
Abstract
Cerebral blood flow increases more during water-based exercise than land-based exercise owing to the effects of end-tidal CO2 (PETCO2) and mean arterial pressure (MAP) changes due to water immersion. However, it is unclear whether oxygenated hemoglobin (oxy-Hb) concentrations in the prefrontal cortex (PFC) are increased more by water-based or land-based exercise. We hypothesized that oxy-Hb concentrations in the PFC are higher during water-based exercise than land-based exercise when the exercise intensity is matched. To test this hypothesis, 10 healthy participants (age: 24.2 ± 1.7 years; height: 1.75 ± 0.04 m; weight: 69.5 ± 5.2 kg) performed light- to moderate-intensity cycling exercise in water (water-based cycling (WC); chest-high water at 30 °C) and on land (LC). Stroke volume, cardio output, heart rate, MAP, respiratory rate, PETCO2, and oxy-Hb in the PFC were assessed during 15 min of exercise, with exercise intensity increased every 5 min. Both WC and LC significantly increased oxy-Hb concentrations in the PFC as exercise intensity was increased (intensity effect: p < 0.001). There was no significant difference in oxy-Hb concentrations during WC and LC in most prefrontal areas, although significant differences were found in areas corresponding to the left dorsolateral PFC (exercise effect: p < 0.001). Thus, WC and LC increase oxy-Hb concentrations in the PFC in a similar manner with increasing exercise intensity, but part of the PFC exhibits enhanced oxy-Hb levels during WC. The neural response of the PFC may differ during water-based and land-based exercise owing to differences in external information associated with water immersion.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Exercise has beneficial effects on cerebral function (Hillman et al. 2008; Guadagni et al. 2020; Voss et al. 2013). Previous studies involving transcranial Doppler examinations and oxygenated hemoglobin (oxy-Hb) concentration measurements in the prefrontal cortex (PFC) revealed that cerebral blood flow (CBF) velocity and increases under light- and moderate-intensity aerobic exercise (Rooks et al. 2010; Smith and Ainslie 2017). However, it is difficult for elderly individuals with declining physical function and/or joint disorders to perform higher intensity exercise, and high exercise intensity can inhibit exercise continuity and motivation (Ekkekakis et al. 2011; Zenko et al. 2016). Thus, middle- and old-aged individuals often prefer water-based exercise because water resistance lowers the risk of falling during exercise and water buoyancy reduces the gravity-induced strain on joints.
CBF is regulated by a coordinated combination of many different systems (Girouard et al. 2006; Paulson et al. 1990). Of these systems, the chemical, cardiovascular, metabolic, and neural systems are well documented, with the main factors affecting CBF regulation cited as cardio output (CO), arterial blood pressure, and carbon dioxide (Querido and Sheel 2007). Immersion in water and water-based exercise induce different physiological responses than being on land and land-based exercise, and the variables typically involved in CBF regulation have been reported to differ during water immersion and water-based exercise. For example, water immersion increases hydrostatic pressure, stroke volume (SV), and CO but decreases heart rate (HR) (Christie et al. 1990; Garzon et al. 2015; Park et al. 1999). End-tidal carbon dioxide (PETCO2) at rest has also been shown to increase during water immersion (Sackett et al. 2017).
Several studies have reported CBF responses during water immersion and water exercise. For instance, water immersion at the femur level increases middle and posterior cerebral artery velocities (Carter et al. 2014). In addition, during water immersion at the right atrium level, light-intensity water-based stepping exercise increases middle and posterior cerebral artery velocities relative to the respective velocities achieved during land-based stepping exercise. The increases in CBF during water immersion at rest and exercise are related to increases in mean arterial pressure (MAP) and PETCO2, suggesting that these two variables contribute to the augmentation of CBF during water-based exercise (Pugh et al. 2015).
Although studies have shown that water-based exercise increases CBF more than land-based exercise, it is not clear how oxy-Hb levels, which reflect neural activity, change in the PFC during water-based exercise. Previous studies have reported that changes in oxy-Hb are related to changes in PETCO2 and hemodynamics (Rooks et al. 2010). Therefore, as a first step to accumulating basic data on the effects of water-based exercise on brain function, we focused on young people. The purpose of the present study was to determine whether oxy-Hb concentrations of the PFC in young adults at light- to moderate-intensity exercise are increased more by water-based exercise or land-based exercise when exercise intensity is matched. We hypothesized that the level of prefrontal oxy-Hb is higher during water-based exercise than land-based exercise owing to the hemodynamic and PETCO2 changes associated with water immersion.
