
Abstract
Drug-induced liver injury (DILI) represents one of the major causes why drugs have to be withdrawn from the market. In this study, we describe a new interaction between drug-exposed hepatocytes and natural killer (NK) cells. In a previous genome-wide expression analysis of primary human hepatocytes that had been exposed to clinically relevant concentrations of 148 drugs, we found that several activating ligands for NK cell receptors were regulated by various drugs (e.g., valproic acid, ketoconazole, promethazine, isoniazid). Especially expression of the activating NKG2D ligands (MICA, MICB and ULBPs) and the NKp30 ligand B7-H6 were upregulated in primary human hepatocytes upon exposure to many different drugs. Using the human hepatocyte cell lines Huh7 and HepG2, we confirmed that protein levels of activating NK cell ligands were elevated after drug exposure. Hepatocyte cell lines or primary human hepatocytes co-cultivated with NK cells caused enhanced NK cell activation after pretreatment with drugs at in vivo relevant concentrations compared to solvent controls. Enhanced NK cell activation was evident by increased cytotoxicity against hepatocytes and interferon (IFN)-γ production. NK cell activation could be blocked by specific antibodies against activating NK cell receptors. These data support the hypothesis that NK cells can modulate drug-induced liver injury by direct interaction with hepatocytes resulting in cytotoxicity and IFN-γ production.
Similar content being viewed by others


Introduction
Drug-induced liver injury (DILI) is one of the major challenges in drug development. (Godoy et al. 2013). It accounts for approximately 10% of all cases of acute hepatitis (Lewis et al. 2006) and is one of the most common causes of acute liver failure (Larson et al. 2005; Ostapowicz et al. 2002). Unfortunately, prediction of drugs with an increased risk of DILI still remains challenging based on the currently available technologies in toxicology, such as conventional animal experimentation but also based on in vitro systems with human hepatocytes (Godoy et al. 2013). Therefore, a deeper understanding of the involved mechanisms is critical to improve prediction and to establish better clinical interventions.
Immune cell-mediated mechanisms play a relevant role in the pathogenesis of DILI (Godoy et al. 2013). Natural killer (NK) cells are innate lymphocytes that are essential for providing immunity against viral infections and cancer. They have the ability to detect transformed or infected cells and to induce apoptosis via the release of perforin- and granzyme-containing granules or via the engagement of death receptors such as Fas or TRAIL (Prager et al. 2019). In addition, they produce cytokines such as IFN-γ, TNF-α and others to shape the adaptive immune response. NK cell cytotoxicity is regulated via signals from activating and inhibitory surface receptors and is additionally influenced by cytokines (Watzl 2014). In the liver, NK cells are involved in physiological and pathophysiological processes such as viral infections, liver tumorigenesis, liver injury and inflammation (Fasbender et al. 2016; Peng and Tian 2015). Liver NK cells play a key role in liver fibrosis (Fasbender et al. 2016) and have been reported to be able to kill hepatocytes (Ochi et al. 2004). Unlike T or B cells, NK cells are regulated by an array of germline-encoded activating and inhibitory receptors (Watzl 2014). Inhibitory receptors specific for self-MHC I are important to ensure the self-tolerance of NK cells. The activating Fc receptor CD16 can recognize antibody-coated cells, while other activating receptors recognize ligands on stressed or infected cells. In humans, eight ligands for the activating receptor NKG2D have been described, which are members of either the MIC (MICA and MICB) (Bahram et al. 2005) or the ULBP (ULBP1, ULBP2, ULBP3, ULBP4, RAET1G and RAET1L) family (Bacon et al. 2004; Chalupny et al. 2003; Cosman et al. 2001). Known ligands for the activating NKp30 receptor include B7-H6 (Brandt et al. 2009) and BAT3 (Pogge von Strandmann et al. 2007).
Currently, it is unknown whether the pretreatment of hepatocytes with compounds known to induce immune-mediated DILI may influence the activity of NK cells. Here, we show that ligands for the activating NK cell receptors NKp30 and NKG2D are upregulated on hepatocytes upon drug exposure. This induces the activation of NK cells resulting in cellular cytotoxicity and the production of IFN-γ.
Methods
Cell culture
Peripheral blood mononuclear cells (PBMCs) were isolated from the blood of healthy donors by Ficoll density gradient centrifugation (PAN-Biotech, Aidenbach Germany). Human NK cells were purified from PBMCs using the Dynabeads Untouched Human NK Cell kit (Thermo Fisher Scientific, Waltham, Massachusetts, USA) according to manufacturer’s instructions. For NK cell activation and expansion, purified NK cells were cultured in 96-well round-bottom plates (Nunc) with irradiated K562-mbIL15-41BBL (kind gift from Dario Campana) in IMDM Glutamax supplemented with 10% FCS and 1% penicillin/streptomycin, IL-2 (100 U/ml, NIH Cytokine Repository) and IL-15 (5 ng/ml, PAN-Biotech). IL-21 (100 ng/ml, Miltenyi Biotec, Bergisch Gladbach Germany) was added at the first day. NK cells were between 90 and 99% CD3−, CD56+, and NKp46+ as assessed by flow cytometry. Huh7 cells were cultivated in Dulbecco’s modified Eagle’s medium (DMEM) containing 4.5% glucose, 1% penicillin/streptomycin mixture and 10% heat-inactivated FCS. Primary human hepatocytes were cultivated in William’s E medium (PAN Biotech, P04_29510) with 100 U/ml penicillin, 0,1 mg/ml streptomycin, 10 μg/ml gentamicin, 2 mM stable glutamine, 100 nM dexamethasone and 2 nM insulin–transferrin–selenite (ITS) supplement. When plating cells, 10% fetal calf serum was added for the first 3–4 h of cultivation.
