
Abstract
Purpose
The objectives of the study were to compare MR imaging at 1.5 and 3.0 T in the same patients concerning image quality and visualization of cartilage pathology and to assess diagnostic performance using arthroscopy as a standard of reference.
Materials and methods
Twenty-six patients were identified retrospectively as having comparative 1.5 and 3.0 T MR studies of the knee within an average of 102 days. Standard protocols included T1-weighted and fat-saturated intermediate-weighted fast spin-echo sequences in three planes; sequence parameters had been adjusted to account for differences in relaxation at 3.0 T. Arthroscopy was performed in 19 patients. Four radiologists reviewed each study independently, scored image quality, and analyzed pathological findings. Sensitivities, specificities, and accuracies in diagnosing cartilage lesions were calculated in the 19 patients with arthroscopy, and differences between 1.5 and 3.0 T exams were compared using paired Student’s t tests with a significance threshold of p < 0.05.
Results
Each radiologist scored the 3.0 T studies higher than those obtained at 1.5 T in visualizing anatomical structures and abnormalities (p < 0.05). Using arthroscopy as a standard of reference, diagnosis of cartilage abnormalities was improved at 3.0 T with higher sensitivity (75.7% versus 70.6%), accuracy (88.2% versus 86.4%), and correct grading of cartilage lesions (51.3% versus 42.9%). Diagnostic confidence scores were higher at 3.0 than 1.5 T (p < 0.05) and signal-to-noise ratio at 3.0 T was approximately twofold higher than at 1.5 T.
Conclusion
MRI at 3.0 T improved visualization of anatomical structures and improved diagnostic confidence compared to 1.5 T. This resulted in significantly better sensitivity and grading of cartilage lesions at the knee.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Although 1.5 T MRI of the knee is standard in clinical practice and performs well in assessing internal joint derangement, limitations have to be considered. In particular, assessing abnormalities of the hyaline articular cartilage and lateral meniscus may be challenging [1–3]. The current literature suggests that imaging at 3.0 T MRI offers clinical benefits compared to 1.5 T [4, 5]. The stronger field strength increases signal-to-noise ratio (SNR), potentially allowing thinner sections and higher in plane spatial resolutions resulting in better visualization of anatomical and pathological structures [6].
A number of in vitro studies have shown improved visualization of cartilage and ligament pathology at the knee and ankle using 3.0 T in comparison with 1.5 T MRI [7, 8]. Studies have also demonstrated 3.0 T MRI to have high sensitivity and specificity in diagnosing knee meniscus, cartilage, and ligamentous pathology when compared with subsequent arthroscopy [9–12]. A limitation of these studies, however, was that direct comparison with imaging at 1.5 T in the same subjects was not obtained and that previously published data from the literature obtained at 1.5 T were used as a reference in some of these studies. To the best of our knowledge, no studies have been performed directly comparing MR imaging at the knee at 1.5 and 3.0 T obtained in the same patients and correlating these findings with arthroscopy.
The goals of our study therefore were (a) to compare standard clinical MRI studies obtained at 1.5 and 3.0 T in the same patients concerning visualization of cartilage, menisci, and ligaments and (b) to assess these 1.5 and 3.0 T studies concerning abnormalities of cartilage using arthroscopy as a standard of reference.
Materials and methods
Patients
This Health Insurance Portability and Accountability Act-compliant (HIPAA) study had institutional review board approval. A retrospective search examining patient records from July 27, 2004 through July 25, 2008 was conducted. Twenty-six patients (eight males and 18 females) were identified who had both a comparative 3.0 and 1.5 T MRI scan of the knee. Comparative studies were completed within an average time interval of 101.66 ± 79.09 days. Nineteen of the 26 patients also had a knee arthroscopy of the same knee that were performed at our department of orthopedic surgery within an average time interval of 56 ± 40.9 days to the most recent MR study. The average age of the patients at the time of the first examination was 38.5 ± 11.3 years. Clinical indications for MRI of the knee included knee pain in 17 patients, pain and/or locking with suspected meniscal injury in five patients, and instability with suspected ligament tears in four patients. The main reasons for repeated imaging studies were (a) to obtain a 3 T study to better visualize cartilage lesions and (b) to provide a follow-up MRI after arthroscopy if no cartilage repair was performed.