Methods
Participants
Ten healthy participants were enrolled in this study (age: 24.2 ± 1.7 years; height: 1.75 ± 0.04 m; weight: 69.5 ± 5.2 kg; body mass index: 22.7 ± 1.1 kg/m2). All participants were nonsmokers with no history of cardiovascular, musculoskeletal, or metabolic disease or any contraindications to exercise. None of the participants reported taking any medication. This study was approved by the Institutional Ethics committee of Tsukuba University and was performed in accordance with the latest version of the Declaration of Helsinki. Written informed consent was obtained from all participants after they were provided with a complete description of the study.
Experimental protocol
Each participant visited the laboratory three times and one set of measurements were taken per visit in the following order: peak oxygen consumption (VO2peak) measurement, water-based cycling (WC) test, and land-based cycling (LC) test. The participants were instructed to fast for a minimum of 3 h and refrain from vigorous exercise, alcohol consumption, and caffeine intake at least 24 h before each visit. All visits were separated by at least 72 h. We needed to match exercise intensity between WC and LC, but when WC and LC were performed in a random order, it was difficult to match oxygen uptake (VO2) under both conditions. Therefore, based on the VO2 at each stage of WC, the VO2 and ergometer workload (W) values measured in the first VO2peak measurement were applied to the workload at each stage of LC.
VO2peak measurement
We defined the average value for 30 s just before the end of the incremental cycling exercise as the VO2peak. In the test, a recumbent bicycle (Corival Recumbent, Lobe, BV, Netherlands) and expiratory gas analyzer (Aero Monitor, MINATO, Osaka, Japan) were used to assess oxygen uptake during exercise. The ergometric workload was started at 60 W and increased by 20 W every 2 min. At the point where the phase of cycling at 160 W for 2 min was completed, the workload was increased by 10 W until two of the following criteria were met: (1) the participant’s heart rate reached the 95% heart rate reserve, (2) the participant’s respiratory quotient was > 1.2, (3) the participant was unable to maintain cycling at 60 ± 5 rpm, and/or (4) the rate of perceived exercise intensity was > 18.
Cycling procedure
First, the participants practiced the cycling exercise for 15 min with no load and an increase in cadence by 15 rpm every 5 min in each test environment to acclimatize to the cycling exercise under both conditions. Under the WC condition, the participants wore swimwear and rested in a seated position for 5 min out of the water, after which they were submersed in water at 31–32 ℃ to the xiphoid appendix level and sat for 4 min. Since the temperature normally used in ordinary heated swimming pools is set slightly lower than the neutral water temperature of 34 °C, this temperature range was also set for this experiment. Subsequently, the participants conducted 15 min of cycling exercise using a water-based stationary semi-recumbent bicycle (Hydrorecline, H3Oz Company, Italy). The cycling exercise began at 30 rpm, and the cadence was increased by 15 rpm every 5 min (stages 1–3, respectively). Participants maintained the cadence according to the sound of a metronome. To increase pedaling resistance, three plastic paddles (7.0 × 22.0 × 0.5 cm) were placed on the rear wheel. During the exercise test, the participants’ cardiorespiratory and hemodynamic variables were monitored. Under the LC condition, the participants rested in a seated position on the land at room temperature (25–26 ℃) for 5 min, after which they rested for another 4 min to match the WC procedure. After resting, the participants conducted 15 min of cycling exercise. Using a recumbent bicycle (Corival Recumbent), the participants underwent VO2-matched cycling exercise (with the wheel-load adjusted electrically every 5 min), and their cardiorespiratory and hemodynamic variables were measured. During the exercise, we instructed the participants to maintain cadence at 60 rpm (Fig. 1).

