
Abstract
Background
Since the number of breast cancer genetic gene testing is increasing, more women opt for bilateral prophylactic mastectomy (BPM) followed by breast reconstruction. However, little is known about the differences in Quality of Life (QoL) after various reconstructive surgeries in this population. In this study, the long-term breast-related, body-related, and health-related QoL between immediate implant-based breast reconstruction (IBBR) and autologous breast reconstruction (ABR) were compared, in women who underwent BPM.
Methods
In this cross-sectional study, women who underwent postmastectomy breast reconstruction between January 2015 and December 2018 were invited for an online questionnaire, in which the BREAST-Q, the BODY-Q and the SF-36 were included. Women who underwent BPM and immediate breast reconstruction were included for analysis. Multivariable linear regression analysis was performed to adjust mean differences in patient-reported outcomes between IBBR and ABR for potential confounders.
Results
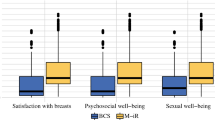
Of the included women (n = 47), 33 underwent ABR and 14 women underwent IBBR following BPM. BREAST-Q scores were in favor of the ABR group before and after adjustment, with statistically significance on Satisfaction with breasts (mean difference 15.8, p = 0.019) and Physical well-being (mean difference 13.5, p = 0.033). None of the mean differences in BODY-Q and SF-36 scores between groups, before and after adjustment, were statistically significant.
Conclusion
This study suggests that there is a higher satisfaction with breasts and better physical well-being in women who underwent immediate ABR compared to those who underwent immediate IBBR after BPM. However, these data should be interpreted carefully as a result of selection bias and a small sample size.
Level of Evidence: Level III, risk study.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Breast cancer is the most common cancer in women. Five to ten percent of all breast cancer cases are hereditary, with BRCA1 and BRCA2 germline gene mutations being accountable for approximately 30% of these cases [1, 2]. Multigene panel testing is increasingly adopted in individuals with an increased risk of hereditary breast cancer. As a result, the number of detected gene mutations is growing [3].
There are several risk-reducing options for women with a high risk of breast cancer. They can choose intensive breast surveillance to detect breast cancer at an early stage, or they can opt for the prophylactic removal of all breast tissue by undergoing a bilateral prophylactic mastectomy (BPM), which reduces the risk of breast cancer by up to 100%. Both options lead to comparable survival rates at age 65 of 98–100% [4]. While risk-reducing surgery can reduce the fear of cancer, removing healthy breasts is a radical choice with potential surgical complications and altered body image as a result [5,6,7]. Studies have shown that breast reconstruction can restore body image and Quality of Life (QoL) after mastectomy [8,9,10,11]. It has its positive effects on sexual and psychosocial well-being. Therefore, a rising number of women opt for breast reconstructive surgery after mastectomy [12, 13].
In order to facilitate decision-making whether or not to undergo BPM and breast reconstruction, women must be informed about the benefits and drawbacks of the different options. Short-term complication rates as well as long-term QoL outcomes should be an important part of patient counseling. However, little is known about the long-term QoL outcomes in this specific population in terms of physical, psychosocial, and sexual well-being, as well as satisfaction with their choice, satisfaction with breasts, and satisfaction with body image. Studies showed mixed results, were based on small sample sizes, and used non-validated or generic questionnaires [14]. This results in a paucity of high-quality data on long-term QoL in women with a high risk of breast cancer. Therefore, more research using validated patient-reported outcomes measures (PROMs) is required.
The aim of this study was to evaluate long-term breast-related, body-related, and health-related QoL in women who underwent BPM and immediate breast reconstruction and to compare implant-based breast reconstruction (IBBR) to autologous breast reconstruction (ABR).
