
Abstract
Background
Obesity is pandemic nowadays, and hanging skin with consequent functional and psychological impairments is a common price to pay for massive weight loss. Plastic surgery in postbariatric patients represents a fundamental step to regain possession of a positive self-image. The authors aimed to investigate how EU countries’ National Health System (NHS) behaves regarding reimbursements for body-contouring procedures after massive weight loss.
Methods
A 1-item survey was sent to contacts found on the NHS official Web sites of 27 EU countries. The question focused on postbariatric surgery practice and investigated the accessibility criteria for NHS coverage concerning body-contouring procedures after massive weight loss.
Results
Responses were collected between January 2020 and February 2020. Response rate was 65%, and access criteria to NHS coverage for postbariatric surgery presented great variation across EU countries. Only one country presented an NHS with no coverage for postbariatric surgeries.
Conclusions
Despite the conspicuous variability found among the EU NHS, none of them admit reimbursement in cases of merely aesthetic procedures: postbariatric patients need to display functional or health impairments due to the extensive weight loss. The results of the current study describe a complex situation among EU countries, but a common lead towards postbariatric patients’ care shows off. The ultimate goal of bariatric patient’s healing should be full restoration of physical and psychological well-being. NHS of EU countries are facing this increasing request in various ways, and more studies should be performed in order to understand which is the best approach.
Level of evidence: Not ratable.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Frenetic and unhealthy lifestyle led obesity to assume an epidemic trend nowadays [1]. Along with an increased risk of morbidity and mortality, obesity has a strong impact on personal and public health and economy [2]. Bariatric surgery, combined to metabolic and medical treatments, represents a validated therapeutic strategy. If compared to lifestyle change alone, it allows a more effective and stable weight loss, and therefore, it abates the associated comorbidities. An increasing number of patients are reported to undergo bariatric procedures [3]. However, the price to pay for massive decrease of weight is the risk of excessive quantities of hanging skin with poor skin tone, which causes functional, aesthetic, and psychological impairments [4]. Hanging skin folds may cause difficulties in carrying on personal hygiene, possibly leading to itching and dermatologic problems. Patients are often embarrassed by their new body image, and they usually complain about specific body parts such as upper arms, breast, abdomen, and things. All these problems may affect patients’ social life, for a huge impact on relationships, and consequent decay of their psychological state [5].
The role of plastic surgery is to reduce or eliminate these postbariatric deformities and to restore patient’s body appearance, thus optimizing functional results and promoting psychological and social reintegration. As long as plastic surgery plays an important role in the path of these patients as a fundamental step to regain possession of a positive self-image, we do believe that postbariatric surgeries cannot be considered as mere aesthetics procedures. We asked ourselves how EU countries’ National Health System (NHS) behaves regarding reimbursements for body-contouring procedures after massive weight loss. As long as we know, this is the first study to investigate how each EU country faces the problem of body-contouring procedures in postbariatric patients.
Materials and methods
A 1-item questionnaire was distributed by e-mail to contacts found on the NHS official Web sites of 27 EU countries. The question focused on postbariatric surgery practices. In particular, it questioned the accessibility criteria for NHS coverage that patients must meet in order to undergo body-contouring procedures after massive weight loss:
“Dear Sir/Madame, I’m writing to you in order to have information about postbariatric plastic surgery procedures (such as abdominoplasty, arm and thigh lift, breast lift…) in your country. I would like to know if your NHS reimburses plastic surgery when it is practiced not only for aesthetic reasons but to return the integrity of physical appearance, and if it is available only to patients who underwent bariatric surgery or also to patients who had massive weight loss. I would appreciate it if you could send me more detailed information about that or at least if you can address me to an official site. Thank you for your help in this matter.”
Responses were collected between January 2020 and February 2020. In case of nonresponders, a maximum of five attempts were made to reach them, using different official e-mail addresses.
Results
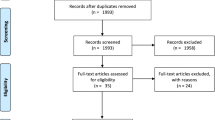
Response rate was 65% with 20 out of 27 countries that answered to our survey. Seven (35%) countries (Austria, Bulgaria, Czech Republic, Hungary, Malta, Portugal, Romania) did not reply even after five attempts to contact them. Responses gathered from the 20 respondents were analyzed and are listed in Table 1. Access criteria to NHS coverage for postbariatric surgery appear to vary greatly across EU countries. None of them admits reimbursement when the surgery aim is merely aesthetic. Patients need to display functional or health disadvantages due to the extensive weight loss.
