
Abstract
Background
Fireworks are often used to celebrate holidays and events. With novel designs and availability, there is potential for blast and burn injuries that can impact livelihood and function. This study aims to describe and analyse firework-related burns in adults across New South Wales and the Australian Capital Territory.
Methods
A retrospective statewide review was performed from January 2010 to December 2020 at the adult burns units. All firework-related burn injuries older than 18 years that attended or were referred to the burns unit were included.
Results
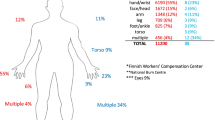
There were 203 patients with a firework-related burn injury. The male to female ratio was 4:1 with an average age of 32.2 years. Men were 5.2 years younger than women (31.2 vs 36.4, p = 0.010). Men were more likely to have firework-related injuries on non-holidays, whereas women were more likely on holidays (p = 0.050). Men were more likely to operate fireworks after consuming alcohol resulting in burns than women (34.4% vs 12.5%, p = 0.007). Sparklers were more common amongst women, whereas fireworks had higher proportions amongst men (p = 0.009). The most common site of injury was the hands. The most frequent type of injury was a mid-dermal burn (61.6%), followed by superficial (25.2%), and full thickness (13.2%) respectively. The operative rate was 17.7% with a mean total length of stay of 2.2 days (range: 1–12).
Conclusions
Firework-related burns have distinct patterns of use and injuries amongst men and women. Alongside legislation, awareness of the potential hazards for shopgood fireworks such as sparklers is critical for future prevention campaigns.
Level of evidence: Level III, Risk/Prognostic.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Fireworks are often used to celebrate national holidays, religious festivals, and cultural events. A firework is defined as ‘any device activated by combustion, deflagration, or detonation that produces a visual and/or sound effect’ [1]. Firework-related burns are preventable injuries that affects developing and developed countries with different presentations of trauma [2, 3]. The availability of fireworks in unprofessional hands can lead to serious soft tissue and bone injury with potential to impair function and living. There are changing trends of firework types such as shop good fireworks, pertaining to fireworks that can be bought from a local supermarket or store, like sparklers, and professional fireworks reflective of accessibility and availability. Most firework-related admissions are young adult males with hands commonly afflicted [4, 5]. Only about one in five presentations to emergency departments for firework injuries results in admission to hospital [6]. Firework-related injuries in America have an estimated annual cost of $100 million USD [7] with potential for physical and psychological burden for the patient and bystanders of the event.
Despite the effectiveness of control for fireworks with legislation and age restrictions such as the Explosives Act 2013 in Australia, there is anecdotal reporting of increased sales of fireworks, both shop goods and professional types [8]. A 1984 New South Wales (NSW) fireworks study reported injuries at a major trauma centre were caused by misuse behaviours, such as carrying live fireworks in pockets, or standing directly over the firework while igniting it [9]. To date, there has been no Australian statewide review of firework-related burns from major burn units that capture the clinical differences between firework types and sex. This study focuses on identifying patterns of firework-related burns and clinical outcomes in adults treated at the main tertiary centres in NSW, Australia, with the aim to better tailor effective preventative strategies, targeting affected patient populations, and minimise firework-related burns in the future.
Methods
Study setting
The Concord Repatriation General Hospital (CRGH) and Royal North Shore Hospital (RNSH) treat over 2000 patients per year combined for burn-related injuries. CRGH and RNSH are the two major adult tertiary burn centres in NSW, Australian Capital Territory (ACT), and French Polynesian islands. Care is delivered through inpatient, ambulatory care, and outreach services. A retrospective review was conducted at CRGH and RNSH Burns Units from January 1st of 2010 to December 31st of 2020 for patients who presented with firework burns. Inclusion criteria were patients older than 18 years of age with a firework-related burn treated at one of the two burn units.
Data collection and study design
Burn patients referred to either the CRGH or RNSH Burn Centre (in or outpatient services) were clinically assessed by a surgical trainee and/or a specialist surgeon at the time of presentation. Data was retrospectively collected via the Agency of Clinical Innovation Database Statewide Burn Injury Service Network (ACI SBIS) and medical records. Ethics approval was granted from the Human Research and Ethics Committee [2021/ETH00376].
