
Abstract
In previous work, relationships between muscle and bone size and strength have been demonstrated and were stronger in females, suggesting possible sexual dimorphism. Here we examine sex-specific associations between individual muscle sarcopenia components with clinical outcomes (falls and fractures). 641 participants were recruited. Muscle mass was assessed as cross-sectional area (CSA) by peripheral quantitative computed tomography of the calf, grip strength (GpS) by Jamar dynamometry and function by gait speed (GtS). Falls and fractures were self-reported. Ordinal and logistic regression were used to examine the associations between muscle measurements and outcomes with and without adjustment for confounders. Mean (SD) age was 69.3 (2.6) years. CSA, GpS, and GtS were greater among males (p < 0.002). A higher proportion of females had fallen since age 45 (61.3% vs 40.2%, p < 0.001); in the last year (19.9% vs 14.1%, p = 0.053); and reported a previous fracture since age 45 (21.8% vs 18.5%, p = 0.302), than males. Among females, greater CSA was related to reduced risk of falling and fewer falls in the previous year in fully adjusted analysis only (p < 0.05); higher GpS was related to lower risk of falls since age 45 in unadjusted analysis (p = 0.045) and lower risk of fracture since age 45 in both unadjusted and fully adjusted analysis (p < 0.045). No statistically significant associations were observed for GtS among either sex for any relationships between muscle measurements and clinical outcomes studied. We observed relationships between muscle mass and strength but not function with falls and fractures in females only; further longitudinal studies are required to reproduce these results.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Falls constitute a major risk factor for fracture and associated morbidity, mortality and economic costs [1]. Sarcopenia is an important contributor to falls risk, and hence fractures [2]. We have previously demonstrated relationships between muscle size and grip strength, and bone size and strength, supporting a role for the muscle-bone unit [3], with stronger relationships in females as it has been observed elsewhere [4, 5]. In 2019, the revised European Working Group on Sarcopenia in Older People 2 guidelines were published emphasising muscle strength, relative to muscle mass and function [6]. The aim of this study was to examine the strength of sex-specific associations between each of the key individual sarcopenia components (muscle mass, strength, and function) with the clinically important outcomes of falls and fractures in a population-based cohort of older adults.
Materials and Methods
The Hertfordshire Cohort Study
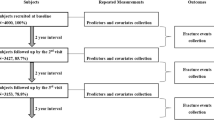
The Hertfordshire Cohort Study (HCS) comprises 2997 individuals born in Hertfordshire from 1931 to 1939 who lived there in 1998–2004 where they completed a home interview and clinic visit for a detailed health assessment. In 2004, of the 966 participants from the geographic region of East Hertfordshire who formed the in-depth musculoskeletal subgroup, 642 attended a clinic visit as part of a musculoskeletal follow-up study. The HCS baseline investigations had ethical approval from the Hertfordshire and Bedfordshire Local Research Ethics Committee and all participants provided written informed consent [7]; ethical approval was also obtained for all HCS follow-up studies. Further details of HCS have been described previously [7].
Ascertainment of Participant Information in 1998–2004
Physical activity (Dallosso questionnaire) was ascertained by a nurse-administered questionnaire [8]. Dietary calcium intake was determined using a food-frequency questionnaire [9]. Current or most recent full-time occupation (husband’s for ever-married females) was ascertained. Social class was coded from the 1990 OPCS Standard Occupational Classification (SOC90) unit group for occupation [10], using computer-assisted standard occupational coding to generate the following occupational classes: I (Professional); II (Managerial and technical); IIINM (Skilled non-manual); IIIM (Skilled manual); IV (Partly skilled); V (Unskilled) [11]. These were dichotomised as follows: ‘Non-manual’ (I, II and IIINM) and ‘Manual’ (IIIM, IV and V). Fractures since age 45 years were self-reported. Among females, information on hormone replacement therapy (HRT) use, the age at which they had their last menstrual cycle and whether they had undergone a hysterectomy was also collected.
Ascertainment of Participant Information in 2004–2005
Information on fractures since baseline, whether participants had fallen since age 45 years, the number of falls in the last year, smoking status and alcohol consumption was ascertained by a nurse-administered questionnaire. History of fracture since age 45 was determined from questionnaire data here and at baseline. Among females, information on HRT use was updated. Height was measured (Harpenden pocket stadiometer, Chasmors Ltd, London, UK) along with weight (SECA floor scale, Chasmors Ltd, London, UK) and used to derive BMI (kg/m2). Grip strength was measured three times for each hand using a Jamar dynamometer; the highest measurement was used for analysis. Customary gait speed in metres per second was calculated using a 3 m walk test. Radial and tibial (non-dominant side) peripheral qualitative computed tomography (pQCT) scans (Stratec 2000XL instrument, version 6.00) were performed; the other side was scanned if the non-dominant side had sustained a fracture. Calf muscle area was derived using default procedures, thresholds, and edge tracking settings to segment muscle from subcutaneous fat. Additional details relating to the pQCT scans have been published previously [12]. At time of assessment of the muscle size, strength, and function measures in this study (2004–2005), 33 (5%) participants were taking bisphosphonates and 113 (18%) were taking medications for the endocrine system. Associations of interest were similar if binary variables for current use of bisphosphonates and medications for the endocrine system were included as additional adjustments as shown in Table 2.