Materials and methods
Patient selection and data collection
Patient demographics, medical history, and patient-reported outcomes of all women who underwent postmastectomy breast reconstruction in either Maastricht University Medical Centre (MUMC +) or Zuyderland Medical Centre between January 2015 and December 2018 were collected through an online survey. Women aged 18 years or older who underwent IBBR or ABR following BPM were included for analysis. Exclusion criteria were unilateral mastectomy, unilateral reconstruction, delayed reconstruction, mixed reconstruction methods, tertiary breast reconstruction after previously failed reconstruction, and currently distant metastases. Women received a personal URL to get access to the online questionnaire (Qualtrics, Provo, UT, USA). A paper version of the questionnaire was available on request. Non-responders received one reminder after three weeks. Medical history, including diagnoses, treatments, and complications, was obtained from the electronic medical record. The manuscript was written according to the STROBE guidelines [15].
Patient-reported outcome measures
The following postoperative scales of the BREAST-Q reconstruction module (Dutch, version 1.0) were used to measure breast-related QoL: Satisfaction with breasts, Satisfaction with outcome, Psychosocial well-being, Sexual well-being, and Physical well-being. Additionally, a study-specific question about satisfaction with reconstruction with the following three answer options was used: I am satisfied with my breast reconstruction (1), I would choose a different reconstruction method (2), and I would no longer opt for breast reconstruction (3).
The BODY-Q was used to assess body image and satisfaction with certain body parts: body, abdomen, buttocks, hips and outer thighs, scars, and body image.
The Short Form 36 (SF-36) was used to measure Health-Related Quality of Life (HRQoL). This PROM consists of eight domains, being Physical functioning, Physical role functioning, Emotional role functioning, Social role functioning, Bodily pain, General mental health, Vitality, and General health perceptions.
Statistical analysis
Patient characteristics were analyzed with descriptive statistics. Q-scores were converted into outcomes from 0 (worst) to 100 (best) with the Q-score software. SF-36 outcomes were transformed into scores from 0 to 100 with higher scores meaning better HRQoL. Continuous variables were represented as mean and standard deviation (SD). Categorical variables were represented as counts and percentages (%). The independent-samples t-test was used to compare the mean outcomes of continuous variables, categorical variables were compared using the Pearson’s chi-square test or the Fisher’s exact test, and ordinal data were compared using the Mann–Whitney U test. Multivariable linear regression was performed to adjust mean differences in patient-reported outcomes between IBBR and ABR for potential confounders. Independent variables were determined a priori, based on literature and professional experience. For the BREAST-Q model, the following variables were selected: age, BMI, smoking, and mastectomy type. For the BODY-Q model, variables selected were age, BMI, smoking, and salpingo-oophorectomy. The outcomes of the SF-36 were adjusted for the following independent variables: age, BMI, active smoker, allergies, chronic illness, mastectomy type, and salpingo-oophorectomy.
A p value ≤ 0.05 was considered statistically significant. All analyses were performed in IBM SPSS Statistics version 25.
Results
Patient characteristics
Of the 887 living women who underwent breast reconstruction during the study period, 444 responded. Of these, 63 women underwent BPM. Sixteen women did not meet the eligible criteria and were therefore excluded from the analyses. Of the included women (n = 47), 33 underwent ABR, and 14 women underwent IBBR following BPM (Fig. 1). The mean age of ABR patients (mean 42.6 ± 8.3) was significantly higher (p = 0.002) than IBBR patients (mean 33.0 ± 10.7). Mean BMI was 26.3 ± 4.4 in the ABR group compared to 23.5 ± 4.6 in the IBBR group (p = 0.057). Five women underwent BPM because of a familial increased risk of breast cancer, without a genetic mutation being detected. In one case, a CHEK2 mutation was diagnosed. In the remaining cases, a BRCA1 and/or BRCA2 germline gene mutation was the reason for BPM. More than half of the women in the ABR group also underwent salpingo-oophorectomy compared to 21% in the IBBR group (p = 0.052). Median follow-up was 39.0 and 39.5 months in the ABR and IBBR group, respectively (p = 0.630). Patient demographics are presented in Table 1.

Flowchart of patient inclusion
Complications
Complications that occurred within 3 months of breast reconstruction are described in Table 2. Minor complications of the breast occurred in nine patients after ABR and three patients after IBBR. Infection was significantly more common after IBBR than after ABR (p = 0.026).
