
Abstract
Purpose
To analyze the prevalence of classic magnetic resonance imaging (MRI) findings of intramuscular peripheral nerve sheath tumors (PNSTs), including schwannoma, ancient schwannoma, and neurofibroma.
Method
Thirty pathologically confirmed benign intramuscular PNSTs (24 schwannomas, 3 ancient schwannomas, and 3 neurofibromas) were retrospectively reviewed. Classic MRI findings of PNSTs including split fat sign, fascicular sign, target sign, entering and exiting nerve, and thin hyperintense rim were assessed for each intramuscular PNST. Denervation change of the affected muscle was also assessed. In ancient schwannoma and neurofibroma, the signal intensity (SI) and enhancement pattern were analyzed.
Results
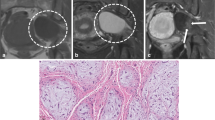
All intramuscular schwannomas revealed two more classic MRI findings. Eight of the 24 intramuscular schwannomas revealed affected muscle denervation change. All intramuscular ancient schwannomas showed only split fat sign. All intramuscular ancient schwannomas showed denervation change of the associated muscle. All intramuscular neurofibroma showed split fat sign and one case with target sign was detected. Ancient schwannomas were isointense SI on T1-weighted image (T1WI) and one case had hyperintense foci. They showed heterogeneously hyperintense SI on T2-weighted image (T2WI) with heterogeneous enhancement. Neurofibromas were isointense SI (2/3) and slight hyperintense SI (1/3) on T1WI and heterogeneously hyperintense SI on T2WI with heterogeneous enhancement. One ancient schwannoma showed conglomerated calcifications.
Conclusions
Intramuscular schwannomas were easily diagnosed based on MRI. In the case of intramuscular ancient schwannoma and neurofibroma with only split fat sign among the classic MRI findings, they might be distinguished from other intramuscular soft tissue tumors based on muscle denervation change or typical crescent split fat sign.






Similar content being viewed by others


References
Donner TR, Voorhies RM, Kline DG. Neural sheath tumors of major nerves. J Neurosurg. 1994;81:362–73.
Artico M, Cervoni L, Wierzbicki V, D’Andrea V, Nucci F. Benign neural sheath tumours of major nerves: characteristics in 119 surgical cases. Acta Neurochir. 1997;139:1108–16.
Salunke AA, Chen Y, Tan JH, et al. Intramuscular schwannoma: clinical and magnetic resonance imaging features. Singap Med J. 2015;56:555–7.
Kwon BC, Baek GH, Chung MS, Lee SH, Kim HS, Oh JH. Intramuscular neurilemoma. J Bone Joint Surg Br. 2003;85:723–5.
Murphey MD, Smith WS, Smith SE, Kransdorf MJ, Temple HT. From the archives of the AFIP. Imaging of musculoskeletal neurogenic tumors: radiologic-pathologic correlation. Radiographics. 1999;19:1253–80.
Abreu E, Aubert S, Wavreille G, Gheno R, Canella C, Cotten A. Peripheral tumor and tumor-like neurogenic lesions. Eur J Radiol. 2013;82:38–50.
Pilavaki M, Chourmouzi D, Kiziridou A, Skordalaki A, Zarampoukas T, Drevelengas A. Imaging of peripheral nerve sheath tumors with pathologic correlation: pictorial review. Eur J Radiol. 2004;52:229–39.
Chee DW, Peh WC, Shek TW. Pictorial essay: imaging of peripheral nerve sheath tumours. Can Assoc Radiol J. 2011;62:176–82.
Shimose S, Sugita T, Kubo T, et al. Major-nerve schwannomas versus intramuscular schwannomas. Acta Radiol. 2007;48:672–7.
Chennakeshaviah G, Ravishankar S, Maggad R, Manjunath GV. Solitary giant intramuscular myxoid neurofibroma resulting in an above elbow amputation. Case Rep Pathol. 2012;2012:353215.
Lee YS, Kim JO, Park SE. Ancient schwannoma of the thigh mimicking a malignant tumour: a report of two cases, with emphasis on MRI findings. Br J Radiol. 2010;83:e154–7.
Sung J, Kim JY. Fatty rind of intramuscular soft-tissue tumors of the extremity: is it different from the split fat sign? Skelet Radiol. 2017;46:665–73.
Jee WH, Oh SN, McCauley T, et al. Extraaxial neurofibromas versus neurilemmomas: discrimination with MRI. AJR Am J Roentgenol. 2004;183:629–33.
Patel NB, Stacy GS. Musculoskeletal manifestations of neurofibromatosis type 1. AJR Am J Roentgenol. 2012;199:W99–106.
Soldatos T, Fisher S, Karri S, Ramzi A, Sharma R, Chhabra A. Advanced MR imaging of peripheral nerve sheath tumors including diffusion imaging. Semin Musculoskelet Radiol. 2015;19:179–90.
Beaman FD, Kransdorf MJ, Menke DM. Schwannoma: radiologic-pathologic correlation. Radiographics. 2004;24:1477–81.
Lin J, Martel W. Cross-sectional imaging of peripheral nerve sheath tumors: characteristic signs on CT, MR imaging, and sonography. AJR Am J Roentgenol. 2001;176:75–82.
Stull MA, Moser RP Jr, Kransdorf MJ, Bogumill GP, Nelson MC. Magnetic resonance appearance of peripheral nerve sheath tumors. Skelet Radiol. 1991;20:9–14.
Isobe K, Shimizu T, Akahane T, Kato H. Imaging of ancient schwannoma. AJR Am J Roentgenol. 2004;183:331–6.
Nakashima T, Tsurumaru D, Nishimuta Y, Miyasaka M, Nishie A, Honda H. A case of pelvic schwannoma presenting prominent eggshell-like calcification. Case Rep Radiol. 2013;2013:825078.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Part of the population of this study (n = 18) originates from a previous study with different aim to determine the MRI findings for differentiating Intramuscular PNSTs [12]. No data have been fabricated or manipulated. No data, text, or theories by others are presented as if they were the author’s own. Proper acknowledgements to other works have been given, quotation marks were used for verbatim copying of material, and permissions were secured for material that is copyrighted. Authors whose names appear on the submission have contributed sufficiently to the scientific work and therefore share collective responsibility and accountability for the results. Authors are prepared to send documentation or data in order to verify the validity of their results.
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval and informed consent
The institutional review board approved this retrospective study and the informed consent was waived.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This manuscript has been submitted to Skeletal Radiology alone at this time and has not previously been published.
Rights and permissions
About this article

Cite this article
Lee, S.K., Kim, JY., Lee, YS. et al. Intramuscular peripheral nerve sheath tumors: schwannoma, ancient schwannoma, and neurofibroma. Skeletal Radiol 49, 967–975 (2020). https://doi.org/10.1007/s00256-020-03371-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-020-03371-6