables are shown in Table 4. Multivariate analysis revealed that the above risk factors remained statistically significant after adjusting for well-known clinicopathological parameters, including age, tumor site, histological differentiation, and tumor markers (data not shown).
Discussion
Our study is the first to report that TLR and tumor SUVmax have potential clinical significance in predicting recurrence in stage IIA CRC. Metabolic parameters from 18F–FDG-PET/CT, such as SUVmax, have previously been reported as strong prognostic factors for a number of malignancies, including lung cancer, esophageal cancer, lymphoma, cervical cancer, and intrahepatic cholangiocarcinoma [8, 21,22,23,24,25,26]. Moreover, elevated SUVmax in the primary tumor has been associated with poor prognosis in patients with CRC [27, 28]. 18F–FDG uptake has been identified as a significant prognostic factor correlated with prognosis in patients with CRC: the more metabolically active the tumor, the worse the outcome [29]. However, Lee et al. showed that SUVmax had no significant relationship with recurrence and DFS in patients with resectable tumors by both single- and multi-factor analysis [11]. These previous studies included subjects with different tumor stages (stage I to IV) and heterogeneous histological types who received various therapeutic modalities, including surgery, radiation, and chemotherapy. Whether the metabolic parameters obtained from 18F–FDG-PET/CT vary in different stages of CRC and their prognostic function in the early stage of CRC remained unclear. In the present study, we first analyzed the primary tumor SUVmax in all 504 CRC patients who underwent 18F–FDG-PET/CT examination, which revealed no relationship of primary tumor SUVmax with TNM stage in CRC (Fig. 1). Furthermore, all stage IIA CRC patients who underwent only curative resection were enrolled, thus avoiding the bias caused by the inclusion of multiple therapeutic factors in previous studies. We observed that TLR, tumor SUVmax and tumor size had prognostic value in predicting recurrence in stage IIA CRC (Table 1 & Fig. 2).
This study is the first to report the prognostic value of preoperative 18F–FDG-PET in stage IIA CRC. In addition, the present study provides the largest consecutive series of stage IIA CRC patients undergoing preoperative FDG-PET examination, which is normally performed on patients with locally advanced or metastatic tumors. Recurrence of CRC in the early stage has long troubled both patients and doctors. However, in the absence of preoperative prognostic parameters to predict the outcome of patients with early-stage tumors, identifying patients with early-stage tumors at high risk of recurrence has remained challenging. Murakami [30] reported that preoperative 18F–FDG-PET had prognostic value in stage IA lung adenocarcinoma. 18F–FDG uptake has been identified as a significant prognostic factor showing correlation with prognosis in patients with CRC cancer: the more metabolically active the tumor, the worse the outcome [29]. In our study, all stage IIA CRC patients who underwent only curative resection were enrolled. We observed recurrence occurred significantly earlier in patients with elevated TLR or SUVmax. In addition, the most discriminative cutoff value of SUVmax for predicting recurrence was 15.85, higher than our previously reported SUVmax in CRC for all TNM stages [22]. The difference in the cutoff value between the present and the previous study might be due to differences in the enrolled subjects.
Despite the convenience of its measurement and wide use, SUVmax is biased by many factors, including body composition and habitus, development time and injection dose of developer, length of FDG uptake period, plasma glucose, recovery coefficient, tumor volume, and volume of interest [31]. Additional limitations of SUVmax for representing the glucose metabolic rate of tumors are its susceptibility to the influences of noise, partial volume effect, image resolution, and definition of the volume of interest; SUVmax is a single-voxel value representing the most intense FDG uptake in the tumor [32, 33]. Therefore, SUVmax may not be an adequate surrogate marker representing the metabolic rate of the tumor, and other metabolic parameters that can predict prognosis should be further explored. The mediastinum vessel and normal liver tissue are the most frequent candidates for normal tissue [34]. In the current study, we used the SUVmax from normal liver tissue as the individual background. Normalization using normal tissue uptake might reduce the effect of individual bias on TLR. We found that TLR was superior to tumor SUVmax in predicting recurrence, which is of potential clinical significance (Fig. 2). As an independent prognostic factor, TLR >6.2 indicated poor prognosis with a relatively high HR (Table 4).