RTCA assay
Cells were seeded on the E-Plate PET 16 (Omni Life Science, Bremen Germany) according to the manufacturer’s recommendations. First, a background reading was performed in the presence of 100 μl medium. Then cells were seeded and allowed to attach for 30 min at room temperature. For experiments with PHH, E-Plates were pre-coated with a monolayer of collagen according to the manufacturer’s instructions. Briefly, E-Plates were incubated with 50 μl of collagen for 1 h at 37 °C, then washed with PBS and air-dried. Drugs were added the next day for 24 h, then cells were washed with PBS and NK cells were added with fresh, drug-free medium for co-culture. Cell Index was recorded every 5 min by the RTCA xCELLigence DP (Acea Bioscience, San Diego, California, USA). Cell index was normalized to the time point before addition of NK cells and deltaCI was calculated as shown in Fig. 3a. For blocking experiments, NK cells were preincubated with specific antibodies against NKp30 (p30-15, own production), or control IgG (MOPC21, Sigma-Aldrich, St. Louis, Missouri, USA) for 30 min on ice at 10 μg/ml and were then added to the E-Plate at RT.
After the experiment, supernatants were anaylzed for IFN-γ by ELISA (Biolegend, San Diego, California, USA) according the manufacturer’s instructions. For some experiments, adherent Huh7 cells were analyzed by Cell Titer Blue assay (Promega, Madison, Wisconsin, USA) according to the manufacturer’s instructions.
The following drugs were used: aspirin (A5376, Sigma-Aldrich, St. Louis, Missouri, USA), isoniazid (I3377, Sigma-Aldrich), ketoconazole (K1003), Sigma-Aldrich), promethazine (P4651, Sigma-Aldrich) and valproic acid (PHR1061, Sigma-Aldrich).
Flow cytometry
Flow cytometric analysis was performed according to recently published guidelines (Andrea Cossarizza 2019). Huh7 cells were harvested using cell dissociation buffer (Gibco—Thermo Fisher Scientific, Waltham, Massachusetts, USA) to prevent loss of trypsin-sensitive ligands. Subsequently, cells were blocked with mouse serum to prevent unspecific antibody binding and then stained with the viability dye 7AAD (Biolegend San Diego, California, USA), followed by staining for NK cell ligands with human B7-H6 APC-conjugated antibody (FAB7144A, clone # 875001; R&D Systems, Minneapolis, Minnesota, USA), human ULBP-2/5/6 PE-conjugated antibody (FAB1298P, clone # 165903, R&D Systems), MICA/B AF488 (FAE-13001G, RD Systems) or isotype controls APC mouse IgG1 (BioLegend), FITC mouse IgG1 (BioLegend), PE-mouse IgG1 (Santa-Cruz) and PE-Cy5 mouse IgG1 (BD Biosciences, Heidelberg, Germany). Cells were analyzed by LSR Fortessa (BD, Franklin Lakes, New Jersey, USA) and FlowJo (BD).
Results
Drug exposure of human hepatocytes induces the expression of activating NK cell ligands
Previously, we established a toxicogenomics directory with genome-wide expression data of primary human hepatocytes (PHH) that have been exposed to in vivo relevant concentrations of 148 drugs (Grinberg et al. 2014). Using this dataset, we found that the expression of several ligands of NK cell receptors is influenced by drug exposure (Supplemental Table 1). Particularly, the expression of the activating NKG2D ligands (MICA, MICB, and ULPBs) and the NKp30 ligand B7-H6 was upregulated in hepatocytes upon exposure to many different drugs. No inhibitory ligands were significantly increased or decreased by drug exposure. Thus, we hypothesized that NK cells are activated by drug-exposed hepatocytes and therefore modulate DILI by cytotoxicity and IFN-γ production.
To test this, we focused on drugs with the strongest upregulation of activating NK cell ligands (Fig. 1). Promethazine (PMZ) and isoniazid (INAH) only increased the expression of the NKp30 ligand B7-H6. Valproic acid (VPA) induced increased expression of several NKG2D ligands, including MICA and ULBP2, but not expression of B7-H6. This was previously reported only for HepG2 and Huh7 hepatocyte cancer cell lines, but not for PHH (Armeanu et al. 2005). Ketoconazole (KC) induced strong upregulation of both NKG2D ligands and the NKp30 ligand. As a negative control we choose acetylsalicylic acid (ASA) as a known non-hepatotoxic compound that did not upregulate activating NK cell ligands.