MR imaging
MR studies were obtained using 1.5 and 3.0 T whole body scanners (Signa, GE Healthcare, Waukesha, WI, USA). Standard transmit/receive knee coils were used; most of the studies were obtained with quadrature knee coils (GE, Healthcare and MR Solutions, Brookfield, WI, USA; 18 at 3 T and 16 at 1.5 T) and more recently eight-channel phased-array knee coils (Invivo, Orlando, FL, USA; eight at 3 T and ten studies at 1.5 T) were used. Given that approximately the same number of the studies at each field strength was obtained with similar coils, no bias is expected due to coil design. The MR protocol consisted of a coronal T1-weighted and fat-saturated (fs) intermediate-weighted (iw) fast spin-echo (FSE) sequences, sagittal iw and fs iw FSE sequences, and axial fs iw FSE sequences. Detailed sequence parameters are listed in Table 1; sequence parameters had been adjusted to account for differences in relaxation at 3.0 T. Also, we reduced the number of excitations (NEX) from 3 to 2 and increased the echo train length at 3.0 T to maintain acquisition time. With the higher SNR at 3.0 T, it was also possible to increase the matrix size from 224 × 224 to 320 × 256 pixels.
MR image analysis
Three board-certified radiologists and a radiology resident with expertise in musculoskeletal MRI ranging from 3 to 23 years evaluated all images (CS, JZ, LS, TML) on PACS workstations (Agfa, Ridgefield Park, NJ, USA). At the time of analysis, the radiologists were blinded to the clinical history, previous reports, field strength, and sequence parameters. During the reading sessions, ambient light was kept at a minimum, and no time constraints were used. No more than 25 studies were reviewed at one time. Time between reading sessions was at least 96 h to prevent learning bias. Studies obtained at 1.5 and 3.0 T were presented to the radiologist in random order.
The radiologists reviewed all sequences of one MR study and were asked to grade image quality, using the following criteria: edge sharpness, amount of blurring, artifacts, contrast between fluid and cartilage, contrast between fluid and soft tissue, delineation of small ligamentous structures, and amount of noise. A four-level scale was used, in which four indicated optimal image quality and one substantially reduced image quality limiting diagnostic evaluation.
In addition, presence and absence of pathology were graded focusing on cartilage, meniscal, ligamentous, tendon, and bone marrow abnormalities. Cartilage lesions were graded according to Recht et al. based on a modified Noyes classification [13]. Four grades were differentiated: grade 1 was defined as signal heterogeneity and/or swelling, grade 2 as a less than 50% defect, grade 3 as a more than 50% defect, and grade 4 as a full thickness defect. If a lesion was identified, radiologists were asked to assign a confidence score indicating whether they felt the lesion was a definite [3], a probable [2], or a questionable lesion [1]. For meniscus pathology, radiologists were asked to identify lesions in the anterior and posterior horn as well as the body of both the medial and lateral meniscus. Abnormalities identified were graded as intra-substance signal abnormality, non-displaced vertical or horizontal tear, complex tear without deformity, and complex tears with deformity of the meniscus. A confidence score was also assigned, analogous to this used for the cartilage lesions.
The ligaments and tendons assessed included anterior cruciate ligament, posterior cruciate ligament, medial collateral ligament, lateral collateral ligament, popliteus, and patellar tendon. Abnormalities were assessed as grade 1 (mild), grade 2 (signal abnormality of the tendon or ligament suggesting partial tear), and grade 3 (complete tear) strain or sprain. A diagnostic confidence score was assigned as outlined previously for cartilage and menisci.