The following recorded parameters were analyzed included social demography and socioeconomic parameters (Index of Relative Socio-economic Advantage and Disadvantage, IRSAD) [10]. Information about the burn injury included adequate first aid use, burn mechanism, substance use, diabetic status, bystander (injured as a bystander), firework type (sparkler, firecracker, firework, other), percentage of total surface area burnt (%TBSA), burn depth (superficial, mid-dermal, full thickness), site of injury (head and neck, upper limb, lower limb, torso, genitals and buttocks, multiple areas (more than one), and associated injuries. Information about management included operative vs non-operative, admission, number of operations, hospital length of stay (LoS), and number of days from outpatient burns ambulatory care to discharge from care.
Statistical analysis
A statistical analysis using SPSS (Version 26.0) was computed for continuous variables assessing the relationship between linear data and correlation based on a level of significance set at p value of 0.05. Continuous variables were expressed as mean, median, inter-quartile range (IQR), and standard deviation (SD). Differences between proportions for men and women derived from categorical data were analyzed using Pearson’s chi-squared test and Mann–Whitney U for continuous variables. Crude rate for hospitalisation of firework burns were calculated by number of injuries per 100,000 population of NSW per year. Poisson linear regression was used to calculate differences in firework types per year.
Results
The total number of firework-related burns over the study period was 203 giving a crude separation rate of 0.24 per 100,000, population per year for NSW (Table 1). In NSW, the average incident per year for sparkler burns was 10.0, firecrackers 2.9, and fireworks 4.8. A reduction of 10.7% per year was reported for firecrackers (OR = 0.893, 95%CI: 0.798–0.998, p = 0.046). There were no significant changes for sparklers and fireworks per year. Fireworks showed a normal distribution of use, whereas sparklers gradually increased, and firecrackers decreased. There was a greater use of fireworks after the introduction of the Australian 2013 Explosive regulation law compared to before the law (81.1% vs 18.9%, p = 0.069).
Patient characteristics
There was a strong male predominance (4:1) with men 5.2 years younger than women (31.2 vs 36.4, p = 0.010; Table 2). The distribution of age for men was positively skewed, whereas women had a normal distribution. The most prevalent age group was 18–25 years (36.5%) followed by 26–35 years (30.0%). Almost half of firework-related burns (45.8%) occurred in summer, predominantly on weekends and in 32.0% (n = 65) during public holidays. Men had a significantly higher proportion of holiday-related firework burns (71.2% vs 55.0%), whereas women predominantly sustained non-holiday-related firework burns (45.0% vs 28.8%, p = 0.050; Table 2). Sixty patients (29.6%) identified as a bystander at the time of injury. The vast majority (93.6%) were accident-related incidents with the remaining work related (5.4%) and assault (1.0%).
Men were more likely to consume alcohol at the time of the injury than women (34.4% vs 12.5%, p = 0.007). Two patients sustained an associated injury (full thickness hand laceration and left ulnar fracture). First aid was adequate in 68.5% (n = 139) of patients. The most common firework used was sparklers (54.2%). Women had significantly higher incidences of sparkler-related burns (77.5% vs 48.5%), whereas men had higher proportions for firecrackers and fireworks (17.8% vs 7.5%, 28.8% vs 15.0%, p = 0.009).
Injury characteristics
The mean TBSA% was 1.2% (± 1.7) with different proportions amongst sex (male = 1.3% vs female = 0.7%, p = 0.067). The upper limb was the most common site of injury with the left-hand accounting for 47.3% (n = 96) of all burn sites. Burn injuries were predominantly (61.6%) of mid-dermal depth and the most prevalent burn depth for all body sites, with the exception of the lower limbs where full-thickness burns were more frequent (Table 2). Sparklers predominantly caused mid-dermal burns (69.4%). Firecrackers had an equal distribution of superficial and mid-dermal burns, whereas fireworks were largely mid-dermal burns (61.4%; Fig. 1). There were no significant differences between sex for site of injury and burn depth.

