
Abstract
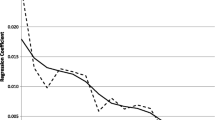
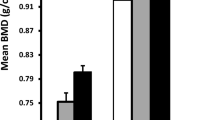
This study reports on ethnic differences in bone mass before and after adjusting for differences in body size and bone area (BA). Lumbar spine (LSBMC), proximal femur (PFBMC) and femoral neck (FNBMC) bone mineral contents were measured in black (‘black’; n = 263) and white (‘white’; n = 73) children from Johannesburg and children of mixed ancestral origin (‘mixed’; n = 64) from Cape Town, South Africa. Geometric estimates and the power coefficient from the regression analyses of BMC on BA were calculated. After adjusting for age, weight, and height, LSBMC in girls and FNBMC in girls and boys were greatest in mixed, followed by black and then white, groups. Mixed boys and girls also had greater PFBMC than their black and white peers, but only in the boys was PFBMC greater in the black than the white groups. When including BA in the adjustment, differences remained at the FN in boys and girls, and the LS and PF in girls, but disappeared at the PF in mixed and black boys. The difference in LSBMC between mixed and black boys became significant after adjustment for age, weight, height, and BA. Geometric estimates at the femoral neck were greater in the mixed group. Power coefficients were greater in the white group, suggesting differences in shape or bone distribution. In conclusion, this study suggests that, in addition to differences in BMC, differences in bone strength and geometry are present which might confer advantages to the bone of mixed-ancestry children.



Similar content being viewed by others

References
Weaver CM, McCabe LD, McCabe GP et al (2007) Bone mineral and predictors of bone mass in white, Hispanic, and Asian early pubertal girls. Calcif Tissue Int 81:352–363
Grant AM, Gordon FK, Ferguson EL et al (2005) Do young New Zealand Pacific Island and European children differ in bone size or bone mineral? Calcif Tissue Int 76:397–403
Daniels ED, Pettifor JM, Schnitzler CM, Russell SW, Patel DN (1995) Ethnic differences in bone density in female South African nurses. J Bone Miner Res 10:359–367
Vidulich L, Norris SA, Cameron N, Pettifor JM (2006) Differences in bone size and bone mass between black and white 10-year-old South African children. Osteoporos Int 17:433–440
Micklesfield LK, Norris SA, Nelson DA, Lambert EV, van der ML, Pettifor JM (2007) Comparisons of body size, composition, and whole body bone mass between North American and South African children. J Bone Miner Res 22:1869–1877
Croxford J, Viljoen D (1999) Alcohol consumption by pregnant women in the Western Cape. S Afr Med J 89:962–965
Carter DR, Bouxsein ML, Marcus R (1992) New approaches for interpreting projected bone densitometry data. J Bone Miner Res 7:137–145
Webber CE, Sala A, Barr RD (2009) Accounting for body size deviations when reporting bone mineral density variables in children. Osteoporos Int 20:113–121
Prentice A, Parsons TJ, Cole TJ (1994) Uncritical use of bone mineral density in absorptiometry may lead to size-related artifacts in the identification of bone mineral determinants. Am J Clin Nutr 60:837–842
Beck T (2003) Measuring the structural strength of bones with dual-energy X-ray absorptiometry: principles, technical limitations, and future possibilities. Osteoporos Int 14(Suppl 5):S81–S88
Richter LM, Yach D, Cameron N, Griesel RD, de Wet T (1995) Enrolment into Birth to Ten (BTT): population and sample characteristics. Paediatr Perinat Epidemiol 9:109–120
Richter LM, Norris SA, de Wet T (2004) Transition from Birth to Ten to Birth to Twenty: the South African cohort reaches 13 years of age. Paediatr Perinat Epidemiol 18:290–301
Pearson J, Dequeker J, Reeve J et al (1995) Dual X-ray absorptiometry of the proximal femur: normal European values standardized with the European Spine Phantom. J Bone Miner Res 10:315–324