Cycling procedure. WC cycling in water, LC cycling on land
Functional near-infrared spectroscopy measurement
We used an 8-channel functional near-infrared spectroscopy (fNIRS) system (OctaMon, Artinis Medical Systems, Netherlands) to measure changes in oxy-Hb levels in the PFC. For fNIRS probe placement, the international 10–20 system was used to ensure consistency. First, we identified the Cz position from the middle point of the nasion and inion and the middle point of the left and right preauricular point. Second, the areas 20% left and right toward the left and right preauricular point from the Cz were set as C3 and C4, respectively. Third, the area 5 cm sagittally from C3 and C4 was covered by CH1 and CH7 of fNIRS, respectively; hence, the left and right dorsolateral PFC (DLPFC) areas were covered with CH1 and CH7, respectively. All parameters were measured using 765 and 855 nm penetrating wavelengths with an emitter to optode distance of 3.5 cm, resulting in a penetrated tissue depth of approximately 1.50–1.75 cm. The 8-channel system recorded the hemoglobin signals at 10 Hz. MATLAB was used to analyze the fNIRS data. First, noise (from head movement) was automatically detected and excluded from the acquired data. Second, timeline data were preprocessed with a bandpass filter using cut-off frequencies of 0.04 Hz to remove baseline drift and 0.7 Hz to filter out heartbeat pulsations. Third, 20 s just before the end of rest before exercise was set as the baseline, and the baseline was subtracted from the oxy-Hb level measured during cycling for 15 min. The oxy-Hb volume in the last 20 s of each 5-min exercise stage was considered the oxy-Hb volume in each stage. Each channel (CH1–8) and all channel averages (All-CH) were analyzed.
Systemic hemodynamics variables
Throughout the experiment, the digital arterial pressure waveform was measured from the participant’s middle finger using a noninvasive blood pressure recording device (INL382, AD Instrument, Colorado Springs, CO, USA), and the data were stored on a computer at 1 kHz of the sampling rate using a data acquisition system (PowerLab, AD Instrument, Colorado Springs, CO, USA) interfaced with a computer running dedicated acquisition and analysis software (LabChart ver.8, AD Instrument). We asked participants to keep their right hand at heart level throughout the rest and exercise periods (placed on a side table outside the bathtub under the WC condition). HR and blood pressure were calculated using the LabChart analysis software, and SV and CO were estimated using the Modelflow-based add-on program for this software.
Breathing pattern
Respiratory rate (RR) and PETCO2 were measured or calculated using the expiratory gas analyzer system (Aero monitor, MINATO, Osaka, Japan) during 4-min rest under each resting condition and 15 min of cycling exercise under each exercise condition. These variables were measured using the breath-by-breath method and averaged over the last 20 s of 4-min rest and each 5-min stage of exercise. Data collection was standardized. The expiratory gas analyzer was calibrated before each experiment according to the manufacturer’s instructions.
Eardrum temperature
The body temperature of each participant was measured according to their right eardrum temperature at rest and at 4 min of each exercise stage.
Estimation of sample size
Sample size and statical power were calculated using the G*Power software. The following parameters were considered according to previous research (Cohen 1992): F test (analysis of variance [ANOVA]); effect size: 0.8; alpha level: 0.05; statistical power: 0.8; number of groups: 2 (WC and LC); number of measurement periods: 3 (stage1, stage2, stage3); and number of participants who refused to participants: 2. As a result, the size of the total sample was 12.
Statistical analysis
Statistical analyses were performed using the Statistical Packages for Social Sciences for Windows version 28 (IBM Inc). Statistical significance was set at p < 0.05. Two-factor repeated-measures ANOVA was used to analyze the exercise factor (WC and LC) and stage factor. Stage factors were classified as follows for each variable: oxy-Hb level: stage 1, stage 2, and stage 3; other parameters: rest, stage 1, stage 2, and stage 3. The change per stage was calculated, and correlation coefficients were used to determine the strength of relationships between the change in oxy-Hb levels (Δoxy-Hb) and the change in other variables (i.e., ΔMAP, ΔRR, ΔPETCO2, and ΔCO) at each stage (i.e., change from rest to stage 1: 1st stage; change from stage 1 to stage 2: 2nd stage; change from stage 2 to stage 3: 3rd stage).
Results
The WC and LC exercise bouts were successfully matched for VO2 (exercise, p < 0.001; stage and exercise–stage interaction, p > 0.05, respectively). %VO2peak changed significantly according to stage (p < 0.001) but not exercise (p > 0.05), nor was their interaction effect significant (p > 0.05). Exercise intensity was about 8% VO2peak at stage 1, 17% VO2peak at stage 2, and 47% VO2peak at stage 3 under both conditions, in which stages 1 and 2 involved light-intensity exercise and stage 3 involved moderate-intensity exercise. The rate of perceived exertion (RPE) changed significantly according to stage (p < 0.001) but not exercise (p > 0.05), nor was their interaction effect significant (p > 0.05) (Table 1). HR increased significantly throughout the stages of both protocols (p < 0.001) but did not differ significantly according to exercise (p > 0.05), nor was the exercise–stage interaction effect significant (p > 0.05) (Table 2).