Firework types vs depth of burn injury
Management
Operative intervention was reported in 17.7% (n = 36) of patients who required debridement and closure with a split-thickness skin graft or biosynthetic dressings (Biobrane®). The vast majority of operative patients were males (n = 30, 83.3%) with an average of 31.3 years (± 11.5). First aid was inadequate in ten patients (27.8%) and sixteen patients (44.4%) were under the influence of alcohol at the time of injury. The TBSA for operative patients was significantly higher by 1.3% compared to non-operative patients (2.2% vs 0.9%, p < 0.001). Of the 36 operative patients, split thickness skin graft was used in 26 patients and biosynthetic dressings (Biobrane®) were used in ten patients. No amputations, flaps, or other reconstructive methods were utilised. There were variations for the operative rates for each anatomical site: head and neck 25.0%, torso 16.7%, upper limbs 16.3%, lower limbs 43.3%, and genitals and buttocks 40%. Biosynthetic dressings were mainly used for upper limbs, followed by lower limbs and genitals, whereas split thickness skin grafts were predominantly used for upper limbs, followed by lower limbs and buttocks. Forty-six patients (22.7%) were admitted to hospital for treatment including operative management, analgesia, and/or social reasons. The total average LoS was 2.2 (± 2.4) days with men having a significantly longer LoS of 1.5 days compared to women (2.5 vs 1.0, p = 0.028). The average number of days from injury to discharge from outpatient clinic was 13.0 (± 11.0) days.
Discussion
Firework burns in NSW have a strong male predominance with distinct patterns of firework types amongst sex resulting from sparklers, fireworks, and less so firecrackers. There was a strong male predominance (4:1) with younger men more likely to get injured than women (31.2 vs 36.4 years, p = 0.010). In Australia, the most prevalent time for firework burns was summer during festive celebrations from the Christmas season to New Year’s Day. In other countries, firework burns during celebratory events have been linked to Spring festival [11], Guy Fawkes [12], Diwali [13], Eid [3], and Independence Day [14].
Almost half our incidents occurred at the weekend and almost a third on holidays. Men were significantly more likely to have firework-related burns on holidays in line with a previous report [15]. These findings suggest that men are significantly more likely to take risky behaviours and drink alcohol at the time of handling fireworks than women (34.4% vs 12.5%, p = 0.007). Women on the other hand had higher incidences on non-holidays, principally sustaining sparkler-related burns from celebratory events. These behaviours undoubtedly contribute to the severity of the injury with men having greater TBSA than women (1.3% vs 0.7%). Furthermore, people from less to least disadvantaged socioeconomic levels were predominantly affected potentially reflecting a difference in firework types and accessibility. A Colombian fireworks study reported, workplace, ethnicity, and lower socioeconomic status had increased odds for mortality [16, 17].
In an earlier American study, McFarland et al. reported ground display fireworks emitting sparks were the most common cause of injury (36%), followed by crackers (34%) [18]. Almost 50 years later, a contemporary review identified differences in firework-related burns for age groups with rockets/homemade fireworks for under 17-year-olds, and shells (spherical explosives launched into the sky) for adults [19]. An Indian study during Diwali showed flare fountains in young children were most common, often unsupervised, with a total of 28.0% associated injuries [13]. The most common type of firework injury identified in our patient cohort was sparklers predominantly resulting in mid dermal burns (69.4%), specifically to the hands with a left hand dominance. Recent studies are in line with our findings that most injuries affect the hands, particularly the thumb of male patients, which are much more likely to be injured than female patients [20, 21].
Sparklers are an inexpensive and easily accessible firework made of metallic fuel with a metal rod often used for birthdays. It is a deceivingly innocuous handheld firework that emits sparks with temperatures up to 2000 °C and continues to remain hot once burnt. In the UK, sparkler burns have been increasingly common over the years [22]. Sparkler burns were also largely responsible for the majority of the legal firework-related injuries in our cohort, particularly in women (77.5%). In men, sparkler burns were significantly less frequent (48.5%, p = 0.009) and included homemade sparkler bombs, which were often positioned around the genitalia and buttocks with serious potential for urological complications and psychological harm. All these cases resulted in mid-dermal and full thickness burns with a 40.0% operative rate using split thickness skin grafts and biosynthetic dressings. Most other sparkler injuries however were managed in the outpatient setting with a relatively low operative rate with appropriate burn dressings.
Firecracker and firework burns were of mid-dermal or full-thickness depth requiring operative management and more common amongst men with a broader distribution for site of injury attributed to the explosive blast. Blast injuries from fireworks have the potential for soft tissue and bone injuries that can impact functional living. Studies have shown that blast exposure can cause vascular vasospasm [23], air emboli from shock waves [24], and partial neuronal degeneration in facial nerves [25]. During Eid in Malaysia, 22 of 32 paediatric cases had firework-associated injuries including nerve, tendon, fractures, or amputation injuries [26]. Three adult cases of firecrackers have previously been reported in NSW who suffered an explosive injury resulting in degloving of the digits, loss of neurovascular bundles, Bennett’s-type fractures, and first-web soft-tissue losses [27]. The combination of blast and burn injuries also has the potential to impact bystanders and operator. A Northern territory study reported females and children were more likely to be injured as bystanders with similar rates compared to our study of 29.6% [28]. Although we did not report any injuries similar to the aforementioned studies, the present study reported two associated injuries including soft tissue lacerations and ulnar fracture.