SNR measurements
Quantitative analysis was also performed calculating effective signal-to-noise-ratios (SNRE) for the sagittal fs iw FSE sequences with \( {\text{SNR}}_{\text{E}} =\frac{{\frac{{{\text{SI}}_{\text{Tissue}} }}{{{\text{SD}}_{\text{Background}} }}}}{{\sqrt {\text{scantime}} }} \), where SITissue was the signal intensity of cartilage, and SDBackground was the standard deviation of the background. Regions of interest were placed in the background and the trochlear cartilage.
Standard of reference
The standard of reference for the MR abnormalities was based on the arthroscopic findings in 19 subjects, which were reviewed with all available MR imaging and clinical findings. The arthroscopies were performed by one of three experienced orthopedic surgeons at UCSF Medical Center who specialize in sports medicine. Arthroscopies were performed after the orthopedic surgeons had reviewed the MRI studies. All articular surfaces were examined, and their lesions were graded using the Noyes scale, analogous to the grading system used for the cartilage lesions (grade 1 = softening, grade 2 = less than 50% defect, grade 3 = more than 50% defect, grade 4 = full thickness cartilage defect). The location and the type of meniscal defects were noted analogous to the classification used for the MRI. Ligament and tendon lesions were examined and scored as for the MRI studies.
Statistical analysis
A signed rank test, with a significance threshold of p < 0.05, was used to compare the differences in image quality measurements of all evaluated anatomical structures and confidence scores between 3.0 and 1.5 T. McNemar's tests were used to assess the differences in direct comparison of image quality. SNR differences of cartilage signal between 3.0 and 1.5 T were assessed using paired Student's t tests with a significance threshold of p < 0.05. Sensitivities, specificities, and accuracies with 95% confidence intervals were calculated to estimate the diagnostic performance for cartilage and meniscal lesions using the established standard of reference. All of the statistical computations were processed using JMP 7 (SAS Institute, Cary, NC, USA).
Results
Image quality
Each of the four radiologists independently rated images obtained at 3.0 better than at 1.5 T. Both visualization of anatomy and abnormalities of the knee obtained superior grades at 3.0 T compared to 1.5 T (p < 0.05). The average image quality at 3.0 T was 3.65 ± 0.54, while 2.74 ± 0.73 was calculated for the 1.5 T studies (Table 2). In 80.7% of cases, the four radiologists found the image quality of the 3.0 T studies to be higher than that of the 1.5 T studies (p < 0.01). Results for all radiologists combined and each radiologist individually are shown in Table 3.
SNR measurements
As expected, higher effective SNR values were found at 3.0 than at 1.5 T. The SNR for the 3.0 T scan was approximately twofold higher at 3.0 T versus 1.5 T measured in the sagittal fs iw FSE sequences. The SNR values for 3.0 and 1.5 T were 2.63 ± 0.83 and 1.24 ± 0.67, respectively.
Diagnostic performance
Based on arthroscopy as a standard of reference, diagnostic performance in terms of accuracy, sensitivity, and specificity was calculated for cartilage lesions (Table 4). Thirty-nine cartilage lesions were identified. Thirteen were full thickness lesions (grade 4). Fourteen were graded as greater than 50% (grade 3) and seven as less than 50% (grade 2). Five lesions were graded as abnormal signal/swelling resp. softening (grade 1).
The diagnostic performance at 3.0 T was superior to that at 1.5 T for sensitivity and overall accuracy of cartilage lesions (p < 0.05). Specificity for cartilage lesions was not significantly different at 3.0 and 1.5 T (p < 0.05). Differences between the number of false-positive cartilage lesions found at 3.0 and 1.5 T were not significant (p > 0.05). The number of false-negative findings at 3.0 T was significantly lower than at 1.5 T (p < 0.05).