Oxy-Hb levels
Two-way repeated-measures ANOVA revealed a significant main effect of stage in each CH and All-CH (p < 0.001, respectively). However, exercise was a significant factor for CH7 only (p = 0.039), and the exercise–stage interaction effect was not significant for each CH and All-CH (p > 0.05) (Table 3).
SV and CO
For SV and CO measurements, two-way repeated-measures ANOVA revealed a significant main effect of stage (p < 0.001, respectively), exercise (p = 0.003 and p = 0.007, respectively), and their interaction (p = 0.007 and p = 0.038, respectively). Post hoc tests revealed that SV and CO were significantly higher under WC than under LC at each stage (Fig. 2).

Change in stroke volume (mL) (A) and cardio output (L/min) (B) at rest and each exercise stage. White (○) and black (●) circles indicate WC and LC, respectively. Error bars represent SD. P values according to two-way ANOVA are presented (“stage”, “exercise”, and “interaction”). *P < 0.05, WC vs. LC. a, b, and c indicate differences from rest, stage 1, and stage 2, respectively
PETCO2 and RR
Two-way repeated-measures ANOVA revealed that PETCO2 changed significantly according to stage (p < 0.001) and exercise (p = 0.832), and their interaction effect was significant (p < 0.001). Post-hoc tests revealed that PETCO2 was higher at rest under WC than under LC but higher at stage 3 under LC than under WC. RR changed significantly according to stage (p < 0.001) and exercise (p = 0.166), and their interaction effect was significant (p = 0.035). Post-hoc tests revealed that RR was higher at stage 3 under WC than under LC (Fig. 3).

Change in end-tidal carbon dioxide (mmHg) (A) and respiratory rate (times) (B) at rest and each stage of exercise. White (○) and black (●) circles indicate WC and LC, respectively. Error bars represent SD. P values according to two-way ANOVA are presented (“stage”, “exercise”, and “interaction”). *P < 0.05, WC vs. LC. a, b, and c indicate differences from rest, stage 1, and stage 2, respectively
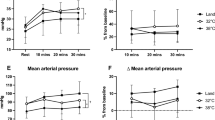
Blood pressure
Two-way repeated-measures ANOVA revealed that systolic blood pressure changed significantly according to stage and exercise (p < 0.001, respectively), but their interaction effect was not significant (p = 0.747). Diastolic blood pressure did not change significantly with stage nor was the exercise–stage interaction effect significant (p > 0.05, respectively), although diastolic blood pressure changed significantly according to exercise (p = 0.006). MAP changed significantly according to stage (p = 0.006), but their exercise and interaction effect was not significant (p = 0.707, p = 0.889, respectively) (Table 2).
Body temperature
Body temperature did not differ according to stage and exercise, and their interaction effect was not significant (p > 0.05, respectively).
Correlation analysis for Δoxy-Hb
According to Pearson product-moment correlation coefficients, in the 1st stage, oxy-Hb under WC was correlated with PETCO2 (r = 0.51) and RR (r = 0.76), while oxy-Hb under LC was correlated with CO (r = − 0.80) and RR (r = 0.7). In the 2nd stage, oxy-Hb under WC was correlated with CO (− 0.44), PETCO2 (r = 0.34), and RR (r = − 0.66) while oxy-Hb under LC was correlated with CO (r = 0.40). In the 3rd stage, oxy-Hb under WC was correlated with RR (r = 0.5) while oxy-Hb under LC was correlated with CO (r = 0.50) and MAP (r = − 0.39).
Discussion
In the present study, we found that oxy-Hb levels increased as the intensity of exercise was increased under both WC and LC conditions; however, oxy-Hb levels were higher under WC than LC in some regions of the PFC.
