
Abstract
The potential of enriched Pb (204Pb) was assessed to monitor pathways of trace levels of Pb in the pg range within the human body via isotope pattern variation in situations where natural lead cannot be used as a tracer due to regulatory limitations. Isotope ratio measurements were accomplished by means of (multi-collector) inductively coupled plasma mass spectrometry including a comparison of single and multi-collector ICP-MS for low-level 204Pb assessment. Isotopic pattern results from a blend of a large quantity of the element with a natural isotopic composition and an enriched stable isotope at orders of magnitude lower levels pose a nontrivial analytical problem. Isotope pattern deconvolution was successfully applied as mathematical tool based on multiple linear regressions. The method allowed for deconvolving the isotope pattern from measured isotope ratios without knowing the quantities of different isotope sources incorporated and mixed into the sample at levels of < 1 pg 204Pb/g blood. The objective of this manuscript is to evaluate and summarize the analytical aspects for Pb isotope pattern deconvolution based on the results of a clinical trial, where a 204Pb-enriched isotope tracer was applied to investigate the bioavailability of orally applied Pb along with purified clinoptilolite tuff as potential supplement. This unique approach allows to reduce tracer amounts to harmless levels to human health, which are in accordance with the legal regulative to study enrichment levels of < 0.01% in human blood.
Graphical abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Enriched stable isotopes provide an outstanding tool for tracer studies in living systems. In the past, radioactive isotopes were used for addressing questions related to the biology of metals and trace metals [1,2,3]. Radioisotopes can be used at ultra-low levels to trace the biological fate of elements. However, possible side effects caused by the radioactivity had to be taken into account [4]. Enriched spikes of naturally occurring non-radioactive isotopes have experienced increasing interest as monitors of metabolic processes in life sciences [5, 6]. Since these spikes are unique markers, they allow to monitor elemental uptake, distribution, deposition, or mobilization in living organism and to study the fate of materials applied for medical purposes. The advantages and challenges of introducing an isotopically enriched tracer into an organism are described in detail elsewhere [7,8,9].
A prerequisite of tracer-based studies is to minimize or preclude the possible negative impact (i.e. the toxicity) of tracers on the organism (in particular on human subjects). Thus, only very low molar amounts of tracer material ideally below any limits of toxicity are to be introduced into biological systems. The resulting challenge is to decrypt isotopic mixtures composed of the enriched stable tracer isotope and natural-abundance levels of the investigated element. Isotope pattern deconvolution (IPD) has been proven as method of choice in this context [8].
Any exposure to lead is considered to cause adverse health effects [10, 11]. Blood lead levels as low as 5 µg dL−1 (or about 50 ng g−1) are associated with increased risk of cardiovascular disease mortality [12]. Subtle neuropsychological impairment and headaches appear at blood lead levels of 25 µg dL−1 (or about 250 ng g−1). Blood lead levels exceeding 100 µg dL−1 (or about 1,000 ng g−1) are associated with an increased intracranial hypertension, encephalopathy with delirium and peripheral motor neuropathy [13]. Treatment of acute lead poisoning is based on administration of chelating agents, which reduce lead blood levels by forming chelator-lead complexes that are excreted in urine [14]. However, these drugs have serious side effects and require repeated courses of therapy. Thus, they are recommended only for patients with blood lead levels of greater than 45 µg dL−1 (450 ng g−1) [13, 15]. As a consequence, elimination of the source of lead exposure recommended as the single most effective way to prevent lead-induced adverse health effects [11]. The toxico-kinetics of lead are outlined in detail in Samekova et al. [16].
Contaminated water and food are the primary sources of lead exposure for the general population [17]. Lead in drinking water originates from the environment (natural and industrial sources) and/or lead containing water pipes [18]. Crops, fruits and vegetables can accumulate lead from (contaminated) soil in which they grow [10].
Clinoptilolite, a natural non-toxic mineral of the zeolite group, can be administered as preventive measure to bind lead with high selectivity and efficiency [19]. Due to its specific crystal structure and negative framework-charge, clinoptilolite acts as an active sorbent and ion-exchanger for free lead ions. In mice, which were exposed to elevated levels of lead (i.e. 50 mmol L−1) in their drinking water for 90 days, the concomitant administration of clinoptilolite reduced the accumulation of lead in the kidney and bones by about 90% and 70%, respectively [20]. These and related data [20,21,22,23,24,25,26,27,28,29,30,31,32] imply that clinoptilolite is potentially useful for reducing the amount of bioavailable heavy metals in people. It is worth pointing out, though, that people are exposed to submicromolar rather than millimolar levels of lead in their drinking water.
Accordingly, a clinical study was designed in accordance with Good Clinical Practice, the ISO 14155 [33] and the European Union Directive 98/63 EG [34] recommending an upper threshold of lead in drinking water of 10 µg L−1. The study aimed at the investigation of enteral lead uptake in healthy humans with concomitant oral intake of purified clinoptilolite-tuff (approved by the Food and Drug Administration for use as a dietary supplement with the brand name G-PUR®) [16]. Based on literature, the expected amounts of 204Pb tracer to be administered in blood and urine of human subjects required elaborated analytical measurement procedures and validation. This included the comprehensive assessment of blanks and of consumables used in the clinical study, sample preparation and the evaluation and comparison of methods based on single collector and multi collector inductively coupled plasma mass spectrometry for isotope ratio measurements. Isotope pattern deconvolution had to be adapted to allow for detection of ultra-low level enriched stable isotope tracers and for its successful application to a large sample set from a clinical trial.
Materials and methods
Note that chemical symbols were used according to the IUPAC Goldbook [35]
Preparatory laboratory work was performed in a class 100,000 clean room. Type I reagent-grade water (18 MΩ cm) (F + L GmbH, Vienna, Austria) was further purified by sub-boiling distillation (Milestone-MLS GmbH, Leutkirch, Germany). Analytical reagent-grade nitric acid (w = 65%, Merck-Millipore) was purified by double sub-boiling using a DST-1000 sub-boiling distillation system (AHF Analysentechnik, Tübingen, Germany). Polyethylene (PE) flasks, tubes and pipette tips (VWR International, Radnor, USA), as well as perfluoroalkoxy (PFA) screw cap vials (Savillex, Eden Prairie, USA) were pre-cleaned in a two-stage washing procedure using nitric acid (w = 10% and 1% respectively).
Certified reference material NIST SRM 981 (high purity lead metal, NIST, Gaithersburg, US) was used for Pb isotopic analysis to optimize instrument parameters as well as for calibration of instrumental isotopic fractionation (IIF). Solutions of this standard were prepared gravimetrically in nitric acid (w = 2%) and diluted to final mass fraction of w = 50–100 ng g−1 as isotopic reference for standard-sample bracketing (SSB) to correct for IIF.
Blank assessment of materials used in clinical study and in lab
Mineral water (Vöslauer Still®): tracer vector
Commercially available 500 mL bottles (n = 5) of Vöslauer Still® (Vöslauer, Vienna, Austria) water were opened using a commercially available, pre-cleaned crown cork opener, and 10 mL of water was transferred directly into pre-cleaned test tubes. For the measurement using ICP-MS, the solutions were acidified with HNO3 (w = 65%, 2 × subboiled) in order to obtain a HNO3 solution of w = 2%. A triplicate determination was carried out for each bottle.
