
Abstract
Summary
New models describing anthropometrically adjusted normal values of bone mineral density and content in children have been created for the various measurement sites. The inclusion of multiple explanatory variables in the models provides the opportunity to calculate Z-scores that are adjusted with respect to the relevant anthropometric parameters.
Introduction
Previous descriptions of children’s bone mineral measurements by age have focused on segmenting diverse populations by race and sex without adjusting for anthropometric variables or have included the effects of a single anthropometric variable.
Methods
We applied multivariate semi-metric smoothing to the various pediatric bone-measurement sites using data from the Bone Mineral Density in Childhood Study to evaluate which of sex, race, age, height, weight, percent body fat, and sexual maturity explain variations in the population’s bone mineral values. By balancing high adjusted R 2 values with clinical needs, two models are examined.
Results
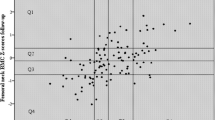
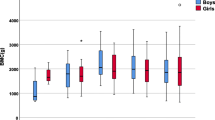
At the spine, whole body, whole body sub head, total hip, hip neck, and forearm sites, models were created using sex, race, age, height, and weight as well as an additional set of models containing these anthropometric variables and percent body fat. For bone mineral density, weight is more important than percent body fat, which is more important than height. For bone mineral content, the order varied by site with body fat being the weakest component. Including more anthropometrics in the model reduces the overlap of the critical groups, identified as those individuals with a Z-score below −2, from the standard sex, race, and age model.
Conclusions
If body fat is not available, the simpler model including height and weight should be used. The inclusion of multiple explanatory variables in the models provides the opportunity to calculate Z-scores that are adjusted with respect to the relevant anthropometric parameters.


Similar content being viewed by others

References
Peck W (1993) Consensus development conference: diagnosis, prophylaxis, and treatment of osteoporosis. Am J Med 94:646–650
Kalkwarf H, Zemel B, Gilsanz V, Lappe JM, Horlick M, Oberfield S, Mahboubi S, Fan B, Frederick MM, Shepherd JA, Winer KK, Shepherd JA (2007) The bone mineral density in childhood study: bone mineral content and density according to age, sex, and race. J Clin Endocrinol Metab 92:2087–2099
Zemel BS, Kalkwarf HJ, Gilsanz V, Lappe JM, Oberfield S, Shepherd JA, Frederick MM, Huang X, Lu M, Mahboubi S, Hangartner T, Winer KK (2011) Revised reference curves for bone mineral content and areal bone mineral density according to age and sex for black and non-black children: results of the Bone Mineral Density in Childhood Study. J Clin Endocrinol Metab 96:3160–3169
Zemel BS, Leonard MB, Kelly A, Lappe JM, Gilsanz V, Oberfield S, Mahboubi S, Shepherd JA, Hangartner TN, Frederick MM, Winer KK, Kalkwarf HJ (2010) Height adjustment in assessing dual energy x-ray absorptiometry measurements of bone mass and density in children. J Clin Endocrinol Metab 3:1265–1273
Lewiecki EM, Gordon CM, Baim S, Leonard MB, Bishop NJ, Bianchi ML, Kalkwarf HJ, Langman CB, Plotkin H, Rauch F, Zemel BS, Binkley N, Bilezikian JP, Kendler DL, Hans DB, Silverman S (2008) International Society for Clinical Densitometry 2007 Adult and Pediatric Official Positions. Bone 6:1115–1121
Wainer H, Thissen D (1975) Multivariate semi-metric smoothing in multiple prediction. J Am Stat Assoc 70:568–573
Khamis H, Guo S (1993) Improvement in the Roche-Wainer-Thissen stature prediction model: a comparative study. Am J Hum Biol 5:669–679
Short DF, Zemel BS, Gilsanz V, Kalkwarf HJ, Lappe JM, Mahboubi S, Oberfield SE, Shepherd JA, Winer KK, Hangartner TN (2011) Fitting of bone mineral density with consideration of anthropometric parameters. Osteoporos Int 4:1047–1057
Tanner J (1962) Growth at adolescence, 2nd edn. Blackwell Scientific, Oxford, UK
McKay HA, MacLean L, Petit M, MacKelvie-O’Brien K, Janssen P, Beck T, Khan KM (2005) “Bounce at the Bell”: a novel program of short bouts of exercise improves proximal femur bone mass in early pubertal children. Br J Sports Med 39:521–526
Neter J, Wasserman W, Kutner M, Richard D (1990) Applied Linear Statistcal Models. Irwin Inc, New York
Horlick M, Wang J, Pierson R Jr, Thornton J (2004) Prediction models for evaluation of total body bone mass with dual-energy x-ray absorptiometry among children and adolescents. Pediatrics 114:E337–E345
Baptista F, Fragosa O, Vieira F (2007) Influence of body composition and weight-bearing physical activity in BMD of pre-pubertal children. Bone 40(Sup 1):S24–S25
Hogler W, Brioday J, Woodhead H, Chan A, Cowell C (2003) Importance of lean mass in the interpretation of total body densitometry in children and adolescents. J Pediatr 143:81–88
Gordi T, Khamis H (2004) Simple solution to a common statistical problem: interpreting multiple tests. Clin Ther 5:780–786
CDC Growth Charts (2000) [Graph illustration Weight for age percentiles: Girls 2 to 20 years] Retrieved from http://www.cdc.gov/growthcharts/data/set1/chart-04.pdf. Accessed Dec 2014
Jackson RL, Kelly HG (1945) Growth charts for use in pediatric practice. J Pediatr 27:215–229
Gordon CM, Bachrach LK, Carpenter TO, Crabtree N, Fuleihan GE, Kutilek S, Lorenc RS, Tosi LL, Ward KA, Ward LM, Kalkwarf HJ (2008) Dual energy x-ray absorptiometry interpretation and reporting in children and adolescents: the 2007 ISCD pediatric official positions. J Clin Densitom 11:43–58
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(XLSX 141 kb)
Rights and permissions
About this article

Cite this article
Short, D.F., Gilsanz, V., Kalkwarf, H.J. et al. Anthropometric models of bone mineral content and areal bone mineral density based on the bone mineral density in childhood study. Osteoporos Int 26, 1099–1108 (2015). https://doi.org/10.1007/s00198-014-2916-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-014-2916-x