Tumor size (maximum) can reflect the tumor volume. Larger tumors contain more tumor cells than smaller tumors, thus requiring a greater glucose supply to maintain the metabolism and proliferation of tumor cells, which would result in an increase in SUVmax. The maximum tumor size has previously been related to tumor SUVmax [35], and our data also identified tumor size as a risk factor for CRC prognosis (Tables 1, 3). Riedl et al. reported that SUV was related to GLUT1, Ki67, and P53, which reflect tumor glucose metabolism and the tumor cell proliferation rate, and found that patients with colorectal liver metastasis (CRLM) and a higher SUVmax had a shorter OS than those with a lower SUVmax [36]. SUV had a positive correlation with Ki67. Decreased tumor differentiation is associated with faster proliferation and higher Ki67 expression. The SUVmax was higher in low-differentiation tumors than in high-differentiation tumors. In this study, we confirmed that TLR was related to the differentiation of stage IIA CRC. The TLR and SUVmax were significantly higher in lower-differentiation tumors than in higher-differentiation tumors (Table 2). However, we did not identify histology as a prognostic factor, consistent with studies focusing on T3 N0 CRC (Table 3) [37, 38]. Notably, we also found that TLR was related to lymphovascular/neural invasion in stage IIA CRC. Patients with elevated TLR suffered more lymphovascular/neural invasion than those with lower TLR (Table 2). A similar finding was reported for earlier CRC, such as stage I CRC [39].
The benefit of neoadjuvant or adjuvant therapy in stage IIA CRC remains unclear. Routine administration of neoadjuvant or adjuvant chemotherapy is not currently recommended for stage II CRC patients after curative resection outside of clinical trials, except for patients with “high-risk factors”, including T4 tumor, bowel obstruction or perforation at diagnosis, lymphovascular invasion, poor differentiation and inadequate lymph node sampling [40]. In this study, 96.9% of patients with normal TLR experienced 5-year DFS, similar to that of stage I CRC patients [41,42,43]. However, patients with elevated TLR had a cumulative 5-year DFS of only 60.6%, similar to that of stage IIIB CRC patients in previous reports [41,42,43]. Thus, we consider elevated TLR a risk factor for early-stage CRC that may warrant consideration for neoadjuvant or adjuvant chemotherapy. In a CRC mouse model, Burt et al. observed a positive correlation of the radioactive FDG concentration in the tumor with the tumor proliferation rate, suggesting that FDG imaging can be used in clinical staging and also in the evaluation of the prognosis and therapeutic effect of adjuvant chemotherapy [44]. Recent studies have also shown that molecular and biochemical markers, such as KRAS mutation, p53 mutations, microsatellite instability (MSI), and disseminated circulating tumor cells, may be used more precisely to define prognosis and predict benefit of neoadjuvant treatment in CRC [45]. However, none of these markers are currently in clinical application for determining whether patients with stage IIA CRC should receive neoadjuvant or adjuvant chemotherapy. The prediction of recurrence in patients with stage IIA CRC might contribute to the decision for neoadjuvant or adjuvant chemotherapy to prevent or delay of recurrence. Of note, chemotherapy has been reported to normalize elevated SUVmax in patients with primary or metastatic CRC, resulting in significantly improved survival compared with that of patients whose elevated SUVmax has not been normalized [29, 46, 47]. Moreover, TLR has been proven to have predictive value for chemotherapeutic response in lymphoma [48, 49]. Thus, based on our findings, TLR might be a useful radiological index for determining the optimal personalized therapeutic policy and might contribute to the improvement of outcomes in stage IIA CRC patients. In addition, TLR might serve as a potential predictor of response to chemotherapy.
However, we acknowledge that our study has some limitations. First, this was a retrospective study with a relatively small number of patients. Further prospective studies with larger patient numbers would provide more definitive data to clarify the significance of our findings. Second, although a previous study showed that SUVmax is a predictor of response to chemotherapy, we did not have sufficient data in the present study to prove that stage IIA CRC patients with elevated TLR could benefit from neoadjuvant or adjuvant chemotherapy. Future clinical trials to test the efficacy of neoadjuvant or adjuvant chemotherapy and screen prognostic biomarkers involved in stage IIA CRC with elevated TLR are warranted. Third, recent studies have demonstrated the prognostic significance of other metabolic PET parameters, such as metabolic tumor volume (MTV) and total lesion glycolysis (TLG), in various types of cancer [50]. We did not evaluate these parameters due to a lack of software. Moreover, there have been reports that a low extracellular pH may be an important factor in inducing more aggressive cancer phenotypes, and highly pH-sensitive PET tracers have potential for use in the clinic [51]. We will further investigate the association of MTV, TLG, and intracellular pH with the prognosis of stage IIA CRC in future work.