Crown corks for re-sealing of bottles
Crown corks were covered with reagent grade type I H2O in pre-cleaned plastic containers and leached out overnight. After leaching, the solution was acidified for the measurement.
Medical test tubes and needles
Different commercially available test tubes dedicated to sampling of blood during the clinical trial were leached with 4 mL HNO3 (w = 2%) (prepared from HNO3 (w = 65%, 2 × subboiled and ultrapure water, 1 × subboiled) for 24 h. This solution was measured directly with ICP-MS. The necessary sample preparation and leaching steps were adapted according to the material. Needles were placed in water overnight or leached directly by pressing the solution through using pre-cleaned syringes. The tube types tested included routinely used Vacuette tubes (Greiner Bio-One, purple K3EDTA (Ref. 454217); green (lithium heparin) (Ref. 454217); green (lithium heparin) Ref. 455084; blue (9NC Coagulation sodium citrate 3.2%) (Ref. 454332); grey (FE Sodium Fluoride/K3EDTA) (Ref. 454033); yellow (Z Urine No Additive) (Ref. 455028)); Safety Blood Collection Greiner Bio-One; VASOFIX SAFETY PUR 18G (Braun); and BD Venflon Pro Safety 20G (Beckton Dickinson Infusion Therapy).
Lead isotope tracer
The 2.5 μg dose of 204Pb was prepared by solving 11.74 mg of 99.94% atom-enriched metal 204Pb in 5.0 mL of w = 15% nitric acid and further diluting it with ultrapure water to a final lead mass concentration of 2681 μg L−1 for spiking bottled water.
Experimental design using certified reference materials of blood
Blood was the primary target matrix in the clinical study. Thus, preliminary laboratory spiking experiments using matrix-matched blood certified reference materials and the 204Pb tracer were carried out. Therefore, we used blood certified reference material quantities, which were in accordance with the planned human study. This allowed to characterize the expected degree of enrichment and develop the analytical measurement procedure accordingly.
Three different blood certified reference materials were available for the experiments: BCR-634 (γ(Pb) = 46 μg L−1), BCR-635 (γ(Pb) = 210 μg L−1) and BCR-636 (γ(Pb) = 520 μg L−1). The lead isotope tracer solution of the dissolved 204Pb Spike-Tracer was used for spiking after further dilution to γ (204Pb) = 1 µg L−1. For the spike experiment, 10 mixtures of blood and tracer and 10 blanks with microwave digestion were produced and, after dilution, measured using ICP-MS. BCR-636 (γ(Pb) = 520 μg L−1) was chosen for the spike tests. The high Pb concentration allowed a large number of parallel experiments from the same starting material. Relative enrichment levels in the range from 0.01 to 0.50% were analysed, beside blank digests. The levels were chosen accordingly in order to determine the limitations of the method (i.e. 204Pb minimum amount that is necessary to monitor a significant change in the Pb isotopic composition).
A final volume of 1 mL was selected for each mixture prepared for digestion. A volume of the diluted tracer solution (γ(204Pb) = 1 µg L−1, V ranging from 10 to 520 µL) was added to a volume of 200 μL blood (BCR-636) (m(Pbnat) = 104 ng) and then filled up to 1000 μL with HNO3 (w = 2%). After a reaction time of 10 min, 4 mL HNO3 (w = 65%, 2 × subb.) and 0.5 mL H2O2 were added as digestion reagents. After the addition of HNO3, the solution was shaken, and the cap of the reagent tube was opened 2–3 times in order to allow gases to be released to reduce the pressure in the vessel.
Subsequently, mixtures of BCR-636 and 204Pb-traver were digested by means of microwave pressure digestion (Multiwave Pro, Anton Paar GmbH, Graz, Austria) in a 48MF50 rotor, using pre-cleaned vessels. The microwave program was ramped up at 1400 W for 15 min and then held at power for 20 min before being cooled for 15 min. The Pb isotope ratio measurements of mixtures of BCR-636 and 204Pb tracer were performed using multi-collector inductively coupled plasma mass spectrometry (MC ICP-MS) on a Nu Plasma HR (NP048) (Nu Instruments, Wrexham, UK). See the “Measurement procedures based on ICP-MS” section for details on Pb isotope ratio measurements by MC ICP-MS.
Clinical trial
This trial was conducted as a medical device clinical trial according to the regulatory provisions in Austria. Glock Health, Science and Research GmbH acted as sponsor of this single centre study. The study protocol was approved by the Ethics Committee of the Medical University of Vienna (no. 1285/2019) and the Austrian Federal Office for Safety in Health Care (BASG) and is registered at clinicaltrials.gov (NCT04138693). This study was conducted at the Department of Clinical Pharmacology at the Medical University of Vienna in accordance with the Declaration of Helsinki. All study participants provided written informed consent before any study-specific procedures were performed. The study was initiated on 28th of August 2019 and the clinical phase completed on the 12th of February 2020. The study followed a randomized, placebo controlled, double-blind, parallel-group design. Male or female healthy volunteers aged 18–45 years with a body mass index (BMI) of 19–27 kg/m2 for males and 17–25 kg/m2 for females were eligible for participation. Main inclusion criteria were whole blood lead concentration < 40 μg/L as measured by graphite furnace atomic absorption spectroscopy, serum ferritin concentration within the sex-specific normal range and 1 month of stable eating habits. Key exclusion criteria were pregnancy or breastfeeding in women, regular use of medication or iron supplements in the previous 2 months, any relevant organ disease, especially gastrointestinal pathology, recent diarrhoea, diabetes, symptomatic food allergies or aluminium and/or silicon hypersensitivity. Participants were excluded, if they showed any clinically relevant laboratory abnormalities at screening, or alcohol, nicotine or drug abuse.
The investigational medical device (IMD) investigated in this study consisted of purified clinoptilolite-tuff (product name is G-PUR®). The raw material of the product originated from a large quarry in Eastern Slovakia and was refined with a technically sophisticated and fully quality-controlled production process. The patented purification process results in removal of natural bioavailable impurities to meet highest safety standards and regulatory requirements. For details about the clinoptilolite-tuff characteristics and source, see [36, 37].
The major component of the product is clinoptilolite, a natural non-toxic mineral of the zeolite group that due to its specific crystal structure and negative framework-charge, and acts as an active sorbent and ion-exchanger, capable of binding lead (among other heavy metals) with high selectivity and efficacy [19]. When orally ingested, the IMD remains inside the digestive tract and is eliminated via the stool. As the IMD is stable even in an acid pH environment, there is no major degradation of the structure.
In short, in this clinical investigation, healthy volunteers received 250 mL drinking water spiked with stable lead isotope 204Pb in a concentration of 10 µg L−1; no harm to the trial subjects was expected with the dose applied as kept below the Austrian drinking water regulation [38]. Overall, 42 subjects were enrolled and randomized in three groups, who received in addition to 204Pb spiked drinking water, 4.0 g G-PUR®, 2.0 g G-PUR® and placebo (no addition to water) (note that the numbers of subjects follow the numbers of recruitment; subjects not meeting the requirements of the trial, e.g. due to elevated Pb levels in blood, were excluded in the study). Blood samples for assessment of blood lead levels and the lead isotopes were taken at baseline (t = 0 h) and at specific timepoints of 4 h, 8 h, 12 h, 24 h, 48 h and 192 h after tracer administration. Urine was sampled at baseline and during the first 24 h after tracer administration. The clinical trial was carried out in two stages with 6 subjects in stage 1 sampled at more times as compared to stage 2 (36 subjects). Details about the clinical trial can be found in Samekova et al. [16].