The WC and LC exercises at light to moderate intensity were successfully matched for VO2, indicating that the exercise protocols were similar in terms of relative intensity among participants. Regarding fNIRS data, we found no changes in tympanic membrane temperature during exercise and no difference in this temperature under WC and LC conditions, suggesting that the effect of oxy-hb on body temperature changes was minimal in both conditions. Previous studies on land-based exercise have found that incremental exercise increases the oxy-Hb concentration in the PFC at the light to high-intensity stage and decreases this concentration at the very high-intensity stage (Garzon et al. 2015). To the best of our knowledge, it was not known whether light- and moderate-intensity water-based exercise enhance the oxy-Hb concentration in the PFC. Thus, we show for the first time that oxy-Hb levels increase in the PFC under light to moderate exercise intensity in both WC and LC protocols; moreover, the oxy-Hb levels did not differ significantly between the WC and LC conditions in most CH at each stage. The mechanisms underlying the increase in oxy-Hb levels according to increasing exercise intensity likely differ between WC and LC. For example, LC showed correlations with CO in all stages, whereas WC showed correlations with RR and PETCO2 in each stage (Table 4).
The parameters related to an increase or decrease in CBF differed between the WC and LC conditions. First, CO was higher under WC than LC at each stage of exercise. Previous studies have reported a decrease in HR and increases in SV and CO due to water immersion (Christie et al. 1990; Garzon et al. 2015; Park et al. 1999); in the present study, both SV and CO were higher under WC than LC both at rest and during exercise. Additionally, HR tended to be lower under WC than LC, although not significantly lower. Thus, the participants exhibited physiological responses to water immersion in the present study. Nevertheless, the increase in CO during water immersion did not have a significant effect on the oxy-Hb concentration in the PFC. MAP tended to be higher in LC than in WC, but the difference was not significant. Also, ΔMAP and Δoxy-Hb showed no significant correlation. However, fluctuations in MAP during exercise have been reported to affect CBF (Smith and Ainslie 2017). Previous studies have also reported that light- and moderate-intensity exercise influenced a positive correlation between oxy-Hb and MAP (Tsubaki et al. 2016). Therefore, the changes in oxy-Hb of LC in this study may be more influenced by the MAP than the WC. At rest, PETCO2 increases during water immersion (Sackett et al. 2017). In the present study, RR did not differ between WC and LC, whereas PETCO2 was higher under WC than under LC at rest. The effect of water pressure likely caused spontaneous or voluntary hypoventilation, resulting in higher PETCO2. However, neither RR nor PETCO2 differed between the WC and LC conditions at the light-intensity stage of exercise; conversely, at the moderate-intensity stage of exercise, RR was higher under WC than LC, whereas PETCO2 was lower under WC than LC. Hyperventilation leads to lower PETCO2, and the increase in RR may have resulted in a plateau, if not a decrease, in PETCO2 that led to the observed reduction under WC (Pendergast et al. 2015). Ventilation has been suggested as a factor that affects CBF (Querido and Sheel 2007). Incremental increases in the partial pressure of arterial carbon dioxide (PaCO2) have been found to contribute to increased CBF by promoting cerebral vasodilation (Ide et al. 2003). PETCO2 is a useful parameter that can be measured noninvasively and reflects PaCO2 (Brothers et al. 2009). Increased ventilation during high-intensity exercise induces a decrease in PETCO2, which is suggested to be a contributor to decreased CBF (Nybo et al. 2002). Oyanagi et al. (2021) used a locomotor respiratory coupling system to intentionally increase ventilation and then examined the effects of low-intensity exercise under two conditions. They found that PETCO2 and oxy-Hb levels were lower under the increased ventilation condition than under the normal ventilation condition, suggesting that increased ventilation during exercise may be related to the reduction in PETCO2 and oxy-Hb levels. Under moderate- and high-intensity water-based exercise protocols, differences in RR and PETCO2 may occur earlier than under land-based exercise protocols, and CBF may be lower at an earlier stage in water-based exercise protocols than in land-based exercise protocols owing to the limitation on CBF caused by vasoconstriction. However, Pugh et al. (2015) reported that CBF during low-intensity stepping exercise was higher under water conditions than land conditions. Therefore, the advantages of water-based and land-based exercise might differ depending on the intensity of exercise. In the present study, CO was higher under WC than LC at all stages, whereas PETCO2 and RR were higher under LC with moderate-intensity exercise. Moreover, MAP was within the autoregulation range of CBF under both WC and LC and did not differ significantly between the conditions. Importantly, oxy-Hb levels did not differ under WC and LC in most CHs in the present study. Thus, we conclude that measuring only oxy-Hb levels, which reflect neural activity, cannot explain the factors or mechanisms that produce differences in CBF under WC and LC conditions.