Statistical Methods
Participant characteristics were described using summary statistics. Associations between calf muscle area, grip strength and gait speed in relation to binary outcomes were examined using logistic regression with and without adjustment for age, BMI, social class, smoker status, alcohol consumption, physical activity, dietary calcium intake, hormone replacement therapy use (females only) and time since menopause (females only), use of bisphosphonates and use of medications for the endocrine system. Relationships between predictors and number of falls in the last year (0, 1, > 1) were examined using ordinal regression with the same set of adjustments. Sex-stratified analyses were performed; p < 0.05 was regarded as statistically significant. Analyses were conducted using Stata, release 17.0. The analysis sample comprised 641 participants with data on at least one predictor and at least one outcome; of the 642 participants who attended the 2004–2005 follow-up stage, one participant had missing values for grip strength, gait speed and calf muscle area so they were excluded from the analysis sample.
Results
Descriptive Statistics
Participant characteristics of the analysis sample are presented in Table 1. Mean (SD) age was 69.3 (2.6) years. Calf muscle area, grip strength and gait speed were greater among males than females (p < 0.002 for all associations). Compared to males, a greater proportion of females had fallen since age 45 years (61.3% vs 40.2%, p < 0.001); fallen in the last year (19.9% vs 14.1%, p = 0.053); and had a previous fracture since age 45 years (21.8% vs 18.5%, p = 0.302). However, these latter two sex-differences were not statistically significant.
Relationships Between Muscle Size, Strength, and Function In Relation tTo Falls and Fractures
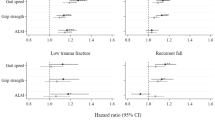
Associations between predictors (calf muscle area, grip strength, gait speed) and outcomes (fallen since age 45, fallen in last year, number of falls in last year, fracture since age 45) are presented in Table 2. Among females, greater calf muscle area was related to reduced risk of falling in the previous year and fewer falls in the previous year (p < 0.05) but only in fully adjusted analysis; higher grip strength was related to lower risk of falls since age 45 in unadjusted analysis only (odds ratio per SD greater grip strength: 0.79 (0.63, 0.99), p = 0.045) and lower risk of fracture since age 45 in both unadjusted (0.74 (0.56, 0.97), p = 0.030) and fully adjusted analysis (0.74 (0.56, 0.99), p = 0.044). No statistically significant associations were observed for gait speed among females, or among males for any of the predictors in relation to any of the outcomes.
Discussion
In this study, higher grip strength was related to lower risk of falls and fractures since age 45 years and greater muscle size was associated with both reduced risk of falling and fewer falls in the previous year. The association between muscle strength and risk of fractures remained robust after adjustments. Conversely, associations regarding muscle size were only significant in adjusted models. Our findings support previous evidence that muscle strength is a key characteristic in detecting older adults at risk of adverse outcomes including falls and fractures [6]. Our study once again demonstrated sexual dimorphism in relationships observed and in general accord with previous literature, although previous studies have also suggested important relationships between muscle measures and bone outcomes in men [5].
Gait speed was not associated with prevalent falls and fractures in this study. Gait speed has been shown to reflect health and functional status, and to be associated with survival in older adults [13,14,15]. We previously found no associations of gait speed with measures of bone size, strength and density in the same cohort [3]. Amongst other physical performance tests, gait speed has previously been shown to be weakly associated with risk of hip fractures in participants without walking difficulties [16]. Gait speed is suitable for screening of poor physical performance and is used to identify cases of severe sarcopenia, as defined by the European Working Group on Sarcopenia in older adults (EWSGOP2) [6], but it is possible that it is more adversely affected by gait ability and/or severe weakness that leads to falls and fractures [17]. Two main types of gait speed assessment exist: the short-and long-distance gait test. Some groups favour the use of long-distance gait speed for its established relationship to mobility disability and public health relevance [18, 19]. Conversely, short gait tests can be used as surrogates for long-distance speed tests for the assessment of functional status in older adults, and are easily implemented into clinical practice [6, 20]. Thus, we suggest that gait speed combined with other physical performance measures, such as chair stand test, might perform better as a predictor of falls and fractures when assessing community-dwelling older adults [16].