Preparation of 204Pb enriched water for drinking
As the final dilution of 204Pb in mineral water was discovered to be only semi-stable (precipitation of PbCO3 and other insoluble Pb compounds may occur over time), the final dilution step was performed on-site, adding 925 μL of spiking solution to the 250 mL “Vöslauer Still®” glass bottles resulting in a final concentration of 10.0 μg L−1. After an overnight stay at the study site, all subjects received 2.5 μg 204Pb in 250 mL of mineral water (spiked 250 mL “Vöslauer Still®” in glass bottles). Subjects drank the bottle content using a straw; the exact amount of fluid/204Pb intake was assessed by weighing the spiked “Vöslauer Still®” glass bottles (straw included) before and after drinking. The concentration of 204Pb administered to the subjects did not exceed the maximum levels listed in the drinking water ordinance for Pb concentration [38]. The same applied for the nitrate concentration and pH of the final solution (0.67 mg L−1 nitrate, pH > 6.5 due to the buffering capacity of the mineral water).
Sample preparation (clinical trial)
Blood sample digestion
Blood samples were pre-digested at the study site. 3.5 mL HNO3 (w = 65%, 1 × subb.) was added to 500 μL blood. The solutions were transferred under controlled conditions from the study site to the laboratories of Montanuniversität Leoben for further processing. Prior to digestion of the samples, purification digestion runs with HNO3 were performed. 0.5 mL H2O2 was added to pre-digested blood samples (500 μL blood + 3500 μL HNO3). After a reaction time of 10 min, the digestions of blood samples were performed by microwave pressure digestion (see details above). Samples were further diluted using ultrapure water or diluted nitric acid.
Urine sample digestion
Urine samples were stabilized at the study site by adding HNO3 (6 mol L−1) depending on the urine volume sampled aiming for w (HNO3) = 3–7%. The solutions were transferred from the study site to the laboratories of Montanuniversität Leoben under controlled conditions for further processing. Acidified urine samples were digested using 3.5 mL HNO3 (w = 65%, 2 × subb.) and 0.5 mL H2O2. The digestion of urine samples was performed by microwave pressure digestion (see details above). Samples were further diluted using ultrapure water or diluted nitric acid. Further treatment was done following the same procedures as for blood samples after digestion.
Blood sample preparation of real samples for MC ICP-MS measurements
Based on the results of the quantification by ICP-QMS of real blood samples and the expected sensitivity of the MC ICP-MS method, 4 mL of selected blood sample digest (subject-01 and subject-02) was evaporated to almost dryness on a hot-plate at 120 °C (note: the set temperature T does not equal T in the vessel; T was kept below boiling point of the sample solution to avoid boiling retardation) in 2 × pre-cleaned PFA vessels. This way, the samples reached a total amount of Pb ranging from 1 to 2 ng to allow measurements by MC ICP-MS using Faraday cups as detectors. The evaporated samples were re-dissolved in 1 mL HNO3 (w = 2%) for the MC ICP-MS measurement.
All seven blood digests (7 time points) of subject-01 and subject-02 were measured by MC ICP-MS. Due to the low Pb levels present in the blood samples, this pre-concentration step was required, leading to increased matrix load during the measurement. The matrix caused the sample introduction system (Aridus II, Teledyne Cetac, Omaha, USA) to clog, eventually resulting in a total loss of signal. Thus, measurements of the entire sample batch were carried out using ICP-QMS and introducing a wet aerosol.
Measurement procedures based on ICP-MS
Elemental analysis was performed on selected samples for quantification of analyte and matrix elements for validation purposes. Details are provided in the Supporting information SI Elemental analysis by ICP-MS.
Pb isotopic compositions of mixtures of BCR-636 and 204Pb tracer and blood of selected subjects were analysed to compare the performance of ICP-QMS to MC ICP-MS. ICP-QMS and MC ICP-MS were compared to determine the optimum measurement protocol for Pb isotope ratio measurements of low-level Pb in a blood matrix. The two setups available differ in their performance regarding Pb analysis primarily by sensitivity, with the ICP-QMS system being more sensitive than MC ICP-MS when Faraday cups are being used as detectors. In contrast, MC ICP-MS stands out because of its high-precision capabilities, given that a decent amount of analyte is present.
A single collector ICP-QMS instrument (NexION 2000, PerkinElmer, Ontario, Canada) equipped with a FAST introduction system and a multi collector ICP-MS (Nu Plasma HR, Nu Instruments) equipped with a desolvation nebulization membrane unit (Aridus II, Cetac) in combination with a PFA nebulizer (Microflow ST Nebulizer, Elemental Scientific, Omaha, USA) as sample introduction system were used. The ICP-QMS instrument was operated using the quantitative method option by Syngistix software. Measurements of isotopes 202Hg (20 ms), 204Pb (75 ms), 206Pb (20 ms), 207Pb (20 ms), 208Pb (20 ms) and 115In (20 ms) were performed with dwell times given in parenthesis and a total measurement time of ca. 3 min (1 sweep, 1 reading, 900 replicates), allowing the simultaneous Pb quantification and Pb isotope ratio analysis. The number of replicates was chosen to optimize the precision for determining the 20xPb/204Pb isotope ratio.
The MC ICP-MS was operated in low mass resolution and static mode allowing for the simultaneous measurement of all natural stable Pb isotopes, as well as of 202Hg for monitoring the mercury background in the samples to correct a possible isobaric interference from 204Hg to 204Pb (see collector block configuration in Table S01). Data collection was accomplished in 6 blocks of 10 measurements with an integration time of 10 s, resulting in a total of 60 measurements per sample. The samples and the isotopic standards NIST SRM 981 were introduced into the plasma in the following sequence: standardSSB1-SRM981—sample – standardSSB2-SRM981, to enable correction for time-dependent instrumental isotopic fractionation (IIF) via classical sample standard bracketing (SSB). Concentrations of sample and SSB standard were matched within 10% [39, 40].
The final results of isotope ratio measurements are expressed as molar fractions (corresponding to an enrichment of 204Pb in the lead isotopic composition). A normalization to BMI (body mass index) and hematocrit was required for data obtained from blood samples to account for inter-subject variability. Normalization of the molar fraction of 204Pb tracer in urine was normalized to creatinine was also performed. In summary, 204Pb tracer enrichment factors assessed by mass spectrometric analysis and IPD were normalized by division with a correction factor calculated from BMI/hematocrit and from creatinine levels for data from blood and urine samples, respectively.
Data processing
The Pb isotope data are given both in absolute notation as 208Pb/204Pb and in relative isotope notation with NIST SRM 981 acting as zero-anchor on the relative (= delta) scale. The actual enrichment in the samples due to the addition of the 204Pb tracer was calculated using isotope pattern deconvolution (IPD). This chemometric method is based on multiple linear regressions with assignment of the proportions of total lead to known end members of the mixture for the final isotopic composition in the sample (see equations below) [8].
Data processing: MC ICP-MS
-
1.
Blank correction was performed using the measure zero—method provided by the instrument software automatically on-peak by subtracting the raw intensity of the analytical blank (calibration blank, w = 2% HNO3) from the raw intensity of each individual sample.
-
2.