Conclusion
In summary, our study indicated that elevated TLR from preoperative 18F–FDG-PET/CT predicted worse DFS in stage IIA CRC patients who underwent curative surgery alone. Patients with elevated TLR might benefit from neoadjuvant or adjuvant chemotherapy to prevent recurrence and should be monitored carefully for the detection of possible recurrence during the early stage of follow-up.
References
Holmes D. A disease of growth. Nature. 2015;521:S2–3. doi:10.1038/521S2a.
Lin HH, Chang YY, Lin JK, Jiang JK, Lin CC, Lan YT, et al. The role of adjuvant chemotherapy in stage II colorectal cancer patients. Int J Color Dis. 2014;29:1237–43. doi:10.1007/s00384-014-1943-6.
Wu X, Zhang J, He X, Wang C, Lian L, Liu H, et al. Postoperative adjuvant chemotherapy for stage II colorectal cancer: a systematic review of 12 randomized controlled trials. J Gastrointest Surg. 2012;16:646–55. doi:10.1007/s11605-011-1682-8.
Edge SB, Compton CC. The American joint committee on cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17:1471–4. doi:10.1245/s10434-010-0985-4.
Norgaard A, Dam C, Jakobsen A, Ploen J, Lindebjerg J, Rafaelsen SR. Selection of colon cancer patients for neoadjuvant chemotherapy by preoperative CT scan. Scand J Gastroenterol. 2014;49:202–8. doi:10.3109/00365521.2013.862294.
Kocarnik JM, Shiovitz S, Phipps AI. Molecular phenotypes of colorectal cancer and potential clinical applications. Gastroenterol Rep. 2015;3:269–76. doi:10.1093/gastro/gov046.
Chowdhury FU, Shah N, Scarsbrook AF, Bradley KM. [18F]FDG PET/CT imaging of colorectal cancer: a pictorial review. Postgrad Med J. 2010;86:174–82. doi:10.1136/pgmj.2009.079087.
Kim DH, Son SH, Kim CY, Hong CM, Oh JR, Song BI, et al. Prediction for recurrence using F-18 FDG PET/CT in pathologic N0 lung adenocarcinoma after curative surgery. Ann Surg Oncol. 2014;21:589–96. doi:10.1245/s10434-013-3270-5.
Song BI, Lee SW, Jeong SY, Chae YS, Lee WK, Ahn BC, et al. 18F-FDG uptake by metastatic axillary lymph nodes on pretreatment PET/CT as a prognostic factor for recurrence in patients with invasive ductal breast cancer. J Nucl Med. 2012;53:1337–44. doi:10.2967/jnumed.111.098640.
Muralidharan V, Kwok M, Lee ST, Lau L, Scott AM, Christophi C. Prognostic ability of 18F-FDG PET/CT in the assessment of colorectal liver metastases. J Nucl Med. 2012;53:1345–51. doi:10.2967/jnumed.112.102749.
Lee JE, Kim SW, Kim JS, Choi KY, Kang WK, Oh ST, et al. Prognostic value of 18-fluorodeoxyglucose positron emission tomography-computed tomography in resectable colorectal cancer. World J Gastroenterol. 2012;18:5072–7. doi:10.3748/wjg.v18.i36.5072.
Lee HJ, Ahn BC, Hong CM, Song BI, Kim HW, Kang S, et al. Preoperative risk stratification using (18)F-FDG PET/CT in women with endometrial cancer. Nuklearmedizin. 2011;50:204–13. doi:10.3413/nukmed-0375-10-12.
Kang S, Ahn BC, Hong CM, Song BI, Lee HJ, Jeong SY, et al. Can (18)F-FDG PET/CT predict recurrence in patients with cutaneous malignant melanoma? Nuklearmedizin. 2011;50:116–21. doi:10.3413/Nukmed-0356-10-09.