The vast majority of our operative management was debridement and split thickness skin grafts (n = 26) and biosynthetic dressings (n = 10). A British study on blast burn injuries reported similar findings with a young male predominance having partial thickness burns to the upper limbs [29]. Blast injuries similar to firework injuries have the high potential for soft and bone tissue injury with the aforementioned study reporting a greater average TBSA of 36.6%, but a much lower operative rate of 11.9% compared to 17.7% (Table 2). An American upper extremity firework burns series reported 70.2% cases of thermal injuries, but with the remaining experiencing lacerations, amputations, and fractures [30]. Although the study did not outline the operative rates and reconstructive management, our experience was vastly different to our American constituents with only two associated injuries. Of the 36 operative cases, we largely used split thickness skin grafts for the upper limbs, lower limbs, and buttocks. We also employed biosynthetic dressings (Biobrane) for arms, hands, feet and the genital region.
Under the Dangerous Goods Act 1985, some fireworks such as Chinese firecrackers, sparklers, model rocket motors, and toy pistol caps are not banned, which are largely attributed for most presentations [31,32,33,34]. In NSW, current restrictions to the use of fireworks are made under the Dangerous Goods (General) Regulation 1999, but there are variations amongst Australian states and territories in regulation of sale and use of shopgood fireworks. Legislation has shown to be an effective measure with the minimum age of purchase for the lightest category of fireworks at 12 years in the Netherlands [35, 36]. Countries with restrictive firework laws had an 87% lower trauma incidence rate [37], whereas liberalisation of firework laws demonstrated an increase in events and injury rate [38,39,40].
Shopgood fireworks are a growing area of concern amongst young adults. We noted a large portion of young men created homemade like explosives (sparkler bombs) from over 100 sparklers in bottles that can incur serious blast, burn, and life-threatening injuries. Sparklers represented the majority of firework burns and emphasis on education awareness and regulation control in supermarkets, like cigarettes and spray cans, should follow suit. The average crude rate over the decade compared to the 1990s in NSW had increased (0.18 vs 0.24; Table 1) [41]. However, firecracker injuries showed a 10.7% reduction over the study period and fireworks showed an increasing trend following the 2013 legislation. Harm minimisation and control of purchase of these everyday goods to young adults such as limiting the number purchased, age restrictions, and access are potential avenues. The success of educational awareness campaigns has been demonstrated in reducing firework-related casualties [42, 43]. A multisector response focused on education and awareness is required from corporations, health bodies, and governments.
There are limitations within the study that reflect the retrospective nature and selection bias. Events surrounding the use of fireworks in some cases were not fully disclosed as to patients were bystanders, victims, or perpetrators. We believe that this number is likely an underestimate as there may be a vast number of minor burn presentations from sparklers, which are not all referred to burn units. Although this study was adult focused, our colleagues have recently published similar concerns with sparkler use in the paediatric population [44]. Furthermore, inter-observer bias potentially influenced burn depth assessment without objective measurement tools such as laser Doppler imaging. This statewide review is the first and largest in Australia that can provide insight into necessary educational campaigns and interventions to young adults, particularly with sparklers. National harmonisation of legislation surrounding sale and use of fireworks is critical, but also improving community awareness and corporations about the dangers of shopgood fireworks.
Conclusions
Firework injuries have distinct profile patterns amongst men and women with risk taking behaviours influencing the type and severity of injury. These preventable injuries can be devastating from the combination of burn and blast forces. Alongside legislation, awareness of the potential hazards for shopgood fireworks such as sparklers is critical for future prevention campaigns.
References
American Pyrotechnic Association. Glossary of pyrotchnic terms. 2016. Accessed 6/6/21, http://www.americanpyro.com/glossary-of-pyrotechnic-terms. 2016.