Outliers were removed on-the-run based on a 2SD-test (95% confidence interval) in the software.
-
3.
Corrections for isobaric interferences: A correction approach referred to as “peak stripping” was applied to check for the impact of remaining Hg in the samples on the final Pb isotope ratio. This strategy was also applied to correct 204Pb+ for minor interferences of 204Hg+ arising from residual Hg (< 0.02%, expressed as relative ratio of int(202Hg)/int(208Pb)) in the purified sample solutions. Here, the simultaneously measured 202Hg (int(202Hg)spl) signal and the IUPAC/CIAAW value for n(204Hg)/n(202Hg)nat (= 0.2293) [41], which was corrected for IIF via SSB with NIST SRM 981 of calculated isotopic compositions (n(206Pb)/n(204Pb)cert = 16.937) [42], assuming the same IIF for n(206Pb)/n(204Pb)spl and n(204Hg)/n(202Hg)spl, were used to calculate the 204Pb (int(204Pb)spl), according to Eqs. 1a–c:
$${int\left({}^{204}Pb\right)}_{spl}={int(204)}_{spl}-{int({}^{202}Hg)}_{spl}\bullet {\left(\frac{n\left({}^{204}Hg\right)}{n\left({}^{202}Hg\right)}\right)}_{nat}\bullet {\left(\frac{M\left({}^{204}Hg\right)}{M\left({}^{202}Hg\right)}\right)}^{f}$$(1a)$$f=\frac{{f}_{{SSB}_{1}}+{f}_{{SSB}_{2}}}{2}$$(1b)$${f}_{SSB}=\mathrm{ln}\left(\frac{{\left(\frac{n({}^{206}Pb)}{n({}^{204}Pb)}\right)}_{cert}}{{\left(\frac{n({}^{206}Pb)}{n({}^{204}Pb)}\right)}_{SSB}}\right)/\mathrm{ln}\left(\frac{M\left({}^{206}Pb\right)}{M\left({}^{204}Pb\right)}\right)$$(1c)where all intensities correspond to blank corrected beam intensities, int(206Pb)/int(204Pb)SSB was the measured raw ratio in the SSB standard, and M(X) were the atomic weights extracted from the IUPAC/CIAAW tables [41]. This correction was considered insignificant for real blood and urine samples and only applied during method optimization.
-
4.
Blank corrected, averaged isotope ratios of 204Pb/208Pb, 206Pb/208Pb and 207Pb/208Pb were corrected for IIF by classical SSB using the isotope reference materials NIST SRM 981 (natural Pb). The NIST SRM 981 solutions (w(Pb) = 1 ng g−1) measured before and after a sample were used for IIF correction. Correction factors were calculated for each isotope ratio, respectively (f(204Pb/208Pb), f(206Pb/208Pb) and f(207Pb/208Pb)) and applied to correct the blank corrected, averaged isotope ratios of 204Pb/208Pb, 206Pb/208Pb and 207Pb/208Pb.
-
5.
Blank and IIF corrected Pb isotope ratios followed isotope pattern deconvolution (IPD) to deconvolute the enrichment of 204Pb administration following equations Eqs. 2a and 2b. The isotopic composition of the 204Pb tracer (as provided in the certificate of the manufacturer) was taken as Pb source (= end-member) 1. The Pb isotopic abundances as determined in blood sample “BL” (corresponding to t = 0 before administration of the Pb-tracer) were taken as Pb source 2 providing the reference isotopic composition before artificial adulteration of the Pb isotopic composition in each individual. (Note: the natural Pb isotopic composition in human blood varies significantly between individuals. Thus, tabulated representative values for the natural Pb isotopic abundances cannot be used as sources/end-members in the IPD.) As there are more parameters (isotopic abundances) than unknowns (molar amounts of two sources) in the equation system, an error vector is included. (Note: a total of 4 sources of different Pb isotopic composition could be treated in the equation; in this study, only two sources were present: source 1: natural Pb; source 1: enriched 204Pb tracer.)
$${A}_{s}^{i}=\frac{{R}_{i}}{{\sum }_{i=1}^{n}{R}_{i}}$$(2a)$$\left[\begin{array}{c}{A}_{s}^{204}\\ {A}_{s}^{206}\\ \begin{array}{c}{A}_{s}^{207}\\ {A}_{s}^{208}\end{array}\end{array}\right]=\left[\begin{array}{c}{A}_{source 1}^{204}\\ {A}_{source 1}^{206}\\ \begin{array}{c}{A}_{source 1}^{207}\\ {A}_{source 1}^{208}\end{array}\end{array}\right]\left[\begin{array}{c}{A}_{source 2}^{204}\\ {A}_{source 2}^{206}\\ \begin{array}{c}{A}_{source 2}^{207}\\ {A}_{source 2}^{208}\end{array}\end{array}\right]\left[\begin{array}{c}{A}_{source 3}^{204}\\ {A}_{source 3}^{206}\\ \begin{array}{c}{A}_{source 3}^{207}\\ {A}_{source 3}^{208}\end{array}\end{array}\right]\left[\begin{array}{c}{A}_{source 4}^{204}\\ {A}_{source 4}^{206}\\ \begin{array}{c}{A}_{source 4}^{207}\\ {A}_{source 4}^{208}\end{array}\end{array}\right]\cdot \left[\begin{array}{c}{x}_{source 1}\\ {x}_{source 2}\\ \begin{array}{c}{x}_{source 3}\\ {x}_{source 4}\end{array}\end{array}\right]+\left[\begin{array}{c}{e}^{204}\\ {e}^{206}\\ \begin{array}{c}{e}^{207}\\ {e}^{208}\end{array}\end{array}\right]$$(2b) -
6.
The molar fraction (in %), indicating the amount of 204Pb tracer (x(204Pb)) contributing to the total amount of Pb in blood as result of the IPD, was further normalized using HCT and BMI as provided by the study site. x(204Pb) was divided by the factor (HCT/BMI) for normalization, resulting in x-norm(204Pb). The average HCT (from two different measurements performed at the study site) was used. In case of urine, data were normalized to creatinine levels.
Data processing: ICP-QMS
Data was processed offline in Microsoft Excel® spreadsheet according to the following procedure point-by-point prior to averaging data.
-
1.
Blank correction at each m/z was performed automatically by the Syngistix software by subtracting the raw intensity of the analytical blank (calibration blank, w = 2% HNO3) from the raw intensity of each individual sample.
-
2.
As outlined above, no correction of the signal at m/z = 204 for 204Hg was necessary as Hg background could be considered negligible.
-
3.
Blank corrected ratios of 204Pb/208Pb, 206Pb/208Pb and 207Pb/208Pb were calculated point-by-point, and the average and standard deviation of 9 blocks of 100 measurements were calculated. (Measurement statistics have previously been optimized to reach best precision for 204Pb/208Pb, 206Pb/208Pb and 207Pb/208Pb.)
-
4.
IIF correction followed the similar procedure as described in detail for MC ICP-MS measurements.
-
5.
IPD calculations following the exact same procedure as for MC ICP-MS measurements were performed.
-
6.
x-norm(204Pb) was calculated as described above for MC ICP-MS measurements.
-
7.