Takeda A, Yokosuka N, Ohashi T, Kunieda E, Fujii H, Aoki Y, et al. The maximum standardized uptake value (SUVmax) on FDG-PET is a strong predictor of local recurrence for localized non-small-cell lung cancer after stereotactic body radiotherapy (SBRT). Radiother Oncol. 2011;101:291–7. doi:10.1016/j.radonc.2011.08.008.
Lee YY, Choi CH, Kim CJ, Kang H, Kim TJ, Lee JW, et al. The prognostic significance of the SUVmax (maximum standardized uptake value for F-18 fluorodeoxyglucose) of the cervical tumor in PET imaging for early cervical cancer: preliminary results. Gynecol Oncol. 2009;115:65–8. doi:10.1016/j.ygyno.2009.06.022.
Ko KY, Liu CJ, Ko CL, Yen RF. Intratumoral heterogeneity of Pretreatment 18F-FDG PET images predict disease progression in patients with nasal type Extranodal natural killer/T-cell lymphoma. Clin Nucl Med. 2016;41:922–6. doi:10.1097/RLU.0000000000001375.
Fuertes S, Setoain X, Lopez-Guillermo A, Carrasco JL, Rodriguez S, Rovira J, et al. Interim FDG PET/CT as a prognostic factor in diffuse large B-cell lymphoma. Eur J Nucl Med Mol Imaging. 2013;40:496–504. doi:10.1007/s00259-012-2320-8.
Park J, Chang KJ, Seo YS, Byun BH, Choi JH, Moon H, et al. Tumor SUVmax normalized to liver uptake on (18)F-FDG PET/CT predicts the pathologic complete response after Neoadjuvant Chemoradiotherapy in locally advanced rectal cancer. Nucl Med Mol Imaging. 2014;48:295–302. doi:10.1007/s13139-014-0289-x.
Song MJ, Bae SH, Yoo Ie R, Park CH, Jang JW, Chun HJ, et al. Predictive value of (1)(8)F-fluorodeoxyglucose PET/CT for transarterial chemolipiodolization of hepatocellular carcinoma. World J Gastroenterol. 2012;18:3215–22. doi:10.3748/wjg.v18.i25.3215.
Lee JW, Paeng JC, Kang KW, Kwon HW, Suh KS, Chung JK, et al. Prediction of tumor recurrence by 18F-FDG PET in liver transplantation for hepatocellular carcinoma. J Nucl Med. 2009;50:682–7. doi:10.2967/jnumed.108.060574.
Nakajo M, Jinguji M, Nakabeppu Y, Nakajo M, Higashi R, Fukukura Y, et al. Texture analysis of 18F-FDG PET/CT to predict tumour response and prognosis of patients with esophageal cancer treated by chemoradiotherapy. Eur J Nucl Med Mol Imaging. 2017;44:206–14. doi:10.1007/s00259-016-3506-2.
Wang X, Peng G, Zhang X, Chen Z, Zhang B, Li Z. Correlation of (1)(8)F-FDG PET-CT maximum standard uptake value and T/N ratio with the prognosis of postoperative colorectal cancer. Zhonghua Wei Chang Wai Ke Za Zhi. 2015;18:232–7.
Riad R, Omar W, Kotb M, Hafez M, Sidhom I, Zamzam M, et al. Role of PET/CT in malignant pediatric lymphoma. Eur J Nucl Med Mol Imaging. 2010;37:319–29. doi:10.1007/s00259-009-1276-9.
Luan X, Huang Y, Gao S, Sun X, Wang S, Ma L, et al. 18F-alfatide PET/CT may predict short-term outcome of concurrent chemoradiotherapy in patients with advanced non-small cell lung cancer. Eur J Nucl Med Mol Imaging. 2016;43:2336–42. doi:10.1007/s00259-016-3505-3.
Lee Y, Yoo IR, Boo SH, Kim H, Park HL, Hyun OJ. The role of F-18 FDG PET/CT in Intrahepatic Cholangiocarcinoma. Nucl Med Mol Imaging. 2017;51:69–78. doi:10.1007/s13139-016-0440-y.