The number and percentage of correctly identified and scored cartilage lesions was significantly higher at 3.0 T than at 1.5 T (p < 0.05) for all radiologists combined. Results were superior at 3.0 T both for exact grading and grading within ±1 score. Note that when using arthroscopy as a standard of reference, correct grading at 3.0 T was achieved in only 51.3% of the lesions, while 42.9% of the lesions were correctly graded at 1.5 T. When including lesions that were scored within one grade, the diagnostic performance improved for both 3.0 and 1.5 T MRI, with 64.7% correct grading at 3.0 T and 58.3% at 1.5 T. Results are demonstrated in Table 5 for subjects with arthroscopy as a standard of reference. One radiologist correctly graded one additional lesion at 1.5 T compared to 3.0 T; however, this radiologist correctly scored one additional lesion within ± one grade at 3.0 T compared to 1.5 T. Figures 1, 2, 3, and 4 show representative images with cartilage lesions obtained at 3.0 and 1.5 T.

A 35-year-old male patient reported locking and painful left knee. a The 1.5 T study (sagittal fs iw FSE sequence, TR 3,200 ms, TE 46 ms) with questionable signal change at the patellar cartilage (arrow). b The corresponding sequence obtained at 3.0 T (TR 4,300 ms, TE 51 ms; arrow), in which the radiologists correctly identified a definite greater than 50% patellar cartilage lesion. Arthroscopy served as a standard of reference

A 37-year-old male patient presented with swelling and contracture of the left knee. While no definite lesion was visualized at 1.5 T (a; axial fs iw FSE sequence, TR 3,700 ms, TE 46 ms), a patellar cartilage lesion (arrow) was correctly demonstrated and graded (>50%) on the corresponding FSE sequence (TR 4,300 ms, TE 51 ms) at 3.0 T (b; arrow), as verified by arthroscopy

A 36-year-old male patient with a clinical history of left knee pain and suspected osteochondritis dissecans. At 1.5 T (a; sagittal fs iw FSE sequence, TR 3,200 ms, TE 46 ms) an area of high signal is shown along the subchondral bone underneath the cartilage suggesting delamination (arrow) without a focal cartilage defect. The 3.0 T study (a; TR 4,300 ms, TE 51 ms) clearly shows a full thickness cartilage defect along with delamination (arrow). Findings were confirmed by arthroscopy after both imaging studies were obtained

A 28-year-old woman reported right knee pain with suspected meniscal tear. The coronal fs iw FSE sequence (TR 3,200 ms, TE 46 ms) at 1.5 T (a) shows a probable less than 50% lesion with additional cartilage thinning, while the corresponding 3.0 T sequence (TR 4,300 ms, TE 51 ms) demonstrates a definite less than 50% lesion (arrow)
False-positive and false-negative findings were studied in more detail, specifically analyzing location and grade of these lesions in relation to field strength. Most of the false-negative lesions were found at the lateral tibial plateau followed by the medial tibial plateau. No false negatives were found at the medial femoral condyle. The largest difference in false-negative findings between 3.0 and 1.5 T was found at the patella with more lesions diagnosed at 3.0 T. Most of the false negatives were grade 1 lesions followed by grade 3 lesions, which may be explained by the fact that the number of grade 2 lesions was small. Overall less false-negative diagnoses were made at 3.0 T. Most of the false-positive lesions were diagnosed at the patella followed by the lateral femoral condyle. The smallest number of false positives was found at the trochlea. Most of the false positives were grade 1 and 2 lesions. Only one false-positive grade 4 lesion was diagnosed. There were no differences in location and grade between false-positive lesions diagnosed at 1.5 and 3.0 T; in fact, no difference in false positives between 1.5 and 3.0 T was found.