In addition, δ-values (in \(\permille\) for Pb isotope ratios were calculated relative to the average isotopic ratio of the used reference standard (NIST SRM 981) from the SSB in accordance with Eq. 3:
$$\begin{array}{cc}\delta{\left({}^iPb/{}^{204}Pb\right)}_{SRM981}=\left(\frac{R_{spl}-R_{SRM981}}{R_{SRM981}}\right)&\lbrack\permille\rbrack\end{array}$$(3)
- δ:
-
delta value
- i Pb :
-
isotopes 206, 207 or 208 of Pb
- R :
-
isotope ratio of the sample (spl) or the standard (SRM981) after blank and interference correction of a specific iPb/204Pb ratio
Uncertainty calculations
The total combined uncertainty budget for Pb isotopic analysis was calculated using a simplified Kragten approach according to established protocols in our laboratory [39, 40, 43]. The precision of the measured isotope ratio of the sample and of the standards, as well as the within-run-repeatability of the measured isotope ratio in the bracketing standards as proxy for instrument stability, was taken into account as main contributors to the uncertainty.
The uncertainty of the x-norm(204Pb) was calculated by combining the total measurement uncertainty of the determination of 204Pb molar fraction and the total analytical error of HCT (u = 10%) as provided by the responsible laboratory [44].
Results and discussion
Blank levels of consumables and tracer vector
The total amount of Pb leached from consumables routinely used for blood sampling was compared to the detection and determination limits of the method. This showed that most materials did not contain significant amounts of leachable Pb. LOD (γ(Pb) = 0.013 µg L−1) and LOQ (γ(Pb) = 0.044 µg L−1) were determined using the analytical blank values (pure HNO3 (w = 2%) used for leaching experiments) via three or ten times the standard deviation of 10 repeated measurements of the analytical blank value from individually prepared solutions over the measurement sequence. Only measured values that were above the LOQ of the measurement were further processed. The examined materials showed no significant amounts of natural Pb especially considering the expected natural Pb levels in human blood as well as 204Pb tracer to be administered.
Only one material (Vacuette purple) showed leachable Pb levels above LOQ with γ(Pb) = 0.284 µg L−1. One product (Vacuette blue) showed increased levels of alkali and alkaline earth elements, which possibly originated from the internal heparin solutions contained. Based on the results of the leaching experiment, tubes “Vacuette green” were chosen for blood sampling during the clinical trial in order to avoid any cross contamination. Crown corks showed leached Pb amounts < LOD. The tracer vector mineral water (Vöslauer Still®) had Pb levels < LOD, as well.
To monitor the digestion blanks, 10 digestion blanks were processed. The lead background, measured on the raw signal of 208Pb in the digestion solutions diluted analogously to the measurement solutions, was 0.016 ng g−1 ± 0.005 ng g−1 Pb, thus considered insignificant.
Blood CRM spiking experiments with 204Pb tracer
The calculation of the absolute Pb isotope ratios (in the following the 208Pb/204Pb isotope ratio is used) and the enrichment (based on IPD) was carried out via external calibration using an isotope-certified standard reference material. In addition, the influence of traces of mercury was estimated by measuring the signal of 202Hg.
Results of the spiking experiment shown in Table 1 show a significant shift in the 208Pb/204Pb isotopic composition already at a 204Pb enrichment level of 0.01% based on IPD. No significant effect was detected based on possible contribution of traces of Hg in the sample, and thus, Hg correction was considered insignificant for further analysis.
Figure 1 shows the molar fraction of 204Pb calculated based on IPD vs the absolute 208Pb/204Pb ratio.

Molar fraction of 204Pb tracer calculated by IPD vs. measured 208Pb/204Pb ratio. The theoretical enrichment levels from experimental design are compared to the actual measured enrichment levels assessed from spiking experiments using BCR-636 spiked with increasing amounts of 204Pb tracer solution
The theoretically calculated change in isotopic composition corresponds very well with the signature achieved in the spike experiments. The natural Pb isotopic composition in the blood based on tabulated values deviates from the estimated calculated values, albeit, not significantly. As a consequence, the true natural Pb isotopic composition was determined for each blood sample from the clinical trial and used as end member for IPD calculations. In the expected degree of enrichment of 0.15% with an administration of 204Pb at the limit of the drinking water ordinance of 10 μg L−1 in 250 mL Vöslauer mineral water, a shift in the 208Pb/204Pb ratio from 38.25 to 34.50 was to be expected. This corresponds to a relative change of approx. 9–10%. The average total measurement uncertainty (both for MC ICP-MS and ICP-QMS measurements) of the 208Pb/204Pb was approx. 0.06% with a measurement signal of 204Pb > 0.004 mV. Accordingly, the bias to be expected in the human experiments was significant with regard to the measurement uncertainty. In conclusion, the method including the data processing based on IPD was considered valid for the carrying out the clinical trial using the protocol outlined above.
Comparison of MC ICP-MS and ICP-QMS for Pb isotope ratio assessment in real blood and urine samples
Pb isotope ratio data and enrichment based on 204Pb administration was obtained in blood of 2 subjects (subject-01 and subject-02) by both MC ICP-MS and ICP-QMS for comparison of instrument performance at low levels of Pb.
Data obtained by MC ICP-MS and ICP-QMS were compared for subject-01 and subject-02 (see Tables 2 and 3).
Figure 2a and b shows the molar fraction of 204Pb contributing to the total Pb in each sample of subject-01 obtained by IPD including a comparison of data obtained by MC ICP-MS and ICP-QMS. Figure 3a and b shows the molar fraction of 204Pb contributing to the total Pb in each sample of subject-02 obtained by IPD including a comparison of data obtained by MC ICP-MS and ICP-QMS. Uncertainties plotted in Figs. 2b and 3b correspond to combined uncertainties taking into account the measurement of 204Pb (RSD = 3%) and the total analytical error of HCT determination (u = 10%).

a (left) Molar fraction of 204Pb tracer by IPD of subject-01 vs sampling time after administration of tracer; error bars represent 1SD of the measurement. b (right) Molar fraction of 204Pb tracer normalized for HCT/BMI by IPD of subject-01 vs sampling time; error bars represent combined uncertainties u (k = 1) of the normalized molar fraction

a (left) Molar fraction of 204Pb tracer by IPD of subject-02 vs sampling time after administration of tracer; error bars represent 1SD of the measurement. b (right) Molar fraction of 204Pb tracer normalized for HCT/BMI by IPD of subject-02 vs sampling time; error bars represent combined uncertainties u (k = 1) of the normalized molar fraction
Molar fractions (in x(204Pb) %; representing the amount of Pb originating from the 204Pb tracer) show similar kinetic curves for subject-01 and subject-02 even though the degree of enrichment differs significantly between the subjects. Data obtained by ICP-QMS and MC ICP-MS do not differ significantly taking into account the combined measurement uncertainty. The combined uncertainty budget considered the precision of the single measurement and the total analytical error of HCT determination. A possible uncertainty of the BMI to the total uncertainty of the final result was considered insignificant and thus not propagated.