Van Yperen DT, Van Lieshout EMM, Dijkshoorn JN, Van der Vlies CH, Verhofstad MHJ (2021) Injuries, treatment, and impairment caused by different types of fireworks; results of a 10 year multicenter retrospective cohort study. Scand J Trauma Resusc Emerg Med 29(1):11
Rashid RA, Heidary F, Hussein A, Hitam WH, Rashid RA, Ghani ZA, Omar NA, Mustari Z, Shatriah I (2011) Ocular burns and related injuries due to fireworks during the Aidil Fitri celebration on the East Coast of the Peninsular Malaysia. Burns 37(1):170–173
Puri V, Mahendru S, Rana R, Deshpande M (2009) Firework injuries: a ten-year study. J Plast Reconstr Aesthet Surg 62:1103–1111
NHS Digital. Hospital episode statistics for England. Admitted Patient Care statistics, 2017–18. n.d.
Abdulwadad O, Ozanne-Smith J (1998) Injuries associated with fireworks in Victoria: an epidemiological overview. Inj Prev 4:272–274
From the Centers for Disease Control and Prevention 2000 Injuries from fireworks in the United States JAMA 284 302
Edwin A, Cubison T, Pape S (2008) The impact of recent legislation on paediatric fireworks injuries in Newcastle upon Tyne Region. Burns 34(7):954–964
Cunningham P, Gaudry P (1984) Misuse of fireworks [letter]. Med J Aust 15:399
Australian Bureau of Statistics. Information paper. An introduction to Socio-Economic Indexes for Areas (SEIFA) 2006(2039.0). ABS: Canberra, Australia, 2008.
Wang C, Zhao R, Du WL, Ning FG, Zhang GA (2014) Firework injuries at a major trauma and burn center: a five-year prospective study. Burns 40(2):305–310
Nizamoglu M, Frew Q, Tan A, Band H, Band B, Barnes D, El-Muttardi N, Dziewulski P (2018) The ten-year experience of firework injuries treated at a uk regional burns & plastic surgery unit. Ann Burns Fire Disasters 31(1):13–16
Puri V, Mahendru S, Rana R, Deshpande M (2009) Firework injuries: a ten-year study. J Plast Reconstr Aesthet Surg 62(9):1103–1111
Morrissey PJ, Scheer RC, Shah NV, Penny GS, Avoricani A, Koehler SM (2021) Increases in firework-related upper extremity injuries correspond to increasing firework sales: an analysis of 41,195 injuries across 10 years. J Am Acad Orthop Surg 29(13):e667–e674
Canner JK, Haider AH, Selvarajah S, Hui X, Wang H, Efron DT, Haut ER, Velopulos CG, Schwartz DA, Chi A, Schneider EB (2014) US emergency department visits for fireworks injuries, 2006–2010. J Surg Res 190(1):305–311
Chaparro-Narváez P, Cotes-Cantillo K, Castañeda-Orjuela C, De la Hoz-Restrepo F (2017) Injuries due to fireworks use: a surveillance data analysis in Colombia, 2008–2013. Burns 43(1):149–156
Di Pierro MC (2008) Educação de jovens e adultos na América Latina e Caribe: trajetória recente. Cad Pesqui 38:367–391
McFarland LV, Harris JR, Kobayashi JM, et al. Risk factors for fireworks-related injury in Washington State. JAMA 1984;251:3251e4.
Jacobson L, Sandvall BK, Quistberg DA, Rowhani-Rahbar A, Vavilala MS, Friedrich JB, Keys KA (2021) Severe fireworks-related injuries: demographic characteristics, injury patterns, and firework types in 294 consecutive patients. Pediatr Emerg Care 37(1):e32–e36
van der Zee C, Smeulders M, van de Kar A (2014) Hand injuries caused by fireworks and treated by plastic surgeons. Ned Tijdschr Geneeskd 158:A8381
Sandvall BK, Keys KA, Friedrich JB (2017) Severe hand injuries from fireworks: injury patterns, outcomes, and fireworks types. J Hand Surg Am 42:385.e1-385.e8
Singh S. Sparklers as major hazard for burn injury. Burns 1997; 23:369e72.
Bauman RA, Ling G, Tong L, et al. An introductory characterization of a combat casualty-care relevant swine model of closed head injury resulting from exposure to explosive blast. J Neurotrauma 2009;26:841–60.10.
