
Abstract
Purpose
A complicated course of the femoral route for neurointervention can prevent approaching the target. Thus, we determined whether transcervical access in the hybrid angiosuite is applicable and beneficial in real practice.
Methods
From January 2014 to March 2017, this approach was used in 17 of 453 (3.75%) cases: 11 cerebral aneurysms (4 ruptured, 7 unruptured), 4 acute occlusions of the large cerebral artery, 1 proximal internal carotid artery (ICA) stenosis, and 1 direct carotid cavernous fistula (CCF).
Results
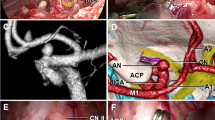
All patients were elderly (mean age, 78.1 years). The main cause was severe tortuosity of the supra-aortic course or the supra-aortic and infra-aortic courses (eight and five cases, respectively), orifice disturbance (three cases), and femoral occlusion (one case). Through neck dissection, 6–8Fr guiding catheters were placed via subcutaneous tunneling to enhance device stability and support. All cerebral aneurysms were embolized (eight complete and three neck remnants) using the combination of several additional devices. Mechanical stent retrieval with an 8Fr balloon guiding catheter was successfully achieved in a few runs (mean, 2 times; range, 1–3) within the proper time window (mean skin to puncture, 17 ± 4 min; puncture to recanalization, 25 ± 4 min). Each stent was satisfactorily deployed in the proximal ICA and direct CCF without catheter kick-back. All puncture sites were closed through direct suturing without complications.
Conclusions
In the hybrid angiosuite, transcervical access via direct neck exposure is feasible in terms of device profile and support when the femoral route has an unfavorable anatomy.




Similar content being viewed by others


References
Kurisu K, Osanai T, Kazumata K, Nakayama N, Abumiya T, Shichinohe H, Shimoda Y, Houkin K (2016) Ultrasound-guided femoral artery access for minimally invasive neuro-intervention and risk factors for access site hematoma. Neurol Med Chir (Tokyo) 56:745–752
Gedikoglu M, Oguzkurt L, Gur S, Andic C, Sariturk C, Ozkan U (2013) Comparison of ultrasound guidance with the traditional palpation and fluoroscopy method for the common femoral artery puncture. Catheter Cardiovasc Interv 82:1187–1192
Larrazabal R, Klurfan P, Sarma D, Gunnarsson T (2010) Surgical exposure of the carotid artery for endovascular interventional procedures. Acta Neurochir 152:537–544
Dorfer C, Standhardt H, Gruber A, Ferraz-Leite H, Knosp E, Bavinzski G (2012) Direct percutaneous puncture approach versus surgical cutdown technique for intracranial neuroendovascular procedures: technical aspects. World Neurosurg 77:192–200
Nii K, Kazekawa K, Onizuka M, Aikawa H, Tsutsumi M, Tomokiyo M, Iko M, Kodama T, Matsubara S, Go Y, Tanaka A (2006) Direct carotid puncture for the endovascular treatment of anterior circulation aneurysms. AJNR Am J Neuroradiol 27:1502–1504
Ribo M, Flores A, Rubiera M, Pagola J, Mendonca N, Rodriguez-Luna D, Pineiro S, Meler P, Alvarez-Sabin J, Molina CA (2013) Difficult catheter access to the occluded vessel during endovascular treatment of acute ischemic stroke is associated with worse clinical outcome. J Neurointerv Surg 5(Suppl 1):i70–i73
Jadhav AP, Ribo M, Grandhi R, Linares G, Aghaebrahim A, Jovin TG, Jankowitz BT (2014) Transcervical access in acute ischemic stroke. J Neurointerv Surg 6:652–657
Yuzawa I, Kurata A, Suzuki S, Ozawa H, Hagiwara H, Niki J, Yamada M, Fujii K, Kan S, Kitahara T (2007) Efficacy of a direct puncture approach for anterior circulation aneurysms using a newly developed guiding catheter—especially for geriatric patients. Surg Neurol 67:30–34; discussion 34
Matsuda Y, Terada T, Masuo O, Matsumoto H, Ohshima K, Tsumoto T, Tsuura M (2013) The clinical results of transcervical carotid artery stenting and frequency chosen as the approach route of carotid artery stenting in 1,067 consecutive cases. Acta Neurochir 155:1575–1581
Levy EI, Boulos AS, Fessler RD, Bendok BR, Ringer AJ, Kim SH, Qureshi AI, Guterman LR, Hopkins LN (2002) Transradial cerebral angiography: an alternative route. Neurosurgery 51:335–340 discussion 340-332
Wiesmann M, Kalder J, Reich A, Brockmann MA, Othman A, Greiner A, Nikoubashman O (2016) Feasibility of combined surgical and endovascular carotid access for interventional treatment of ischemic stroke. J Neurointerv Surg 8:571–575