The accuracy (considering uncertainty and trueness) for ICP-QMS and MC ICP-MS is considered equal. This can be explained by the very low analyte concentrations in the measurement solutions as a result of the low Pb mass fraction in the original samples. MC ICP-MS would usually be considered the method of choice for isotope-ratio analysis based on the improved precisions that can be obtained for isotope ratio analysis given that ideal measurement conditions are met. However, the ICP-QMS setup tested in this study represented the more sensitive method for measuring low concentrations. In this particular case, total Pb levels were assessed in the low ng g−1 to pg g−1 range. (Note: the natural 204Pb abundance is about 1.4%.) In case of MC ICP-MS measurements, 204Pb was assessed at signal intensities of ca. 0.001 V, resulting in decreased measurement precision by 3–4 orders of magnitude as compared to ideal conditions. In addition, the routine sample introduction system (desolvation membrane Aridus II) of MC ICP-MS, which achieves high sensitivity, cannot be used with pre-concentrated blood and urine samples due to the present high salt concentrations. It is possible to subject samples to a purification step as usually performed with samples of high ng g−1 to μg g−1 Pb levels. This was however not considered because conventional purification procedures use significant amounts of purification solutions that potentially carry the analyte in ultra-traces as well. In this case, the purification would significantly increase the Pb background levels in the purified sample solution. Subsequently, the measurements to determine enrichment of 204Pb administration in blood and urine were performed by ICP-QMS as robust and reliable method for all subjects.
Measurement method by ICP-QMS: blood matrix
The Pb mass fraction w(Pb) of the measurement solutions of blood digests (dilution of the digestion solution by a factor of 4) ranged from 0.052 to 0.538 ng g−1 (this corresponds to w(204Pb) = 0.73 to 7.53 pg g−1). The detected (blank corrected) signal intensities of 208Pb and 204Pb were < 300 counts and < 50 counts, respectively. The average LOD of the analytical measurement was 4.0 pg g−1 (for total Pb) corresponding to 0.02 pg g−1 204Pb.
Method blanks showed raw signal intensities of 208Pb and 204Pb of < 80 counts and < 10 counts, respectively, resulting in Pb mass fractions ranging from w(Pb) = 0.010 ng g−1 to 0.020 ng g−1 (w(204Pb) = 0.00014 ng g−1 to 0.00028 ng g−1) in the method blank solutions. The resulting LOD of the method for total Pb determination in blood was w(Pb) = 0.09 ng g−1. The resulting LOD of the method for 204Pb determination in blood was w(204Pb) = 0.001 ng g−1.
BCR-634 (γ(Pb) = 46.0 µg L−1 ± 5.0 µg L−1 (U)) and BCR-635 (γ(Pb) = 210.0 µg L−1 ± 24.0 µg L−1 (U)) (Pb in blood) were processed in replicates along with blood samples. The two materials were chosen based on the certified Pb levels. The average γ(Pb) in BCR-634 and BCR-635 determined was 48.0 µg L−1 ± 19.0 µg L−1 (n = 21; 2SD) and 208.2 µg L−1 ± 57.3 µg L−1 (n = 22; 2SD). Pb concentrations determined in BCR-634 and BCR-635 processed during blood sample preparation overlap within uncertainties with the certified values.
Measurement method by ICP-QMS: urine matrix
The mass fraction of natural Pb in the measurement solutions of urine digests (dilution by a factor of 4 from the original digestion solution) in ICP-QMS ranged from 0.010 to 0.030 µg L−1 (this corresponds to γ(204Pb) = 0.00014 to 0.00042 µg L−1). The detected (blank corrected) signal intensities of 208Pb and 204Pb were < 70 counts and < 10 counts, respectively. Method blanks showed raw signal intensities for 208Pb and 204Pb of < 17 counts and < 0.2 counts, respectively, resulting in an average Pb mass fraction c(Pb) = 0.009 µg L−1 (γ(204Pb) = 0.00013 µg L−1) in the method blank solutions. The LOD of the method for 204Pb tracer determination in urine is γ(204Pb) = 0.001 µg L−1.
Seronorm Trace Elements Urine L-1 (certified γ(Pb) = 0.72 µg L−1 ± 0.36 µg L−1 (as indicative U) was processed in replicates along with urine samples. The average β(Pb) in Seronorm Trace Elements Urine L-1 determined was 1.75 µg L−1 ± 1.25 µg L−1 (n = 18; 2SD). Pb concentrations determined in Seronorm L-1 processed during urine sample preparation overlap within uncertainties with the certified values. The relative standard deviation of a measurement was about 30% as a result of the substantial low signal intensities (I(208Pb) ranging from 40 to 60 counts). Pb concentrations were corrected for the procedural blank (= method blank from microwave digestion).
Results from blood samples of all subjects from the clinical trial
The total amount of Pb and the enrichment of 204Pb by the administered tracer were normalized to HCT and BMI—values for each individual. Table S03 summarizes all data obtained in blood samples of 42 subjects (investigated in a two-stage approach: stage 1 (6 subjects) and stage 2 (36 subjects)) (note: sampling time was adjusted based on actual sampling times for each individual and rounded to an hour). The natural Pb content in the blood of the examined subjects ranged from 4.3 to 52.1 µg L−1 with an average of 16.1 µg L−1 ± 9.7 µg L−1 (1 SD).
Combined uncertainties were calculated by propagating the uncertainty of a single measurement as well as the total analytical error of HCT determination. The major contributor to the overall uncertainty of the primary end point is represented by the HCT value used for normalization with a contribution of > 90%. The uncertainty of the measurement contributes to the total uncertainty by < 10%. Subjects show a significantly different natural Pb isotopic composition in sample BL (t = 0). The 204Pb/208Pb isotope ratio at t = 0 before administration of the 204Pb tracer ranged from 0.026 to 0.038 with an average of 0.028 ± 0.002 (1 SD). This significant variation underlines the importance of using the measured natural Pb isotopic abundance as end member (= source 1) used in isotope pattern deconvolution instead of using tabulated representative natural Pb isotopic composition [8].
Figure S01–S42 show the relative enrichment (molar fraction of 204Pb tracer contributing to the total amount of Pb in blood normalized to HCT and BMI) for the 42 subjects (study phase 1 (6 subjects) and study phase 2 (36 subjects)) as a function of time. Error bars correspond to combined uncertainties u = 10% (k = 1). Subject-02 shows the highest enrichment of 204Pb, thus determining the maximum for the graphical visualization on the y-axis.
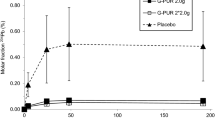
All subjects show enrichment of the 204Pb spike from BL (t = 0) to follow-up sampling times. The maximum accumulation in the blood occurs earliest at 24 h after administration. Figure 4 shows the maximum enrichment as 204Pb-molar fraction in Pb normalized to HCT/BMI of all 42 subjects from the three treatment groups after un-blinding of the treatment of each individual. The mean maximum 204Pb tracer enrichment was significantly higher in the placebo group compared to the treated groups including the IMD.

The maximum enrichment as 204Pb-molar fraction in Pb normalized to HCT/BMI of all 42 subjects from the three treatment groups (placebo, 1 × 2.0 g G-PUR and 2 × 2.0 g G-PUR) (independent of the time of maximum enrichment in tracer) sorted by enrichment, error bars correspond to u = 10% (k = 1)
The enrichment at 204Pb in blood differed significantly between the subjects. This allowed for assessing the efficacy of the administered clinoptilolite. The further medical interpretation of the results behind the clinical trial are discussed in Samekova et al. [16].
Results from urine samples of all subjects from clinical trial
The total concentration of Pb in urine samples was determined by ICP-QMS and further normalized to creatinine in urine as provided (see Table S04). All subjects show enrichment of the 204Pb spike from BL (t = 0) to 24 h (t = 24 h)-urine sample.