Although the differences in oxy-Hb levels between WC and LC were not significant in most CH at each stage, CH7 showed a significant main effect for the exercise factor, with CH7 significantly higher under WC than LC. CH7 corresponds to the left-side DLPFC; as differences were found only in this region, we speculate that functional connections exist between the DLPFC and sensory and motor cortices. Anwar et al. (2016) reported that simple tapping movements make functional connections between the PFC and the sensory and motor cortices to execute the movement. Although the actions of cycling and finger tapping differ, and other factors such as force generation capacity and rhythm formation must be considered, It is thought that the movement is formed on the basis of these. In addition to this, water immersion and water-based exercise include stimulation caused by the pressure sensation from water pressure and temperature sensation from water temperature. Sato et al. (2012) reported an increase in oxy-Hb levels in the sensory and motor cortices during water immersion up to the femur. Dalecki and Bock (2013) reported that decreased muscle tone in the arm during water immersion reduces the intrinsic sensation during isometric tasks and the passive positioning of the arm in the water. It is not clear whether the activation of the motor cortex differs during water-based and land-based exercise, but we postulate that the external information associated with immersion affects the functional connections between the sensory, motor, and prefrontal cortices, leading to differences under WC and LC conditions. Furthermore, previous studies have shown that walking in complex environments on land (e.g., obstacle walking) and posture control result in higher PFC activity than in normal conditions (Mihara et al. 2016; Maidan et al 2018). Such complex walking has also been reported to be associated with executive and attentional functions (Clark 2015). Although the exercise performed in this study was bicycle exercise rather than walking exercise, water-based exercise may activate PFC more because the movement must be performed in a complex water environment with water resistance, water currents, and buoyancy.
We acknowledge that this study has limitations. First, the sample size of this study was smaller than the number of people detected using the G*Power software. This may have affected the test results of the statistics. Future studies should consider increasing the number of participants.
Second, the study was performed using only healthy young men; therefore, we cannot apply our findings to older populations. Third, the fNIRS was attached after the participant entered the water; thus, we were not able to survey the change in oxy-Hb concentration during the environment change from land to water, which might have affected oxy-Hb levels. In studies where differences in CBF and oxy-Hb levels were found owing to differences in environmental conditions, i.e., water vs. land, the participant entered an empty tank that was later injected with water. Hence, the oxy-Hb values under the WC condition in the present study may be underestimated. Forth, previous studies have suggested that NIRS signals are affected by changes in skin blood flow and that cerebral oxygenation dynamics measured by NIRS during exercise do not accurately reflect cerebral blood flow response and cerebral metabolism (Takahashi et al. 2011; Sorensen et al. 2012). In this study, skin blood flow was not measured, the oxy-Hb values may not accurately reflect the neural activity of the PFC. Therefore, future studies should use skin blood flow measurements to investigate this issue.
In conclusion, oxy-Hb levels increased as exercise intensity was increased under WC and LC conditions. However, the advantages of increased SV and CO associated with water immersion may not affect oxy-Hb levels in the PFC. Nevertheless, oxy-Hb concentrations were higher in the WC than in the LC in some regions. Thus, it is possible that differences in motor control exist that execute movements based on information transmitted from the sensory and motor cortices.
Data availability
All data generated or analyzed during this study are included in this published article.