Leseur J, Roman-Jimenez G, Devillers A, Ospina-Arango JD, Williaume D, Castelli J, et al. Pre- and per-treatment 18F-FDG PET/CT parameters to predict recurrence and survival in cervical cancer. Radiother Oncol. 2016;120:512–8. doi:10.1016/j.radonc.2016.08.008.
Suzuki Y, Okabayashi K, Hasegawa H, Tsuruta M, Shigeta K, Murakami K, et al. Metabolic tumor volume and Total lesion Glycolysis in PET/CT correlate with the pathological findings of colorectal cancer and allow its accurate staging. Clin Nucl Med. 2016;41:761–5. doi:10.1097/RLU.0000000000001332.
Makis W, Kurzencwyg D, Hickeson M. 18F-FDG PET/CT superior to serum CEA in detection of colorectal cancer and its recurrence. Clin Imaging. 2013;37:1094–7. doi:10.1016/j.clinimag.2013.04.004.
Liberale G, Lecocq C, Garcia C, Muylle K, Covas A, Deleporte A, et al. Accuracy of FDG-PET/CT in colorectal peritoneal Carcinomatosis: potential tool for evaluation of chemotherapeutic response. Anticancer Res. 2017;37:929–34. doi:10.21873/anticanres.11401.
Murakami S, Saito H, Sakuma Y, Kondo T, Oshita F, Ito H, et al. Prognostic value of preoperative FDG-PET in stage IA lung adenocarcinoma. Eur J Radiol. 2012;81:1891–5. doi:10.1016/j.ejrad.2011.04.007.
Keyes JW Jr. SUV: standard uptake or silly useless value? J Nucl Med. 1995;36:1836–9.
Vanderhoek M, Perlman SB, Jeraj R. Impact of the definition of peak standardized uptake value on quantification of treatment response. J Nucl Med. 2012;53:4–11. doi:10.2967/jnumed.111.093443.
Boellaard R, Krak NC, Hoekstra OS, Lammertsma AA. Effects of noise, image resolution, and ROI definition on the accuracy of standard uptake values: a simulation study. J Nucl Med. 2004;45:1519–27.
Lee JW, Kim SK, Lee SM, Moon SH, Kim TS. Detection of hepatic metastases using dual-time-point FDG PET/CT scans in patients with colorectal cancer. Mol Imaging Biol. 2011;13:565–72. doi:10.1007/s11307-010-0394-x.
Gu J, Yamamoto H, Fukunaga H, Danno K, Takemasa I, Ikeda M, et al. Correlation of GLUT-1 overexpression, tumor size, and depth of invasion with 18F-2-fluoro-2-deoxy-D-glucose uptake by positron emission tomography in colorectal cancer. Dig Dis Sci. 2006;51:2198–205. doi:10.1007/s10620-006-9428-2.
Riedl CC, Akhurst T, Larson S, Stanziale SF, Tuorto S, Bhargava A, et al. 18F-FDG PET scanning correlates with tissue markers of poor prognosis and predicts mortality for patients after liver resection for colorectal metastases. J Nucl Med. 2007;48:771–5. doi:10.2967/jnumed.106.037291.
Wang LM, Kevans D, Mulcahy H, O’Sullivan J, Fennelly D, Hyland J, et al. Tumor budding is a strong and reproducible prognostic marker in T3N0 colorectal cancer. Am J Surg Pathol. 2009;33:134–41. doi:10.1097/PAS.0b013e318184cd55.
Tanaka M, Hashiguchi Y, Ueno H, Hase K, Mochizuki H. Tumor budding at the invasive margin can predict patients at high risk of recurrence after curative surgery for stage II, T3 colon cancer. Dis Colon Rectum. 2003;46:1054–9. doi:10.1097/01.DCR.0000074867.87213.D1.
Barresi V, Reggiani Bonetti L, Vitarelli E, Di Gregorio C, Ponz de Leon M, Barresi G. Immunohistochemical assessment of lymphovascular invasion in stage I colorectal carcinoma: prognostic relevance and correlation with nodal micrometastases. Am J Surg Pathol. 2012;36:66–72. doi:10.1097/PAS.0b013e31822d3008.