WvanH Mason, Damon TG, Dickinson AR et al (1917) Arterial gas emboli after blast injury. Proc Soc Exp Biol Med 136:1253–5
Telischi FF, Patete ML (1994) Blast injuries to the facial nerve. Otolaryngol Head Neck Surg 111:446–449
Al-Qattan MM, Al-Tamimi AS (2009) Localized hand burns with or without concurrent blast injuries from fireworks. Burns 35(3):425–429
MacKenzie DN, Green JA, Viglione W (2001) Firecracker injuries to the hand. Med J Aust 174(5):231–232
Read DJ, Bradbury R, Yeboah E (2017) Firework-related injury in the top end: a 16-year review. ANZ J Surg 87(12):1030–1034
Patel JN, Tan A, Dziewulski P (2016) Civilian blast-related burn injuries. Ann Burns Fire Disasters 29(1):43–46
Serra López VM, Cheema AN, Gray BL, Pirruccio K, Kazmers NH (2020) Epidemiology of fireworks-related injuries to the upper extremity in the United States From 2011 to 2017. J Hand Surg Glob Online 2(3):117–120
The Dangerous Goods (Explosives) Regulations 1988. Statutory Rules 1988. Volume 2, No 272. Victoria, Australia.
The Dangerous Goods Act 1985. Acts of Parliament, 1985. No 10189. Victoria, Australia.
The Explosives (Fireworks Prohibition) order No 1/1982. Statutory Rules 1982. Volume 1, No 151. Victoria, Australia.
The Explosives Act 1960. Acts of Parliament 1960. No 6715. Victoria, Australia.
Rijksoverheid. Wat moet ik weten als ik vuurwerk koop? 2019 [Available from: https://www.rijksoverheid.nl/onderwerpen/vuurwerk/vraag-en-antwoord/wat-moet-ik-weten-als-ik-vuurwerk-koop].
Edwin AF, Cubison TC, Pape SA (2008) The impact of recent legislation on paediatric fireworks injuries in the Newcastle upon Tyne region. Burns 34(7):953–964
Wisse RP, Bijlsma WR, Stilma JS (2010) Ocular firework trauma: a systematic review on incidence, severity, outcome and prevention. Br J Ophthalmol 94(12):1586–1591
Stichting Consument en Veiligheid. Ongevallen met Vuurwerk, 1996e2009. http://www.veiligheid.nl (accessed 21 Jul 2009).
Rudisill TM, Preamble K, Pilkerton C (2020) The liberalization of fireworks legislation and its effects on firework-related injuries in West Virginia. BMC Public Health 20(1):137
Chan WC, Knox FA, McGinnity FG, et al. Serious eye and adnexal injuries from fireworks in Northern Ireland before and after lifting of the firework band an ophthalmology unit’s experience. Int Ophthalmol 2004;25:167e9.
Jorm L. Firework injuries in New South Wales, 1992e93 to 2001e02. NSW Public Health Bull 2003;14:110e13.
D’Argenio P, Cafaro L, Santonastasi F, et al. Capodanno Senza Danno: the effects of an intervention program on fireworks injuries in Naples. Am J Public Health 1996;86:84e6.
Homaie Rad E, Kouchakinezhad-Eramsadati L, Mohtsham- Amiri Z, Davoudi-Kiakalayeh A, Yousefzadeh-Chabok S (2019) Effectiveness of an educational program on decreasing burns and injuries in Persian festival of fire: a burden of diseases approach. Burns 45:46670
Ricciardello D, Yang NK, Chamberlain K, Holland AJA (2021) Firework and sparkler burns in paediatric patients. Australas J Plast Surg 4(1):30–34
Acknowledgements
We would like to extend our acknowledgement to the burns team members at the unit who provided ongoing support. We wish to thank Dr Jeon Cha, Anne Darton, and the New South Wales Agency for Clinical Innovation Statewide Burn Injury Service Data Registry for their assistance with data acquisition.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions
Author information
Authors and Affiliations
Contributions
The authors contributed to the conception and design of the manuscript, revised it critically for important intellectual content, approved the final version to be published, and agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration. This project has been approved by the Human Research Ethics Committee (2021/STE00623).
Informed consent
Informed consent was obtained from the parents or legal guardians. Patient consent has been obtained.
Competing interests
Jason Diab, Zachias Hopkins, Vanessa Diab, Peter KM Maitz, and Andrea C Issler-Fisher declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Diab, J., Hopkins, Z., Diab, V. et al. Patterns and trends of firework-related adult burns in New South Wales, Australia. Eur J Plast Surg 46, 261–269 (2023). https://doi.org/10.1007/s00238-022-01988-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00238-022-01988-5