There are several strengths and limitations to this work which was undertaken in a very well-characterised cohort that has previously been shown to be representative of the UK population [7]. While the sex differences noted in our study insights into potential differential sex-specific mechanisms, a healthy bias in males, as indicated by the relatively higher mean of grip strength and gait speed, and the use of specific cut-off points to define each sarcopenia components should also be considered as a contributing factor to the absence of associations between sarcopenia and falls and/or fractures in males. However, since the cohort is made up of community-dwelling individuals, generalisability of these findings to less healthy or institutionalized groups may be limited. Specifically, we also acknowledge the limitations associated with self-reported outcomes and the need for prospective data.
Conclusion
In conclusion we have observed relationships between muscle mass and strength but not function with falls and fractures in females but not males. Large prospective studies are needed to confirm the above-mentioned relationships, and to further explore the sexual dimorphism observed.
References
Johnell O, Kanis JA (2006) An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int 17:1726–1733. https://doi.org/10.1007/s00198-006-0172-4
Laskou F, Dennison E, Patel H (2021) The interplay of muscle and bone in later. Life. https://doi.org/10.1007/978-3-030-78128-6_10
Edwards MH, Gregson CL, Patel HP, Jameson KA, Harvey NC, Sayer AA, Dennison EM, Cooper C (2013) Muscle size, strength, and physical performance and their associations with bone structure in the Hertfordshire Cohort Study. J Bone Miner Res 28:2295–2304. https://doi.org/10.1002/jbmr.1972
Soh Y, Won CW (2021) Sex differences in impact of sarcopenia on falls in community-dwelling Korean older adults. BMC Geriatr 21:1–9. https://doi.org/10.1186/S12877-021-02688-8
Yeung SSY, Reijnierse EM, Pham VK, Trappenburg MC, Lim WK, Meskers CGM, Maier AB (2019) Sarcopenia and its association with falls and fractures in older adults: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle 10:485–500. https://doi.org/10.1002/jcsm.12411
Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, Cooper C, Landi F, Rolland Y, Sayer AA, Schneider SM, Sieber CC, Topinkova E, Vandewoude M, Visser M, Zamboni M, Bautmans I, Baeyens JP, Cesari M, Cherubini A, Kanis J, Maggio M, Martin F, Michel JP, Pitkala K, Reginster JY, Rizzoli R, Sánchez-Rodríguez D, Schols J (2019) Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 48:16–31. https://doi.org/10.1093/ageing/afy169
Syddall HE, Simmonds SJ, Carter SA, Robinson SM, Dennison EM, Cooper C, Bevilacqua G, Bloom I, Clynes M, Cox K, Cox V, Fuggle N, Gale C, Holloway J, Jameson K, Parsons C, Patel H, Ward K, Westbury L (2019) The Hertfordshire Cohort Study: an overview. F1000Research. https://doi.org/10.12688/F1000RESEARCH.17457.1
Dallosso HM, Morgan K, Bassey EJ, Ebrahim SB, Fentem PH, Arie TH (1988) Levels of customary physical activity among the old and the very old living at home. J Epidemiol Commun Health 42:121. https://doi.org/10.1136/JECH.42.2.121
Robinson S, Syddall H, Jameson K, Batelaan S, Martin H, Dennison EM, Cooper C, Sayer AA (2009) Current patterns of diet in community-dwelling older men and women: results from the Hertfordshire Cohort Study. Age Ageing 38:594–599. https://doi.org/10.1093/AGEING/AFP121
Office of Population Censuses and Surveys (1990) Standard occupational classification. Structure and definition of major, minor and unit groups, vol 1. HMSO, London
Peter Elias KP, Halstead K (1993) CASOC: computer assisted standard occupational coding. University of Warwick, Coventry
Patel A, Edwards MH, Jameson KA, Ward KA, Fuggle N, Cooper C, Dennison EM (2018) Longitudinal change in peripheral quantitative computed tomography assessment in older adults: the Hertfordshire cohort study. Calcif Tissue Int 103:476–482. https://doi.org/10.1007/s00223-018-0442-0
Studenski S, Perera S, Patel K, Rosano C, Faulkner K, Inzitari M, Brach J, Chandler J, Cawthon P, Connor EB, Nevitt M, Visser M, Kritchevsky S, Badinelli S, Harris T, Newman AB, Cauley J, Ferrucci L, Guralnik J (2011) Gait speed and survival in older adults. JAMA 305:50. https://doi.org/10.1001/JAMA.2010.1923