Minor donor site complications occurred in eight ABR cases, with infection being the most common complication (n = 4). Major complications occurred in four IBBR and two ABR cases (p = 1.000). Six cases of ABR and two cases of IBBR required an unplanned reoperation (p = 1.000).
Patient-reported outcomes
BREAST-Q
Women who underwent ABR reported higher scores on all BREAST-Q domains. After adjusting for potential confounders, statistically significantly higher scores were found on Satisfaction with breasts (mean difference 15.8, p = 0.019) and Physical well-being (mean difference 13.5, p = 0.033) in the ABR group.
BODY-Q
Women who underwent IBBR scored higher on all BODY-Q domains. After adjusting for potential confounders, only the mean scores of Hips and outer thighs and Scars were higher in IBBR patients. None of these mean differences were statistically significant.
SF-36
Women in the ABR group reported higher scores in all domains of the SF-36 except for Social functioning and Mental health. After adjusting for potential confounders, women in the ABR group scored slightly, but not statistically significant, higher on all SF-36 domains.
Patient satisfaction
When asked whether, in retrospect, women were satisfied with their breast reconstruction choice, 29 of the ABR patients compared to 9 of the IBBR patients answered positively. The remaining women, being four of the ABR patients and five of the IBBR patients, would have chosen another reconstruction method. However, there were no major differences in complications between these groups (p = 0.810). In both groups, none of the women would not opt for breast reconstruction again. However, this difference in satisfaction with reconstruction was not statistically significant (p = 0.102). Table 3 provides an overview of all PROMs.
Discussion
The aim of this study was to evaluate breast-related, body-related, and health-related QoL in women who underwent BPM and immediate breast reconstruction and to compare IBBR to ABR.
Our study showed that women who underwent ABR reported higher BREAST-Q scores than the IBBR group, with significantly higher satisfaction with breasts and better physical well-being. The adjusted mean difference in Satisfaction with breasts suggests that several confounders in the model, such as age and BMI, do affect this domain. These findings contrast with those of a descriptive study by Metcalfe et al., which reported no difference in satisfaction between IBBR and ABR among 37 women with BPM and breast reconstruction. However, a study-specific questionnaire was used, and the results can therefore not compared directly to our results [16]. In a cross-sectional retrospective study by Moberg et al., women after BPM were significantly less satisfied with breast and outcomes after IBBR (n = 157) than after ABR (n = 18). In addition, the ABR group reported higher scores in all BREAST-Q domains, with the exception of Sexual well-being, which is largely consistent with our results [17]. Toyserkani et al. were the first to compare BREAST-Q data between ABR and IBBR in a systematic review and meta-analysis, which included nine studies. They too found higher satisfaction with breasts and better overall outcome in the ABR group, but physical well-being was similar in both groups [18]. The latter contradicts our results, but can be explained by the differences in baseline characteristics, such as prophylactic or curative mastectomy, radiotherapy, unilateral procedures, and reconstruction timing, which may influence breast reconstruction outcomes according to previous studies. We hypothesize that the more natural-feeling and natural-looking breast, as well as the natural aging of the breast achieved by using the ABR technique, contribute to the better patient-reported outcomes [19].
The lower BODY-Q scores reported by women who underwent ABR may be explained by the additional scarring resulting from flap harvesting, e.g., from the abdomen, which may negatively impact body-related QoL. However, after adjusting for potential confounders, only the mean Hips and outer thighs scores and Scars scores were higher in IBBR patients. The similarities between abdominoplasty and DIEP flap harvest may cause better abdominal and body outcomes in ABR patients [20]. Nevertheless, the mean differences in BODY-Q outcomes between the two groups were not statistically significant.
Health-related QoL was similar in both groups in our study. This is in line with the previously mentioned findings of Moberg et al. [17]. Complications can be a confounding variable for health-related outcomes. With the exception of infection, no significant difference in complications was found between the two methods and is therefore unlikely to have influenced the HRQOL outcomes of this study. In terms of HRQoL, it can be suggested that one technique is not superior to another.