Data from urine of subject-04 could not successfully be evaluated as natural Pb from the background of the storage vessel (as a not pre-cleaned vessel was used accidently) significantly influenced the Pb background. A bias in the input sources to the regression model results in failure of the mathematical procedure. The enrichment of 204Pb differs significantly between the evaluated subjects. The relative uncertainties of > 60% can be explained by the low levels of Pb present in the samples. The major contributor to the uncertainty is the precision of the ICP-QMS measurement with a contribution of > 98% to the overall uncertainty, while the analytical error of creatinine determination amounted to < 2%. Excretion of 204Pb in 24-h urine was also decreased in subjects receiving the IMD compared to the placebo group. The medical implications of the results, which were obtained in the clinical trial, are discussed in Samekova et al. [16].
Conclusion
In this study, we successfully proved the applicability of isotope pattern deconvolution for data reduction when low levels of enriched isotope tracer (here: 204Pb) are orally administered (levels below the Austrian drinking water regulation (i.e. c(Pb) < 10 µg L−1)). The results showed for the first time that IPD allowed for the determination of tracer at levels of < 1 pg 204Pb/g matrix in a biological system, provided that comprehensive blank investigations are performed and that full control of the blank is achieved. ICP-QMS was selected over MC ICP-MS for Pb isotope ratio analysis, because sensitivity was the limiting factor. In this approach, we were able to measure isotope ratios of Pb with signals > 50 counts for the tracer isotope 204Pb. We stress that there was a substantial contribution by the uncertainty of clinical parameters used for normalization of Pb in blood and urine (BMI/HCT and CREA, respectively). Thus, the overall uncertainty was not determined by the measurement but by the normalization parameters. The combined uncertainty of enriched 204Pb molar fraction in blood of U (k = 2) was 20% and thus met the methodological requirement to determine a significant enrichment of the tracer. Finally, it is also conceivable that, due to sequential measurement of the isotopes of interest, the use of MC ICP-MS instead of single collector ICP-QMS may result in a further improvement of uncertainty.
The current study provides a proof-of-principle for employing enriched stable isotope tracers in clinical studies: the ultra-low levels required for the investigation keeps the administered amounts of tracer below any levels of concern.
References
Austoni ME, Greenberg DM. Studies in iron metabolism with the aid of its artificial radioactive isotope: the absorption, excretion, and distribution of iron in the rat on normal and iron-deficient diets. J Biol Chem. 1940;134(1):27–41.
Munro DD. Hair growth measurement using intradermal sulfur 35 cystine. Arch Dermatol. 1966;93(1):119–22.
Spencer H, Laszlo D, Brothers M. Strontium 85 and calcium 45 metabolism in man. J Clin Investig. 1957;36(5):680–8.
Creager ANH Life atomic. In: Life Atomic - A History of Radioisotopes in Science and Medicine. University of Chicago Press. ISBN-13: 978-0226323961; 2013.
Boulyga SF. Calcium isotope analysis by mass spectrometry. Mass Spectrom Rev. 2010;29(5):685–716.
Jones PJH, Leatherdale ST. Stable isotopes in clinical research: safety reaffirmed. Clin Sci. 1991;80(4):277–80.
Draxler J, Martinelli E, Weinberg AM, Zitek A, Irrgeher J, Meischel M, Stanzl-Tschegg SE, Mingler B, Prohaska T. The potential of isotopically enriched magnesium to study bone implant degradation in vivo. Acta Biomater. 2017;51:526–36.
Irrgeher J, Zitek A, Cervicek M, Prohaska T. Analytical factors to be considered for the application of enriched strontium spikes to monitor biological systems. J Anal At Spectrom. 2014;29(1):193–200.
Irrgeher J, Prohaska T. Application of non-traditional stable isotopes in analytical ecogeochemistry assessed by MC ICP-MS-A critical review. Anal Bioanal Chem. 2016;408(2):369–85.
Ab Latif Wani AA, Usmani JA. Lead toxicity: a review. Interdiscip Toxicol. 2015;8(2):55.
World-Health-Organization Preventing disease through healthy environments exposure to lead: a major public health concern. ISBN 9789240037632 (electronic version). 2019;vol WHO/CED/PHE/EPE/19.4.7.
Lanphear BP, Rauch S, Auinger P, Allen RW, Hornung RW. Low-level lead exposure and mortality in US adults: a population-based cohort study. Lancet Public Health. 2018;3(4):e177–84.
Kim H-C, Jang T-W, Chae H-J, Choi W-J, Ha M-N, Ye B-J, Kim B-G, Jeon M-J, Kim S-Y, Hong Y-S. Evaluation and management of lead exposure. Ann Occup Environ Med. 2015;27(1):1–9.
Bjørklund G, Mutter J, Aaseth J. Metal chelators and neurotoxicity: lead, mercury, and arsenic. Arch Toxicol. 2017;91(12):3787–97.
Committee on D. Treatment guidelines for lead exposure in children. Pediatrics. 1995;96(1):155–9.
Samekova K, Firbas C, Irrgeher J, Opper C, Prohaska T, Retzmann A, Tschegg C, Meisslitzer C, Tchaikovsky A, Gouya G. Concomitant oral intake of purified clinoptilolite tuff (G-PUR) reduces enteral lead uptake in healthy humans. Sci Rep. 2021;11(1):1–8.
Tong S, von Schirnding YE, Prapamontol T. Environmental lead exposure: a public health problem of global dimensions. Bull World Health Organ. 2000;78(9):1068–77.
Tchounwou PB, Yedjou CG, Patlolla AK, Sutton DJ. Heavy metal toxicity and the environment. Mol Clin Environ Toxicol. 2012;191:133–64. https://doi.org/10.1007/978-3-7643-8340-4_6.
Colella C. A critical reconsideration of biomedical and veterinary applications of natural zeolites. Clay Miner. 2011;46(2):295–309.
Beltcheva M, Metcheva R, Topashka-Ancheva M, Popov N, Teodorova S, Heredia-Rojas JA, Rodríguez-de la Fuente AO, Rodríguez-Flores LE. Zeolites versus lead toxicity. J Bioequiv Availab. 2015;7:12–29.
Shaheen SM, Derbalah AS, Moghanm FS. Removal of heavy metals from aqueous solution by zeolite in competitive sorption system. Int J Environ Sci Dev. 2012;3(4):362.
Sharifipour F, Hojati S, Landi A, Faz Cano A. Kinetics and thermodynamics of lead adsorption from aqueous solutions onto Iranian sepiolite and zeolite. Int J Environ Res. 2015;9(3):1001–10.
Wingenfelder U, Nowack B, Furrer G, Schulin R. Adsorption of Pb and Cd by amine-modified zeolite. Water Res. 2005;39(14):3287–97.
Erdem E, Karapinar N, Donat R. The removal of heavy metal cations by natural zeolites. J Colloid Interface Sci. 2004;280(2):309–14.
Ghasemi-Fasae RG, Haghigh M, Mousavi SM, Dehghan M. Sorption characteristics of heavy metals onto natural zeolite of clinoptilolite type. Int Res J Appl Basic Sci. 2012;3(10):2079–84.
Kragović M, Daković A, Sekulić Ž, Trgo M, Ugrina M, Perić J, Gatta GD. Removal of lead from aqueous solutions by using the natural and Fe (III)-modified zeolite. Appl Surf Sci. 2012;258(8):3667–73.