Benson AB 3rd, Schrag D, Somerfield MR, Cohen AM, Figueredo AT, Flynn PJ, et al. American Society of Clinical Oncology recommendations on adjuvant chemotherapy for stage II colon cancer. J Clin Oncol. 2004;22:3408–19. doi:10.1200/JCO.2004.05.063.
Kotaka M, Yoshino T, Oba K, Shinozaki K, Touyama T, Manaka D, et al. Initial safety report on the tolerability of modified FOLFOX6 as adjuvant therapy in patients with curatively resected stage II or III colon cancer (JFMC41-1001-C2: JOIN trial). Cancer Chemother Pharmacol. 2015;76:75–84. doi:10.1007/s00280-015-2757-0.
Meyerhardt JA. Adjuvant therapy for stage II and III colon cancer. Clin Adv Hematol Oncol. 2010;8:772–4.
Gramont A. Adjuvant therapy of stage II and III colon cancer. Semin Oncol. 2005;32:11–4. doi:10.1053/j.seminoncol.2005.06.004.
Burt BM, Humm JL, Kooby DA, Squire OD, Mastorides S, Larson SM, et al. Using positron emission tomography with [(18)F]FDG to predict tumor behavior in experimental colorectal cancer. Neoplasia. 2001;3:189–95. doi:10.1038/sj/neo/7900147.
Deng Y, Wang L, Tan S, Kim GP, Dou R, Chen D, et al. KRAS as a predictor of poor prognosis and benefit from postoperative FOLFOX chemotherapy in patients with stage II and III colorectal cancer. Mol Oncol. 2015;9:1341–7. doi:10.1016/j.molonc.2015.03.006.
Buvat I, Necib H, Garcia C, Wagner A, Vanderlinden B, Emonts P, et al. Lesion-based detection of early chemosensitivity using serial static FDG PET/CT in metastatic colorectal cancer. Eur J Nucl Med Mol Imaging. 2012;39:1628–34. doi:10.1007/s00259-012-2172-2.
Vriens D, de Geus-Oei LF, van der Graaf WT, Oyen WJ. Tailoring therapy in colorectal cancer by PET-CT. Q J Nucl Med Mol Imaging. 2009;53:224–44.
Banzo J, Ubieto MA, Giraldo P, Razola P, Prats E, Tardin L, et al. Resistance to first line chemotherapy treatment in a patient diagnosed of nodular lymphocyte-predominant Hodgkin’s lymphoma identified by 18F-FDG PET/CT: diagnostic and therapeutic implications. Rev Esp Med Nucl Imagen Mol. 2012;31:89–92. doi:10.1016/j.remn.2011.03.018.
Cashen AF, Dehdashti F, Luo J, Homb A, Siegel BA, Bartlett NL. 18F-FDG PET/CT for early response assessment in diffuse large B-cell lymphoma: poor predictive value of international harmonization project interpretation. J Nucl Med. 2011;52:386–92. doi:10.2967/jnumed.110.082586.
Ryu IS, Kim JS, Roh JL, Cho KJ, Choi SH, Nam SY, et al. Prognostic significance of preoperative metabolic tumour volume and total lesion glycolysis measured by (18)F-FDG PET/CT in squamous cell carcinoma of the oral cavity. Eur J Nucl Med Mol Imaging. 2014;41:452–61. doi:10.1007/s00259-013-2571-z.
Zhang X, Lin Y, Gillies RJ. Tumor pH and its measurement. J Nucl Med. 2010;51:1167–70. doi:10.2967/jnumed.109.068981.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Funding
This study was funded by the Science and Technology Planning Project of Guangdong Province, China (No. 2013B010404018), and the Research Fund for the Doctoral Program of Higher Education of China (RFDP) (No. 20130171120097).
Conflict of interest
We declare no conflicts of interest.
Ethical approval
All procedures in this study involving human participants were performed in accordance with the ethical standards of the Sixth Affiliated Hospital Research Committee of Sun Yat-sen University and with the 1964 Declaration of Helsinki and its later amendments.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Huang, J., Huang, L., Zhou, J. et al. Elevated tumor-to-liver uptake ratio (TLR) from 18F–FDG-PET/CT predicts poor prognosis in stage IIA colorectal cancer following curative resection. Eur J Nucl Med Mol Imaging 44, 1958–1968 (2017). https://doi.org/10.1007/s00259-017-3779-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-017-3779-0