Ross IB, Luzardo GD (2006) Direct access to the carotid circulation by cut down for endovascular neuro-interventions. Surg Neurol 65:207–211 discussion 211
Ruzsa Z, Nemes B, Pinter L et al (2014) A randomised comparison of transradial and transfemoral approach for carotid artery stenting: RADCAR (RADial access for CARotid artery stenting) study. EuroIntervention 10:381–391
Montorsi P, Galli S, Ravagnani PM, Tresoldi S, Teruzzi G, Caputi L, Trabattoni D, Fabbiocchi F, Calligaris G, Grancini L, Lualdi A, de Martini S, Bartorelli AL (2016) Carotid artery stenting with proximal embolic protection via a transradial or transbrachial approach: pushing the boundaries of the technique while maintaining safety and efficacy. J Endovasc Ther 23:549–560
Mokin M, Snyder KV, Levy EI, Hopkins LN, Siddiqui AH (2015) Direct carotid artery puncture access for endovascular treatment of acute ischemic stroke: technical aspects, advantages, and limitations. J Neurointerv Surg 7:108–113
Blanc R, Piotin M, Mounayer C, Spelle L, Moret J (2006) Direct cervical arterial access for intracranial endovascular treatment. Neuroradiology 48:925–929
Murayama Y, Arakawa H, Ishibashi T, Kawamura D, Ebara M, Irie K, Takao H, Ikeuchi S, Ogawa T, Kato M, Kajiwara I, Nishimura S, Abe T (2013) Combined surgical and endovascular treatment of complex cerebrovascular diseases in the hybrid operating room. J Neurointerv Surg 5:489–493
Iihara K, Satow T, Matsushige T, Kataoka H, Nakajima N, Fukuda K, Isozaki M, Maruyama D, Nakae T, Hashimoto N (2013) Hybrid operating room for the treatment of complex neurovascular and brachiocephalic lesions. J Stroke Cerebrovasc Dis 22:e277–e285
Faggioli G, Ferri M, Rapezzi C, Tonon C, Manzoli L, Stella A (2009) Atherosclerotic aortic lesions increase the risk of cerebral embolism during carotid stenting in patients with complex aortic arch anatomy. J Vasc Surg 49:80–85
Lam RC, Lin SC, DeRubertis B, Hynecek R, Kent KC, Faries PL (2007) The impact of increasing age on anatomic factors affecting carotid angioplasty and stenting. J Vasc Surg 45:875–880
Linfante I, Cipolla MJ (2016) Improving reperfusion therapies in the era of mechanical thrombectomy. Transl Stroke Res 7:294–302
Kaymaz ZO, Nikoubashman O, Brockmann MA, Wiesmann M, Brockmann C (2017) Influence of carotid tortuosity on internal carotid artery access time in the treatment of acute ischemic stroke. Interv Neuroradiol 23:583–588
Son S, Kang DH, Hwang YH, Kim YS, Kim YW (2017) Efficacy, safety, and clinical outcome of modern mechanical thrombectomy in elderly patients with acute ischemic stroke. Acta Neurochir 159:1663–1669. https://doi.org/10.1007/s00701-017-3269-y
Daou B, Chalouhi N, Tjoumakaris S, Hasan D, Barros G, Rosenwasser RH, Jabbour P (2016) Alternative access for endovascular treatment of cerebrovascular diseases. Clin Neurol Neurosurg 145:89–95
Krishnasamy VP, Hagar MJ, Scher DJ, Sanogo ML, Gabriel GE, Sarin SN (2015) Vascular closure devices: technical tips, complications, and management. Tech Vasc Interv Radiol 18:100–112
Cuellar H, Guimaraens L, Ambekar S, Vivas E, Theron J (2015) Angioseal as a hemostatic device for direct carotid puncture during endovascular procedures. Interv Neuroradiol 21:273–276
Morris PP, Braden G (1999) Neurointerventional experience with an arteriotomy suture device. AJNR Am J Neuroradiol 20:1706–1709
Pierot L, Herbreteau D, Bracard S, Berge J, Cognard C (2006) An evaluation of immediate sheath removal and use of the angio-seal vascular closure device in neuroradiological interventions. Neuroradiology 48:45–49
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This study was funded by the Hallym University Research Fund 2016 (HURF-2016-33).
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures in studies involving human participants were performed in accordance with the ethical standards of the institutional and/or national research committee and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Lee, J.Y., Park, JH., Jeon, H.J. et al. Transcervical access via direct neck exposure for neurointerventional procedures in the hybrid angiosuite. Neuroradiology 60, 565–573 (2018). https://doi.org/10.1007/s00234-018-1994-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00234-018-1994-4