References
Anwar AR, Muthalib M, Perrey S, Galka A, Granert O, Wolff S, Heute U, Deuschl G, Raethjen J, Muthuraman M (2016) Effective connectivity of cortical sensorimotor networks during finger movement tasks: a simultaneous fNIRS, fMRI, EEG study. Brain Topogr 29:645–660. https://doi.org/10.1007/s10548-016-0507-1
Brothers RM, Wingo JE, Hubing KA, Crandall CG (2009) The effects of reduced end-tidal carbon dioxide tension on cerebral blood flow during heat stress. J Physiol 587:3921–3297. https://doi.org/10.1113/jphysiol.2009.172023
Carter HH, Spence AL, Pugh CJ, Ainslie P, Naylor LH, Green DJ (2014) Cardiovascular responses to water immersion in humans: impact on cerebral perfusion. Am J Physiol Regul Integr Comp Physiol 306:R636–R640. https://doi.org/10.1152/ajpregu.00516.2013
Christie JL, Sheldahl LM, Tristani FE, Wann LS, Sagar KB, Levandoski SG, Ptacin MJ, Sobocinski KA, Morris RD (1990) Cardiovascular regulation during head-out water immersion exercise. J Appl Physiol 69:657–664. https://doi.org/10.1152/jappl
Clark DJ (2015) Automaticity of walking: functional significance, mechanisms, measurement and rehabilitation strategies. Front Hum Neurosci 9:246. https://doi.org/10.3389/fnhum.2015.00246
Cohen J (1992) A power primer. Psychol Bull 1:155–159. https://doi.org/10.1037//0033-2909.112.1.155
Dalecki M, Bock O (2013) Changed joint position sense and muscle activity in simulated weightlessness by water immersion. Aviat Space Environ Med 84:110–115. https://doi.org/10.3357/asem.3394.2013
Ekkekakis P, Parfitt G, Petruzzello SJ (2011) The pleasure and displeasure people feel when they exercise at different intensities: decennial update and progress towards a tripartite rationale for exercise intensity prescription. Sports Med 41:641–671. https://doi.org/10.2165/11590680-000000000-00000
Garzon M, Juneau M, Dupuy O, Nigam A, Bosquet L, Comtois A, Gayda M (2015) Cardiovascular and hemodynamic responses on dryland vs. immersed cycling. J Sci Med Sport 18:619–623. https://doi.org/10.1016/j.jsams.2014.08.005
Girouard H, Iadecola C (2006) Neurovascular coupling in the normal brain and in hypertension, stroke, and Alzheimer disease. J Appl Physiol 100:328–335. https://doi.org/10.1152/japplphysiol.00966.2005
Guadagni V, Drogos LL, Tyndall AV, Davenport MH, Anderson TJ, Eskes GA, Longman RS, Hill MD, Hogan DB, Poulin MJ (2020) Aerobic exercise improves cognition and cerebrovascular regulation in older adults. Neurology 94:e2245–e2257. https://doi.org/10.1212/WNL.0000000000009478
Hillman CH, Erickson KI, Kramer AF (2008) Be smart, exercise your heart: exercise effects on brain and cognition. Nat Rev Neurosci 9:58–65. https://doi.org/10.1038/nrn2298
Ide K, Eliasziw M, Poulin MJ (2003) Relationship between middle cerebral artery blood velocity and end-tidal PCO2 in the hypocapnic-hypercapnic range in humans. J Appl Physiol 95:129–137. https://doi.org/10.1152/japplphysiol.01186.2002
Maidan I, Shustak S, Sharon T, Bernad-Elazari H, Geffen N, Giladi N, Hausdorff JM, Mirelman A (2018) Prefrontal cortex activation during obstacle negotiation: what’s the effect size and timing? Brain Cogn 122:45–51. https://doi.org/10.1016/j.bandc.2018.02.006
Mihara M, Miyai I (2016) Review of functional near-infrared spectroscopy in neurorehabilitation. Neurophotonics 3:031414. https://doi.org/10.1117/1.NPh.3.3.031414
Nybo L, Møller K, Volianitis S, Nielsen B, Secher NH (2002) Effects of hyperthermia on cerebral blood flow and metabolism during prolonged exercise in humans. J Appl Physiol 93:58–64. https://doi.org/10.1152/japplphysiol.00049.2002
Oyanagi K, Tsubaki A (2021) Effects of increased respiratory rate on cortical oxygenated hemoglobin during low-intensity exercise. Respir Physiol Neurobiol 291:103691. https://doi.org/10.1016/j.resp.2021.103691
Park KS, Choi JK, Park YS (1999) Cardiovascular regulation during water immersion. Appl Human Sci 18:233–241. https://doi.org/10.2114/jpa.18.233
Paulson OB, Strandgaard S, Edvinsson L (1990) Cerebral autoregulation. Cerebrovasc Brain Metab Rev Summer 2:161–192
Pendergast DR, Moon RE, Krasney JJ, Held HE, Zamparo P (2015) Human physiology in an aquatic environment. Compr Physiol 20(5):1705–1750. https://doi.org/10.1002/cphy.c140018