This study had several limitations. The study was nonrandomized, suggesting that it is likely that women were not all eligible for both types of breast reconstruction. In addition, no preoperative patient reported outcome data was available. Psychosocial factors such as family members with breast cancer and/or fear of breast cancer may play an important role in the QoL outcomes of this population. No adjustments could be made for these elements. Another limitation of this study is the small sample size and the low significance level, which both does not benefit the generalizability.
Major strengths of this study include the wide range of questionnaires administered and a strong statistical model in which specific covariates for adjustment were chosen carefully based on literature search and clinical experience. However, more large-scale, comparative research using validated PROMs is needed to collect high-quality data on QoL in women who underwent BPM and breast reconstruction.
Conclusions
This study suggests that there is a higher satisfaction with breasts and better physical well-being in women who underwent immediate ABR compared to IBBR after BPM. However, the results should be interpreted carefully due to possible selection bias and the limitations inherent in the cross-sectional design. Further research with a larger sample size is needed to elaborate on the findings of this study and to provide recommendations for clinical practice.
References
Kuchenbaecker KB, Hopper JL, Barnes DR, Phillips KA, Mooij TM, Roos-Blom MJ, Jervis S, van Leeuwen FE, Milne RL, Andrieu N, Goldgar DE, Terry MB, Rookus MA, Easton DF, Antoniou AC, McGuffog L, Evans DG, Barrowdale D, Frost D, Adlard J, Ong KR, Izatt L, Tischkowitz M, Eeles R, Davidson R, Hodgson S, Ellis S, Nogues C, Lasset C, Stoppa-Lyonnet D, Fricker JP, Faivre L, Berthet P, Hooning MJ, van der Kolk LE, Kets CM, Adank MA, John EM, Chung WK, Andrulis IL, Southey M, Daly MB, Buys SS, Osorio A, Engel C, Kast K, Schmutzler RK, Caldes T, Jakubowska A, Simard J, Friedlander ML, McLachlan SA, Machackova E, Foretova L, Tan YY, Singer CF, Olah E, Gerdes AM, Arver B, Olsson H (2017) Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA 317:2402–2416
Mavaddat N, Peock S, Frost D, Ellis S, Platte R, Fineberg E, Evans DG, Izatt L, Eeles RA, Adlard J, Davidson R, Eccles D, Cole T, Cook J, Brewer C, Tischkowitz M, Douglas F, Hodgson S, Walker L, Porteous ME, Morrison PJ, Side LE, Kennedy MJ, Houghton C, Donaldson A, Rogers MT, Dorkins H, Miedzybrodzka Z, Gregory H, Eason J, Barwell J, McCann E, Murray A, Antoniou AC, Easton DF (2013) Cancer risks for BRCA1 and BRCA2 mutation carriers: results from prospective analysis of EMBRACE. J Natl Cancer Inst 105:812–822
Wang YA, Jian JW, Hung CF, Peng HP, Yang CF, Cheng HS, Yang AS (2018) Germline breast cancer susceptibility gene mutations and breast cancer outcomes. BMC Cancer 18:315
Heemskerk-Gerritsen BAM, Jager A, Koppert LB, Obdeijn AI, Collée M, Meijers-Heijboer HEJ, Jenner DJ, Oldenburg HSA, van Engelen K, de Vries J, van Asperen CJ, Devilee P, Blok MJ, Kets CM, Ausems M, Seynaeve C, Rookus MA, Hooning MJ (2019) Survival after bilateral risk-reducing mastectomy in healthy BRCA1 and BRCA2 mutation carriers. Breast Cancer Res Treat 177:723–733
Hatcher MB, Fallowfield L, A’Hern R (2001) The psychosocial impact of bilateral prophylactic mastectomy: prospective study using questionnaires and semistructured interviews. BMJ 322:76
Brandberg Y, Sandelin K, Erikson S, Jurell G, Liljegren A, Lindblom A, Lindén A, von Wachenfeldt A, Wickman M, Arver B (2008) Psychological reactions, quality of life, and body image after bilateral prophylactic mastectomy in women at high risk for breast cancer: a prospective 1-year follow-up study. J Clin Oncol 26:3943–3949