Eleven meniscal lesions were detected in the 19 patients using arthroscopy as a standard of reference. Five menisci showed complex tears with deformity (grade 4). There were two menisci with non-displaced vertical tears: one meniscus with a horizontal tear and one with a meniscal root-tear (grade 2). Two patients had complex tears without deformity (grade 3). At 3.0 T, improved accuracy for meniscal lesions was found for two radiologists, identical accuracy for one radiologist, and decreased accuracy for one radiologist. The number and percentage of correctly identified and scored meniscal lesions was mildly higher at 3.0 T than at 1.5 T for all radiologists combined, but differences were not significant (p > 0.05). Figure 5 shows a meniscal lesion that was better visualized at 3.0 T. Given that the number of meniscal lesions in the study sample was relatively small and does not provide statistically meaningful data, no additional analyses were listed.

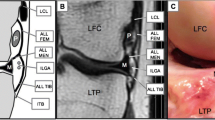
A 52-year-old female patient presents with left knee pain and a history of early osteoarthritis. Comparative MRI studies and arthroscopy were obtained. A horizontal tear of the posterior horn of the medial meniscus is demonstrated at 3.0 T (confidence score 3; b; TR 4,300 ms, TE 51 ms; arrow), which is not well shown at 1.5 T (confidence score 1–2; TR 3,200 ms, TE 46 ms; arrow)
Confidence scores
The confidence scores of each radiologist and all radiologists combined were significantly higher at 3.0 T than at 1.5 T. Results for the individual radiologists are demonstrated in Table 6. Figures 1, 2, 3, and 4 show representative MR images obtained at 3.0 and 1.5 T for cartilage lesions, while in Fig. 5, differences in visualization of a meniscus lesion at 3.0 and 1.5 T are demonstrated.
A higher number of correctly identified cartilage lesions were graded as definite lesions at 3.0 T versus 1.5 T (p < 0.05) using arthroscopy as a standard of reference (Table 6). However, an increased number of false-positive lesions were also graded as definite lesions, while they were scored as questionable or probable lesions at 1.5 T. Meniscal abnormalities also demonstrated higher average diagnostic confidence scores at 3.0 T than at 1.5 T (p < 0.05). Only four ligament and tendon lesions were identified using arthroscopy as a standard of reference. Sensitivities, specificities, and accuracies were therefore not calculated. Ligament and tendon abnormalities showed a higher level of diagnostic confidence at 3.0 T versus 1.5 T (2.65 ± 0.49 versus 2.15 ± 0.59, p < 0.05, respectively). A total of 12 bone marrow lesions were identified and graded by all radiologists on both 1.5 and 3.0 T MR studies. Five bone marrow infarcts, three subchondral fractures, and four cases of post-traumatic bone marrow edema pattern were identified with the highest degree of confidence. Bone marrow abnormalities did not show significant differences in confidence scores between 3.0 and 1.5 T (both 3.0 ± 0.0 for bone marrow, p > 0.05).
Discussion
The results of this study show modest, yet significantly increased accuracies and sensitivities in diagnosing cartilage abnormalities at 3.0 T compared to 1.5 T at the knee. Specificity for cartilage lesions, however, did not improve for 3.0 T. Also, there was a 10% increase in correct grading of cartilage lesions at 3.0 T compared to 1.5 T. Overall image quality and diagnostic confidence were graded consistently higher at 3.0 T than at 1.5 T for each individual radiologist.
Though a number of in vitro studies were performed comparing visualization of cartilage, ligaments, and menisci at 1.5 and 3.0 T [7, 8, 14–16], there is a paucity of clinical studies in particular those comparing 1.5 and 3.0 T studies in the same subjects. Our results are consistent with previous in vitro studies demonstrating an increase in sensitivity and diagnostic performance observed at 3.0 T for cartilage lesion detection. Masi et al. [8] were among the first to demonstrate improved diagnostic performance of 3.0 T versus 1.5 T MRI in cartilage lesions. In a porcine model, artificial cartilage lesions were created, and using intermediate-weighted fast spin-echo and spoiled gradient-echo sequences, these investigators were able to show improved accuracy of cartilage lesion detection. Similar to our study, they were also able to demonstrate improved performance in grading cartilage lesions. Link et al. [16] compared different sequences in assessing cartilage abnormalities in vitro and concluded that while high-resolution intermediate-weighted fast spin-echo sequences showed substantial benefits in detecting cartilage lesions, standard clinical type fast spin-echo sequences did not demonstrate a major improvement in diagnostic performance. This may in part explain why only relatively minor improvement in sensitivity and accuracy in cartilage lesions were found in our study. Those investigators concluded that only thin section high-resolution sequences would exploit the full potential of 3.0 T imaging concerning cartilage lesion evaluation.