Harvey NC, Odén A, Orwoll E, Lapidus J, Kwok T, Karlsson MK, Rosengren BE, Ribom E, Cooper C, Cawthon PM, Kanis JA, Ohlsson C, Mellström D, Johansson H, McCloskey E (2018) Measures of physical performance and muscle strength as predictors of fracture risk Independent of FRAX, falls, and aBMD: a meta-analysis of the osteoporotic fractures in men (MrOS) study. J Bone Miner Res 33:2150. https://doi.org/10.1002/JBMR.3556
Harvey NC, Orwoll E, Kwok T, Karlsson MK, Rosengren BE, Ribom E, Cauley JA, Cawthon PM, Ensrud K, Liu E, Cruz-Jentoft AJ, Fielding RA, Cooper C, Kanis JA, Lorentzon M, Ohlsson C, Mellström D, Johansson H, McCloskey E (2021) Sarcopenia definitions as predictors of fracture risk independent of FRAX, falls and BMD in the osteoporotic fractures in men (MrOS) study: a meta-analysis. J Bone Miner Res 36:1235. https://doi.org/10.1002/JBMR.4293
Cawthon PM, Fullman RL, Marshall L, Mackey DC, Fink HA, Cauley JA, Cummings SR, Orwoll ES, Ensrud KE (2008) Physical performance and risk of hip fractures in older men. J Bone Miner Res 23:1037. https://doi.org/10.1359/JBMR.080227
Patel HP, Syddall HE, Jameson K, Robinson S, Denison H, Roberts HC, Edwards M, Dennison E, Cooper C, Sayer AA (2013) Prevalence of sarcopenia in community-dwelling older people in the UK using the European Working Group on Sarcopenia in Older People (EWGSOP) definition: findings from the Hertfordshire Cohort Study (HCS). Age Ageing 42:378–384. https://doi.org/10.1093/ageing/afs197
Pahor M, Pahor M (2022) Mobility and functional outcomes for sarcopenia trials. J Frailty Aging 4:123. /pmc/articles/PMC4643943/. Accessed 1 April, 2022
Peters DM, Fritz SL, Krotish DE (2013) Assessing the reliability and validity of a shorter walk test compared with the 10-Meter Walk Test for measurements of gait speed in healthy, older adults. J Geriatr Phys Ther 36:24–30. https://doi.org/10.1519/JPT.0b013e318248e20d
Beaudart C, Rolland Y, Cruz-Jentoft AJ, Bauer JM, Sieber C, Cooper C, Al-Daghri N, Araujo de Carvalho I, Bautmans I, Bernabei R, Bruyère O, Cesari M, Cherubini A, Dawson-Hughes B, Kanis JA, Kaufman J-M, Landi F, Maggi S, McCloskey E, Petermans J, Rodriguez Mañas L, Reginster J-Y, Roller-Wirnsberger R, Schaap LA, Uebelhart D, Rizzoli R, Fielding RA (2019) Assessment of muscle function and physical performance in daily clinical practice a position paper endorsed by the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Calcif Tissue Int 105:1–14. https://doi.org/10.1007/s00223-019-00545-w
Funding
FL is supported by the NIHR Southampton Biomedical Research Centre, and the University of Southampton. This report is independent research and the views expressed in this publication are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. These funding bodies had no role in writing of the manuscript or decision to submit for publication.
Author information
Authors and Affiliations
Contributions
FL, NRF, MHE, CC, and EMD participated in the conception, design and conduct of the study. LDW conducted the statistical analyses. FL drafted the first version of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
EMD declares consultancy and speaker fees from Pfizer, UCB, Viatris and Lilly. CC has received lecture fees and honoraria from Amgen, Danone, Eli Lilly, GSK, Kyowa Kirin, Medtronic, Merck, Nestlé, Novartis, Pfizer, Roche, Servier, Shire, Takeda and UCB outside of the submitted work. MHE declares conference and course attendance funding from Eli Lilly, other from UCB, other from Pfizer, other from Chugai, other from AbbVie and an unrestricted project grant from Servier. NRF declares travel bursaries from Pfizer and Eli Lilly. LDW and LF declare no conflicts of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and /or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All study participants provided written informed consent and Ethical approval was obtained from the Hertfordshire and Bedfordshire Local Research Ethics Committee.
Informed Consent
Informed consent was obtained from all participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Laskou, F., Westbury, L.D., Fuggle, N.R. et al. Relationships Between Muscle Parameters and History of Falls and Fractures in the Hertfordshire Cohort Study: Do All Muscle Components Relate Equally to Clinical Outcomes?. Calcif Tissue Int 111, 242–247 (2022). https://doi.org/10.1007/s00223-022-00986-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00223-022-00986-w