Pugh CJ, Sprung VS, Ono K, Spence AL, Thijssen DH, Carter HH, Green DJ (2015) The effect of water immersion during exercise on cerebral blood flow. Med Sci Sports Exerc 47:299–306. https://doi.org/10.1249/MSS.0000000000000422
Querido JS, Sheel AW (2007) Regulation of cerebral blood flow during exercise. Sports Med 37:765–782. https://doi.org/10.2165/00007256-200737090-00002
Rooks CR, Thom NJ, McCully KK, Dishman RK (2010) Effects of incremental exercise on cerebral oxygenation measured by near-infrared spectroscopy: a systematic review. Prog Neurobiol 92:134–150. https://doi.org/10.1016/j.pneurobio.2010.06.002
Sackett JR, Schlader ZJ, Sarker S, Chapman CL, Johnson BD (2017) Peripheral chemosensitivity is not blunted during 2 h of thermoneutral head out water immersion in healthy men and women. Physiol Rep 5:e13472. https://doi.org/10.14814/phy2.13472
Sato D, Onishi H, Yamashiro K, Iwabe T, Shimoyama Y, Maruyama A (2012) Water immersion to the femur level affects cerebral cortical activity in humans: functional near-infrared spectroscopy study. Brain Topogr 25(2):220–227. https://doi.org/10.1007/s10548-011-0204-z
Smith KJ, Ainslie PN (2017) Regulation of cerebral blood flow and metabolism during exercise. Exp Physiol 102:1356–1371. https://doi.org/10.1113/EP086249
Sørensen H, Secher NH, Siebenmann C, Nielsen HB, Kohl-Bareis M, Lundby C, Rasmussen P (2012) Cutaneous vasoconstriction affects near-infrared spectroscopy determined cerebral oxygen saturation during administration of norepinephrine. Anesthesiology 117(2):263–270. https://doi.org/10.1097/ALN.0b013e3182605afe
Takahashi T, Takikawa Y, Kawagoe R, Shibuya S, Iwano T, Kitazawa S (2011) Influence of skin blood flow on near-infrared spectroscopy signals measured on the forehead during a verbal fluency task. NeuroImage 57:991–1002. https://doi.org/10.1016/j.neuroimage.2011.05.012
Tsubaki A, Takai H, Oyanagi K, Kojima S, Tokunaga Y, Miyaguchi S, Sugawara K, Sato D, Tamaki H, Onishi H (2016) Correlation between the cerebral oxyhaemoglobin signal and physiological signals during cycling exercise: a near-infrared spectroscopy study. Adv Exp Med Biol 923:159–166. https://doi.org/10.1007/978-3-319-38810-6_21
Voss MW, Heo S, Prakash RS, Erickson KI, Alves H, Chaddock L, Szabo AN, Mailey EL, Wójcicki TR, White SM, Gothe N, Mcauley E, Sutton BP, Kramer AF (2013) The influence of aerobic fitness on cerebral white matter integrity and cognitive function in older adults: results of a one-year exercise intervention. Hum Brain Mapp 34:2972–2985. https://doi.org/10.1002/hbm.22119
Zenko Z, Ekkekakis P, Ariely D (2016) Can you have your vigorous exercise and enjoy it too? Ramping intensity down increases postexercise, remembered, and forecasted pleasure. J Sport Exerc Psychol 38:149–159. https://doi.org/10.1123/jsep.2015-0286
Funding
This research was funded by the Japanese Society for the Promotion of Science (20K11303, KW).
Author information
Authors and Affiliations
Contributions
TH, DH, FM, TT, JS and KW conceptualized the study design. TH, DH, FM collected, and assembled the data, completed analysis and interpretation of data. TH drafted the manuscript. All authors have critically reviewed, revised and approved the manuscript. All authors have approved the study and manuscript, warrant that it is factual, have agreed to its submission, and have the right to publish.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest associated with this manuscript.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee of the University of Tsukuba (体020-184 and 19th April).
Consent to participate
Informed consent was obtained from all subjects involved in the study.
Additional information
Communicated by Matthew Heath.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hashitomi, T., Hoshi, D., Fukuie, M. et al. Differences in the prefrontal cortex responses of healthy young men performing either water-based or land-based exercise at light to moderate intensity. Exp Brain Res 241, 991–1000 (2023). https://doi.org/10.1007/s00221-023-06583-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00221-023-06583-z