Pearson J, Dequeker J, Henley M et al (1995) European semi-anthropomorphic spine phantom for the calibration of bone densitometers: assessment of precision, stability and accuracy. The European Quantitation of Osteoporosis Study Group. Osteoporos Int 5:174–184
Bonnick SL (2007) HSA: beyond BMD with DXA. Bone 41:S9–S12
Macdonald HM, Kontulainen SA, Petit MA, Beck TJ, Khan KM, McKay HA (2008) Does a novel school-based physical activity model benefit femoral neck bone strength in pre- and early pubertal children? Osteoporos Int 19:1445–1456
Zere E, McIntyre D (2003) Inequities in under-five child malnutrition in South Africa. Int J Equity Health 2:7
Mackelvie KJ, Khan KM, McKay HA (2002) Is there a critical period for bone response to weight-bearing exercise in children and adolescents? A systematic review. Br J Sports Med 36:250–257
McVeigh JA, Norris SA, Cameron N, Pettifor JM (2004) Associations between physical activity and bone mass in black and white South African children at age 9 yr. J Appl Physiol 97:1006–1012
Thandrayen K, Norris SA, Pettifor JM (2008) Fracture rates in urban South African children of different ethnic origins: The Birth to Twenty Cohort. Osteoporos Int 20:47–52
Clark EM, Ness AR, Bishop NJ, Tobias JH (2006) Association between bone mass and fractures in children: a prospective cohort study. J Bone Miner Res 21:1489–1495
Zhu K, Greenfield H, Zhang Q et al (2008) Growth and bone mineral accretion during puberty in Chinese girls: a five-year longitudinal study. J Bone Miner Res 23:167–172
Faulkner RA, Davison KS, Bailey DA, Mirwald RL, Baxter-Jones AD (2006) Size-corrected BMD decreases during peak linear growth: implications for fracture incidence during adolescence. J Bone Miner Res 21:1864–1870
Acknowledgments
Appreciation is extended to all funders and research teams of the respective studies presented in this paper. The Cape Town study was funded by the International Atomic Energy Agency. The Johannesburg study was funded by the Wellcome Trust (UK), South African Medical Research Council, and University of the Witwatersrand, Johannesburg. Dr. Micklesfield holds the Hillel Friedland Postdoctoral Fellowship at the University of the Witwatersrand and Dr. Norris holds a Wellcome Trust Postdoctoral Research Fellowship.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
The method for estimating geometry in the femoral neck (FN; T. J. Beck, Sc.D.) is as follows. Structural geometry can be calculated directly from DXA mass image data, but in cases where the image data are not available it is possible to estimate the geometry from conventional outputs, although the method is meaningful only in DXA regions that traverse the long axis of a long bone (FN). It should be realized that the methods are necessarily crude and assume that the bone within the region is a uniform right circular cylinder. This is not a very good assumption in children and persons with smaller bones since cross sections of the FN change greatly in shape along the length of the neck. How much cross sections change in a fixed region length varies with the size of the bone.
FN width (W) is estimated by dividing the neck region area by its fixed length in Hologic scanners, i.e., 1.5 cm. The cross-sectional area (CSA) is computed as
where ρm is the effective density of bone mineral in fully mineralized bone tissue (~1.05 g/cm3).
The section modulus (Z) is computed as
The cross-sectional moment of inertia (CSMI) is computed as
where p is the trabecular porosity and ED is the estimated endosteal diameter.
where f c is the assumed proportion of cortical mass in the FN (0.6).
An estimate of mean cortical thickness is given by
Buckling ratio can then be estimated as
Rights and permissions
About this article
Cite this article
Micklesfield, L.K., Norris, S.A., van der Merwe, L. et al. Comparison of Site-Specific Bone Mass Indices in South African Children of Different Ethnic Groups. Calcif Tissue Int 85, 317–325 (2009). https://doi.org/10.1007/s00223-009-9286-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00223-009-9286-y