Only one country (Latvia) clearly states in its response that postbariatric surgeries are not state paid services unlike other plastic surgery procedures such as breast reconstruction after mastectomy or surgical treatment of pressure ulcers.
Among the other 19 responders, the most common criterion for NHS coverage appears to be stable weight for a periods ranging from 6 months in Italy and Denmark to 12 months in the Netherlands, Finland, and Slovenia. The time amount during which the weight must be stable is not precisely indicated by Belgium and Estonia. Moreover, stable BMI ranging from less than 27 to less than 35 is required by Estonia, Italy, Luxembourg, Slovenia, and the Netherlands. Alternatively, Belgium and Luxembourg demand for 20% of total body weight loss after surgery. Age restrictions to minimum 18 years old in applications are provided by Estonia and Luxembourg.
Only the Finnish and Slovenian NHS provide reimbursement also for massive weight loss after dieting and not only after bariatric surgery.
Reimbursement is often restricted to specific procedures, and abdominoplasty is the most commonly covered by NHS. Estonia’s public health covers abdominoplasty only, with a precise criteria: patients have to present folded skin on the abdomen longer than 8 cm and presence of dermatitis, ulcers and or trophic disorders. Similar parameters are required in Luxembourg, where the abdominal apron has to cover the pelvic area completely in order to be eligible for panniculectomy.
Discussion
Excessive and redundant skin affects 89% of postbariatric patients. Loose skin in these patients is refractory to diet and sport activity, and the so-called natural look appears to be a far away mirage [6]. Almost 74% of postbariatric patients express the will to undergo body-contouring surgery [7], seeking to solve skin irritations and infections, mobility impairment, and psychologic distress. The overcoming of mobility obstacle improves patient’s physical activity and reduces the risk of weight regain [8]. The achievement of a positive body image is eased, and self-confidence improves [9]. Moreover, postbariatric surgery is reported to cause anti-inflammatory and metabolic advantages [10]. Despite these achievements and rising patients’ demand for body-contouring procedures, lack of insurance coverage represents the main limiting factor [11].
When NHS does not cover body-contouring procedures, third-party payers can follow medical criteria guidelines for insurance authorization. Usually, a “medical necessity” occurs when an illness, injury or disability requires a cure. If addressed to plastic surgery in postbariatric patients, “medical necessity” and “cosmetic surgery” get mixed up by the insurance companies. A surgery is defined “reconstructive” when it improves loosed function or it repairs congenital or developmental abnormal structures of the body. Meanwhile, a surgery that remodels normal body structures to improve patient’s self-esteem is considered “cosmetic surgery” [12]. The boundary between “reconstructive” and “cosmetic” can be fuzzy, and postbariatric patients may meet impediments obtaining reimbursement for body-contouring surgeries. Song et al. [13] aimed to prove that bariatric surgery reaches its maximum effect when combined to body-contouring. In the UK, despite the majority of bariatric surgeons agree on problems caused by loose skin and the utility of body-contouring surgery to be covered by NHS, there are no national guidelines for postbariatric surgery [14].
To our knowledge, there are no reports that resume EU countries’ NHS coverage for postbariatric body-contouring surgeries. This is the first attempt to describe how EU faces the growing postbariatric patients’ needs. Twenty of 27 EU countries answered to our survey. Among them, only one clearly states that postbariatric surgeries are not covered by NHS. In other 19 countries, public health provides coverage for some specific body-contouring procedures, only if patients can prove functional or health problems. Some of the respondents gave detailed information with regard to the bariatric surgery pathway; others were vaguer. In Spain and Croatia, patients are eligible for massive weight loss surgery only after assessment by the treating physician, when he deems there is a clinical justification to prescribe the procedure.
In Greece and Germany, the clinical approval lies with the statutory health insurance which evaluates patient’s request and confirms a possible coverage of costs.
In France, plastic surgery consultation must be followed by further approval by a medical board of the “Assurance maladie.”
In general, stable weight and BMI maintained inferior to precise levels are the most common criterion for European NHS coverage.
Our results describe a complex situation with many differences among EU countries, but a common lead towards post bariatric patients’ care shows off.
Conclusions
This study does not provide a complete view of EU approach to post bariatric procedures, as 35% of the contacted countries did not reply. We hope that our colleagues from all over Europe will wish to help us in completing this study, giving their comments to this first sketch.