MaP E-G, Mattusch J, Wennrich R, Morgenstern P. Uptake of arsenite and arsenate by clinoptilolite-rich tuffs. Microporous Mesoporous Mater. 2001;46(2–3):277–86.
Elizalde-Gonzalez MP, Mattusch J, Einicke WD, Wennrich R. Sorption on natural solids for arsenic removal. Chem Eng J. 2001;81(1–3):187–95.
Faghihian H, Marageh MG, Kazemian H. The use of clinoptilolite and its sodium form for removal of radioactive cesium, and strontium from nuclear wastewater and Pb2+, Ni2+, Cd2+, Ba2+ from municipal wastewater. Appl Radiat Isot. 1999;50(4):655–60.
Mier MV, Callejas RL, Gehr R, Cisneros BEJ, Alvarez PJJ. Heavy metal removal with mexican clinoptilolite: multi-component ionic exchange. Water Res. 2001;35(2):373–8.
Delkash M, Bakhshayesh BE, Kazemian H. Using zeolitic adsorbents to cleanup special wastewater streams: a review. Microporous Mesoporous Mater. 2015;214:224–41.
Puschenreiter M, Horak O, Friesl W, Hartl W. Low-cost agricultural measures to reduce heavy metal transfer into the food chain–a review. Plant Soil Environ. 2005;51(1):1–11.
ISO-14155:2020 Clinical investigation of medical devices for human subjects — good clinical practice. (2020);vol ISO/TC-194 (2020). ISO 14155:2020 Switzerland.
Commission Directive 98/63/EC of 3 September 1998 amending Council Directive 93/16/EEC to facilitate the free movement of doctors and the mutual recognition of their diplomas, certificates and other evidence of formal qualifications (Text with EEA relevance). (1998).
Chalk S, McEwen L. The IUPAC gold book. Chem Int. 2017;39(3):25–30.
Tschegg C, Hou Z, Rice AHN, Fendrych J, Matiasek E, Berger T, Grasemann B. Fault zone structures and strain localization in clinoptilolite-tuff (Nižný Hrabovec, Slovak Republic). J Struct Geol. 2020;138:104090.
Tschegg C, Rice AHN, Grasemann B, Matiasek E, Kobulej P, Dzivák M, Berger T. Petrogenesis of a large-scale miocene zeolite tuff in the eastern Slovak Republic: The Nižný Hrabovec open-pit clinoptilolite mine. Econ Geol. 2019;114(6):1177–94.
Österreichisches Bundeskanzleramt, Verordnung des Bundesministers für soziale Sicherheit und Generationen über die Qualität von Wasser für den menschlichen Gebrauch (Trinkwasserverordnung-TWV). TWV, Vienna. 2001.
Reese A, Zimmermann T, Pröfrock D, Irrgeher J. Extreme spatial variation of Sr, Nd and Pb isotopic signatures and 48 element mass fractions in surface sediment of the Elbe River Estuary-Suitable tracers for processes in dynamic environments? Sci Total Environ. 2019;668:512–23.
Retzmann A, Zimmermann T, Pröfrock D, Prohaska T, Irrgeher J. A fully automated simultaneous single-stage separation of Sr, Pb, and Nd using DGA resin for the isotopic analysis of marine sediments. Anal Bioanal Chem. 2017;409(23):5463–80.
CIAAW Commission on isotopic abundances and atomic weights. ciaaw.org. 2022. Accessed 07 June 2022.
National Institute of Standards and Technology Standard Reference Material NIST SRM 981. 1991.
Wagner S, Santner J, Irrgeher J, Puschenreiter M, Happel S, Prohaska T. Selective diffusive gradients in thin films (DGT) for the simultaneous assessment of labile Sr and Pb concentrations and isotope ratios in soils. Anal Chem. 2022;94(16):6338–46.
Sysmex-Corporation XN series_RIAm_V2.2_additional performance characteristics_de.docx. 2017.
Acknowledgements
Sara Widhalm is gratefully acknowledged for assistance in the laboratory. We thank Matthias Klose, Ines Czucker and Michael Stern (all GHSR) for their support of the clinical trial.
Funding
Open access funding provided by Montanuniversität Leoben.
Author information
Authors and Affiliations
Contributions
J. Irrgeher: Designed research, performed research, contributed analytic tools, analysed data, wrote the paper.
T. Berger: Designing the research, analysed data, reviewed the paper.
A. Retzmann: Performed research, analysed data, reviewed the paper.
C. Opper: Performed research.
A. Tchaikovsky: Analysed data, wrote the paper.
C. Tschegg: Preparation of medical device, analysed data, reviewed the paper.
C. Meisslitzer: Preparation and coordination of clinical trial, reviewed the paper.
M. Freissmuth: Designing the research.
G. Gouya: Designing the research, preparation and coordination of clinical trial.
M. Wolzt: Preparation and coordination of clinical trial.
C. Firbas: Preparation and coordination of clinical trial, performed clinical research.
K. Peschel-Credner: Preparation and coordination of clinical trial.
P. Lechner: Analysed data.
K. Anderle: Performed clinical research, reviewed the paper.
T. Prohaska: Designed research, performed research, contributed analytic tools, analysed data, wrote the paper.
Corresponding author
Ethics declarations
Ethics approval
Refer to clinicaltrials.gov identifier: NCT04138693 for details of approval.
Conflict of interest
The funder had no role in the design of the study; in the collection, analyses or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Financial interests: JI, AR, CO and TP have fully been employed by Montanuniversität Leoben (MUL). MUL has received research funding from Glock Health Science and Research GmbH in the double-blinded study. JI, AR, CO and TP declare no financial interests.
Non-financial interests: JI, AR, CO and TP declare no non-financial interests.
Financial interests: TB, AT, CT and CM have fully been employed by the funder Glock Health Science and Research GmbH. The funder had no role in the design of the study; in the collection, analyses or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Non-financial interests: The authors declare no non-financial interests.
Financial interests: MF, MW and KA were fully employed by the Center of Physiology and Pharmacology, Medical University of Vienna, which received research funding by Glock Health Science and Research GmbH.
Non-financial interests: MF was on the board of scientific advisors of the Gaston H. Glock Research Laboratories for Exploratory Drug Development at the time the study was carried out. KA and MW declare no non-financial interests.
Financial interests: CF was fully funded by the Department of Clinical Pharmacology, Medical University of Vienna. In her role, she was responsible for the clinical trial. CF declares no financial interests.
Non-financial interests: CF declares no non-financial interests.
Financial interests: GG and PL are self-employed with Gouya Insights and LGS-INSIGHTS, respectively, and were responsible for coordination, planning and statistical evaluation of the study. Both companies received research funding from Glock Health Science and Research GmbH.
Non-financial interests: The authors declare no non-financial interests.
Financial interests: KPC has been fully employed at Gouya Insights. She declares no financial interest.
Non-financial interests: KPC declares no non-financial interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Published in the topical collection Making Waves in Analytical Chemistry with guest editors Johanna Irrgeher, Evelyn Rampler, and Teresa Steininger-Mairinger.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Irrgeher, J., Berger, T., Tchaikovsky, A. et al. Enriched stable 204Pb as tracer at ultra-low levels in clinical investigations. Anal Bioanal Chem 415, 255–268 (2023). https://doi.org/10.1007/s00216-022-04311-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00216-022-04311-0