Kijowski et al. [9, 17] recently reported results from a study analyzing 200 consecutive patients undergoing MRI of the knee using identical pulse sequences on either a 1.5 T (n = 100) or 3.0 T (n = 100) scanner who had subsequent arthroscopic knee surgery. These investigators found that 3.0 T MRI had higher specificity and accuracy but not higher sensitivity for detecting cartilage lesions at 3 T than at 1.5 T. Similar to our study, they also found MRI to be more accurate at grading articular surfaces at 3.0 T. These investigators, however, did not study the same patients at 1.5 and 3.0 T but two different patient populations, though their patient numbers in each group were high (n = 100).
There has been discussion about the best-suited sequence for cartilage imaging; gradient-echo sequences (FLASH, fast low-angle shot, and SPGR, spoiled gradient echo) and intermediate- and T2-weighted FSE sequences with and without fat saturation have been used previously [3, 18, 19]. Currently, however, intermediate-weighted FSE sequences are the preferred sequences in a clinical setting and experience with these sequences encompasses multiple studies; sensitivities of 63–100% have been described using arthroscopy as a standard of reference [20–22], which is consistent with the results found in our study. Concern may be raised by the fact that results at 3.0 T in diagnosing cartilage lesions are still relatively low. This, however, may be explained by the fact that imaging studies were obtained over a period of several years, and most of the imaging studies were performed with a quadrature knee coil. Also, we used standard clinical protocols. High-resolution imaging sequences obtained with thinner slice thickness and multi-channel phased-array coils would have probably improved the results. However, the goal of our study was to analyze the effect of 3 T imaging on standard knee imaging, not using dedicated research protocols. The relatively low results for correct grading of cartilage lesions found in our study on the other hand are expected, and similar results have been previously reported at 3.0 T [8, 16].
It should be noted that using arthroscopy as a standard of reference has raised concerns [23]. Differentiating between cartilage lesions that are less than or greater than 50% may be challenging with arthroscopy as the bone surface is not exposed. The same applies for meniscal lesions, where radiologists may diagnose lesions in the red zone of the meniscus, which could not be verified because of the difficulty examining this area with arthroscopy; surgical blind spots, including the posterior meniscocapsular junction [24], and even incomplete arthroscopy may have skewed our false-positive numbers [1, 25].
In addition to optimized sequences, the benefits of 3.0 T imaging also heavily depend on suitable coils, which was a limitation in the early phase of 3.0 T MRI. In an in vivo study, Lutterbey et al. [26] compared the diagnostic performance of knee MRI performed with the body coil at 3.0 T and a dedicated knee coil at 1.5 T. These investigators found a significant decrease in image quality at 3.0 T with a visible and measurable signal loss, but stated that nearly all clinically important information could be obtained.
While most of the previous studies comparing 1.5 and 3.0 T imaging were performed at the knee, two previous studies focused on imaging of the ankle, comparing visualization of cartilage and ligament lesions at 1.5 and 3.0 T in human cadaver ankles [7, 14, 26]. Bauer et al. [7] found that compared with 1.5 T, 3.0 T MRI of the ankle joint improved diagnostic performance in assessing cartilage significantly, and there was a higher sensitivity for assessing ligamentous pathology. This was one of the first studies indicating that 3.0 T MRI may also improve visualization of ligamentous abnormalities. While in our study diagnostic confidence in assessing ligamentous and tendon lesions was also higher at 3.0 T than at 1.5 T, the number of lesions was not high enough to provide statistically meaningful data concerning diagnostic performance.