Patient’s healing from obesity is a course of personal transition [15], in which postbariatric surgery represents a fundamental final step [16]. The ultimate goal of bariatric patient’s healing should be his/her conversion to a productive member of society, with full restoration of physical and psychological well-being. NHS of EU countries are facing this increasing request in various ways, and more studies should be performed in order to understand which is the best approach.
References
World Health Organization. WHO global data bases on body mass index. Available on: https://www.who.int/gho/ncd/risk_factors/bmi_text/en/. Accessed 30 March 2020
Nanchahal K, Power T, Holdsworth E et al (2012) A pragmatic randomized controlled trial in primary care of the Camden weight loss (CAMWEL) programme. BMJ Open 2:e000793
Paul MA, Opyrchał J, Knakiewicz M et al (2020) The long-term effect of body contouring procedures on the quality of life in morbidly obese patients after bariatric surgery. PLoS One 15:e0229138
Klassen AF, Cano SJ, Scott A, Johnson J, Pusic AL (2012) Satisfaction and quality-of-life issues in body contouring surgery patients: a qualitative study. Obes Surg 22:1527–1534
Magdaleno R Jr, Chaim EA, Pareja JC, Turato ER (2011) The psychology of the bariatric patient: what replaces obesity? A qualitative research with Brazilian women. Obes Surg 21:336–339
Aldaqal SM, Makhdoum AM, Turki AM, Awan BA, Samargandi OA, Jamjom H (2013) Post-bariatric surgery satisfaction and body-contouring consideration after massive weight loss. N Am J Med Sci 5:301–305
Kitzinger HB, Abayev S, Pittermann A et al (2012) The prevalence of body contouring surgery after gastric bypass surgery. Obes Surg 22:8–12
Froylich D, Corcelles R, Daigle CR et al (2016) Weight loss is higher among patients who undergo body contouring procedures after bariatric surgery. Surg Obes Relat Dis 12:1731–1736
Stuerz K, Piza H, Niermann K, Kinzl JF (2008) Psychosocial impact of abdominoplasty. Obes Surg. 18:34–38
Cintra W, Modolin M, Faintuch J, Gemperli R, Ferreira MC (2012) C-reactive protein decrease after postbariatric abdominoplasty. Inflammation. 35:316–320
Dreifuss SE, Rubin JP (2016) Insurance coverage for massive weight loss panniculectomy: a national survey and implications for policy. Surg Obes Relat Dis. 12:412–416
American Society of Plastic Surgeons (ASPS) (2006) ASPS Recommended insurance coverage criteria for third-party payers. Surgical treatment of skin redundancy for obese and massive weight loss patients. Available on: https://www.plasticsurgery.org/for-medical-professionals/health-policy/recommended-insurance-coverage-criteria. Accessed 30 March 2020
Song P, Patel NB, Gunther S et al (2016) Body Image & Quality of Life: Changes With Gastric Bypass and Body Contouring. Ann Plast Surg. 76:S216–S221
Highton L, Ekwobi C, Rose V (2012) Post-bariatric surgery body contouring in the NHS: a survey of UK bariatric surgeons. J Plast Reconstr Aesthet Surg. 65:426–432
Ficaro I (2018) Surgical weight loss as a life-changing transition: the impact of interpersonal relationships on post bariatric women. Appl Nurs Res. 40:7–12
Lo Torto F, Marcasciano M, Frattaroli JM et al (2020) Quality assessment of online information on body contouring surgery in postbariatric patient. Aesthetic Plast Surg. 44:839–846
Availability of data and material
Not applicable.
Funding
Open Access funding provided by Università degli Studi di Roma La Sapienza.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Jacopo M. Frattaroli, Juste Kaciulyte, Ugo Redi, and Marco Marcasciano. The first draft of the manuscript was written by Federico Lo Torto, and the final revisions were performed by Donato Casella and Diego Ribuffo. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
Federico Lo Torto, Jacopo M. Frattaroli, Juste Kaciulyte, Ugo Redi, Marco Marcasciano, Donato Casella, and Diego Ribuffo declare that they have no conflict of interest.
Ethical approval
This is a survey-based study. The Research Ethics Committee of the institutions involved have confirmed that no ethical approval is required.
Informed consent
This is a survey-based study; there was no necessity for informed consent.
Code availability
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lo Torto, F., Frattaroli, J.M., Kaciulyte, J. et al. Is body-contouring surgery a right for massive weight loss patients? A survey through the European Union National Health Systems. Eur J Plast Surg 44, 459–466 (2021). https://doi.org/10.1007/s00238-020-01779-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00238-020-01779-w