Gopie JP, Mureau MA, Seynaeve C, Ter Kuile MM, Menke-Pluymers MB, Timman R, Tibben A (2013) Body image issues after bilateral prophylactic mastectomy with breast reconstruction in healthy women at risk for hereditary breast cancer. Fam Cancer 12:479–487
Lagendijk M, van Egdom LSE, Richel C, van Leeuwen N, Verhoef C, Lingsma HF, Koppert LB (2018) Patient reported outcome measures in breast cancer patients. Eur J Surg Oncol 44:963–968
Santosa KB, Qi J, Kim HM, Hamill JB, Wilkins EG, Pusic AL (2018) Long-term patient-reported outcomes in postmastectomy breast reconstruction. JAMA Surg 153:891–899
Nelson JA, Tchou J, Domchek S, Sonnad SS, Serletti JM, Wu LC (2012) Breast reconstruction in bilateral prophylactic mastectomy patients: factors that influence decision making. J Plast Reconstr Aesthet Surg 65:1481–1489
Pusic AL, Matros E, Fine N, Buchel E, Gordillo GM, Hamill JB, Kim HM, Qi J, Albornoz C, Klassen AF, Wilkins EG (2017) Patient-reported outcomes 1 year after immediate breast reconstruction: results of the mastectomy reconstruction outcomes consortium study. J Clin Oncol 35:2499–2506
Skraastad BK, Knudsen C, Jackson C, Utheim TP, Pripp AH, Tønseth KA (2019) Quality of life, patient satisfaction and cosmetic outcome after delayed breast reconstruction using DIEP flap: a 10 years’ follow-up survey. J Plast Surg Hand Surg 53:119–124
Cordeiro PG (2008) Breast reconstruction after surgery for breast cancer. N Engl J Med 359:1590–1601
Razdan SN, Patel V, Jewell S, McCarthy CM (2016) Quality of life among patients after bilateral prophylactic mastectomy: a systematic review of patient-reported outcomes. Qual Life Res 25:1409–1421
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP (2007) The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. The Lancet 370:1453–1457
Metcalfe KA, Semple JL, Narod SA (2004) Satisfaction with breast reconstruction in women with bilateral prophylactic mastectomy: a descriptive study. Plast Reconstr Surg 114:360–366
Moberg IO, Schou Bredal I, Schneider MR, Tønseth KA, Schlichting E (2018) Complications, risk factors, and patients-reported outcomes after skin-sparing mastectomy followed by breast reconstruction in women with BRCA mutations. J Plast Surg Hand Surg 52:234–239
Toyserkani NM, Jørgensen MG, Tabatabaeifar S, Damsgaard T, Sørensen JA (2020) Autologous versus implant-based breast reconstruction: a systematic review and meta-analysis of Breast-Q patient-reported outcomes. J Plast Reconstr Aesthet Surg 73:278–285
Atisha DM, Rushing CN, Samsa GP, Locklear TD, Cox CE, Shelley Hwang E, Zenn MR, Pusic AL, Abernethy AP (2015) A national snapshot of satisfaction with breast cancer procedures. Ann Surg Oncol 22:361–369
Ingvaldsen CA, Tindholdt TT, Tønseth KA (2018) DIEAP flap patients equally as satisfied with the abdomen as abdominoplasty patients. Plast Reconstr Surg Glob Open 6(8):e1876. https://doi.org/10.1097/GOX.0000000000001876
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by the first three authors. The first draft of the manuscript was written by the first three authors, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
The study was approved by the institutional review board of Maastricht University Medical Center (METC2020-2232) and Zuyderland MC (METCZ20200113).
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Conflict of interest
Renée M. L. Miseré, Milou E. M. Joosen, Eva L. Claassens, Andrzej A. Piatkowski de Grzymala, Esther M. Heuts, and René R. W. J. van der Hulst declare no conflict of interest.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Miseré, R.M.L., Joosen, M.E.M., Claassens, E.L. et al. Patient-reported outcomes following bilateral prophylactic mastectomy and immediate breast reconstruction: comparing implant-based with autologous breast reconstruction. Eur J Plast Surg 45, 763–769 (2022). https://doi.org/10.1007/s00238-022-01950-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00238-022-01950-5