To the best of our knowledge, comparative studies assessing meniscal lesions at 1.5 and 3.0 T have not yet been performed. Schoth et al. compared visualization of anatomic structures at the knee and found superior subjective visualization at 3.0 T versus 1.5 T for the meniscus and ligaments; however, no dedicated evaluation of meniscal lesions with arthroscopic correlation was available [27]. Magee et al. and Ramnath et al. [11, 12] used 3 T MRI to study meniscal abnormalities and found promising results. Unfortunately, a direct comparison with imaging at 1.5 T was not available, and results were compared to those previously published in the literature at 1.5 T.
The greatest limitation of our study was our limited patient population, of which only 19 patients had arthroscopy as a standard of reference. An additional limitation is the use of standard protocols, which did not include high-resolution sequences. However, the goal of this study was to assess the performance of 3.0 T versus 1.5 T MRI in a clinical setting without using dedicated research protocols. Also, we acknowledge the differences in imaging performance between the readers; however, we aimed at having readers with different levels of training read the images and assess their performance in relation to field strength. The higher spatial resolution of the imaging sequences at 3.0 T compared to 1.5 T could have also contributed to the results; however, acquisition time was kept in the same range by reducing NEX and increasing ETL.
In conclusion, our study shows that 3.0 T MRI was superior for detecting and grading cartilage lesions compared to 1.5 T. Though a higher diagnostic confidence was found at 3.0 T, the false-positive rate was not decreased. Overall image quality at 3.0 T was rated superior to 1.5 T consistently by all four radiologists.
References
De Smet AA, Mukherjee R. Clinical, MRI, and arthroscopic findings associated with failure to diagnose a lateral meniscal tear on knee MRI. AJR Am J Roentgenol. 2008; 190: 22–26.
Huysse WC, Verstraete KL. Health technology assessment of magnetic resonance imaging of the knee. Eur J Radiol. 2008; 65: 190–193.
Link TM, Stahl R, Woertler K. Cartilage imaging: motivation, techniques, current and future significance. Eur Radiol. 2007; 17: 1135–1146.
Craig JG, Go L, Blechinger J, et al. Three-tesla imaging of the knee: initial experience. Skeletal Radiol. 2005; 34: 453–461.
Shapiro MD, Magee T, Williams D, Ramnath R, Ross JS. The time for 3 T clinical imaging is now. AJNR Am J Neuroradiol. 2004; 25: 1628–1629.
Ramnath RR. 3 T MR imaging of the musculoskeletal system (Part I): considerations, coils, and challenges. Magn Reson Imaging Clin N Am. 2006; 14: 27–40.
Bauer JS, Barr C, Henning TD, et al. Magnetic resonance imaging of the ankle at 3.0 Tesla and 1.5 Tesla in human cadaver specimens with artificially created lesions of cartilage and ligaments. Invest Radiol. 2008; 43: 604–611.
Masi JN, Sell CA, Phan C, et al. Cartilage MR imaging at 3.0 versus that at 1.5 T: preliminary results in a porcine model. Radiology. 2005; 236: 140–150.
Kijowski R, Blankenbaker DG, Davis KW, Shinki K, Kaplan LD, De Smet AA. Comparison of 1.5- and 3.0-T MR imaging for evaluating the articular cartilage of the knee joint. Radiology. 2009; 250: 839–848.
Magee T. Three-tesla MR imaging of the knee. Magn Reson Imaging Clin N Am. 2007; 15: 125–132.
Magee T, Williams D. 3.0-T MRI of meniscal tears. AJR Am J Roentgenol. 2006; 187: 371–375.
Ramnath RR, Magee T, Wasudev N, Murrah R. Accuracy of 3-T MRI using fast spin-echo technique to detect meniscal tears of the knee. AJR Am J Roentgenol. 2006; 187: 221–225.
Recht MP, Piraino DW, Paletta GA, Schils JP, Belhobek GH. Accuracy of fat-suppressed three-dimensional spoiled gradient-echo FLASH MR imaging in the detection of patellofemoral articular cartilage abnormalities. Radiology. 1996; 198: 209–212.
Barr C, Bauer JS, Malfair D, et al. MR imaging of the ankle at 3 Tesla and 1.5 Tesla: protocol optimization and application to cartilage, ligament and tendon pathology in cadaver specimens. Eur Radiol. 2007; 17: 1518–1528.
Fischbach F, Bruhn H, Unterhauser F, et al. Magnetic resonance imaging of hyaline cartilage defects at 1.5 T and 3.0 T: comparison of medium T2-weighted fast spin echo, T1-weighted two-dimensional and three-dimensional gradient echo pulse sequences. Acta Radiol. 2005; 46: 67–73.
Link TM, Sell CA, Masi JN, et al. 3.0 vs 1.5 MRI in the detection of focal cartilage pathology–ROC analysis in an experimental model. Osteoarthritis Cartilage. 2006; 14: 63–70.
Kijowski R, Blankenbaker D, Davis K, Shinki K, Kaplan L, De Smet AA. Comparison of 1.5 T and 3 T magnetic resonance imaging systems for evaluating the articular cartilage of the knee joint. In: RSNA. Chicago, 2007; VS21-14.
Gold GE, McCauley TR, Gray ML, Disler DG. What's new in cartilage? Radiographics. 2003; 23: 1227–1242.
Potter HG, Foo LF. Magnetic resonance imaging of articular cartilage: trauma, degeneration, and repair. Am J Sports Med. 2006; 34: 661–677.
Duc SR, Pfirrmann CW, Schmid MR, et al. Articular cartilage defects detected with 3D water-excitation true FISP: prospective comparison with sequences commonly used for knee imaging. Radiology. 2007; 245: 216–223.
Potter HG, Linklater JM, Allen AA, Hannafin JA, Haas SB. Magnetic resonance imaging of articular cartilage in the knee. An evaluation with use of fast-spin-echo imaging. J Bone Joint Surg Am. 1998; 80: 1276–1284.
Yoshioka H, Stevens K, Hargreaves BA, et al. Magnetic resonance imaging of articular cartilage of the knee: comparison between fat-suppressed three-dimensional SPGR imaging, fat-suppressed FSE imaging, and fat-suppressed three-dimensional DEFT imaging, and correlation with arthroscopy. J Magn Reson Imaging. 2004; 20: 857–864.
Quinn SF, Brown TF. Meniscal tears diagnosed with MR imaging versus arthroscopy: how reliable a standard is arthroscopy? Radiology. 1991; 181: 843–847.
Morin WD, Steadman JR. Arthroscopic assessment of the posterior compartments of the knee via the intercondylar notch: the arthroscopist's field of view. Arthroscopy. 1993; 9: 284–290.
Justice WW, Quinn SF. Error patterns in the MR imaging evaluation of menisci of the knee. Radiology. 1995; 196: 617–621.
Lutterbey G, Behrends K, Falkenhausen MV, et al. Is the body-coil at 3 Tesla feasible for the MRI evaluation of the painful knee? A comparative study. Eur Radiol. 2007; 17: 503–508.
Schoth F, Kraemer N, Niendorf T, Hohl C, Gunther RW, Krombach GA. Comparison of image quality in magnetic resonance imaging of the knee at 1.5 and 3.0 Tesla using 32-channel receiver coils. Eur Radiol. 2008; 18: 2258–2264.
Acknowledgment
We acknowledge Christopher Jovais's assistance in identifying patients examined at 1.5 and 3.0 T.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Wong, S., Steinbach, L., Zhao, J. et al. Comparative study of imaging at 3.0 T versus 1.5 T of the knee. Skeletal Radiol 38, 761–769 (2009). https://doi.org/10.1007/s00256-009-0683-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-009-0683-0