Heat map of mRNA expression of primary human hepatocytes (PHH) after exposure to the indicated drugs for selected genes of activating NK cell ligands. RNA extracted from PHH was analyzed on Affymetrix HG U133 Plus 2.0 arrays in triplicates (hepatocytes isolated from three donors on three different occasions). PHH were treated for 24 h with aspirin (ASA) (200 μM), isoniazid (INAH) (2 mM), ketoconazole (KC) (30 μM), promethazine (PMZ) (10 μM) and valproic acid (VPA) (2 mM) and then analyzed as described. (Data from Grinberg et al. 2014)
Activating NK cell ligand protein is increased in Huh7 cells after drug exposure
Analysis of PHH by flow cytometry was not possible, since these cells could not be detached from their collagen-coated culture plates without affecting surface receptor expression, and alternative methods such as Western blot or immunostaining did not allow quantification with sufficient sensitivity. Therefore, we investigated if the cell lines Huh7 and HepG2 show similar effects as PHH after drug exposure on the protein level by using flow cytometry. Huh7 cells showed some basal expression of B7-H6, which was markedly upregulated by incubation with PMZ, INAH, and KC, but not ASA or VPA (Supplemental Figs. 1 and 2). The NKG2D ligands MICA and MICB were only slightly upregulated after treatment with VPA, while all other samples showed only background levels of expression. Expression of ULBP ligands increased after exposure to KC and VPA. Comparable data were obtained with HepG2 cells (data not shown) (Fig. 2).

Expression of activating NK cell ligands after drug exposure of Huh7 cells. Huh7 cells were seeded in six-well plates and then repeatedly treated with (ASA) (200 μM), isoniazid (INAH) (2 mM), ketoconazole (KC) (30 μM), promethazine (PMZ) (10 μM), valproic acid (VPA) (2 mM) for 72 h once ever day. Cells were then harvested, stained with specific antibodies against activating NK cell ligands or an appropriate isotype control and analyzed by flow cytometry. a FACS histograms are representative of at least three independent experiments. b Quantification of FACS analysis (n = 3–4 per drug). Analyzed for statistical significance by two-way ANOVA. A p of < 0.05 was considered significant (*p < 0.05, **p < 0.01)
These data confirm the results of the expression analysis and show that drug-specific exposure of hepatocytes can result in increased surface expression of ligands for activating NK cell receptors. Furthermore, we could demonstrate this effect in two different hepatocyte cell lines, Huh7 and HepG2, establishing these cells as suitable for subsequent experiments.
Enhanced NK-cell cytotoxicity against drug-exposed hepatocytes
To test the effect of drug-exposed hepatocytes on NK cells, we set up a co-culture system that could detect cytotoxicity label free in real time. Typically, NK cell cytotoxicity is measured against hematological target cells, which grow in suspension culture. However, hepatocytes are adherently growing cells. Detachment of these cells using standard trypsin-based protocols can affect NK cell ligands such as B7-H6 on the surface of hepatocytes (Byrd et al. 2007). The handling of these cells in suspension can create additional artifacts. To circumvent these problems, we established the Real-Time Cell Analyzer (RTCA) xCELLigence system. This technology is based on electric impedance and can determine the proliferation and viability of adherent cells in real time in a label-free and non-invasive fashion (Atienzar et al. 2013). The RTCA system has been used and extensively characterized for toxicity assays in primary human hepatocytes and cell lines (Atienzar et al. 2013, 2011; Kho et al. 2015) as well as immunological assays (Fasbender and Watzl 2018; Moodley et al. 2011; Peper et al. 2014). In our study, we combine both applications and make use of the advantage that the RTCA allows differentiation of cytotoxicity caused by drugs or NK cells.
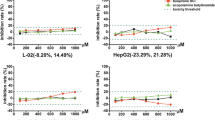
To investigate NK cell-mediated killing of hepatocytes, Huh7 or HepG2 cells were seeded in E-Plates coated with gold electrodes to continuously measure the viability of these adherent cells. After incubation overnight, the drugs were added for 24 h at previously determined sub-toxic concentrations that did not significantly affect the cell index signal. To prevent the effects of the drugs on NK cells, hepatocytes were washed twice before the addition of NK cells in drug-free medium, followed by co-culture for 24 h. After that, the supernatant was analyzed by ELISA for IFN-γ. Additionally, we could confirm the correlation between cell index and viability by CellTiter Blue assay (Supplemental Fig. 2). Using this assay, we observed increased cytotoxicity of NK cells against Huh7 cells incubated with sub-toxic concentrations of INAH, KC, PMZ and VPA but not ASA (Fig. 3). To further validate the enhanced activation of NK cells, we measured IFN-γ by ELISA from the same experiments. IFN-γ was increased in the supernatants of INAH, KC and VPA-treated Huh7 cells after co-culture with NK cells, but not after ASA and PMZ treatment (Fig. 4). Together, these data demonstrate enhanced NK cell effector functions against hepatocyte cell lines for the drugs that induced expression if activating ligands. While most of our data were restricted to hepatocyte cell lines, we confirmed upregulation of activating NK cell ligands in PHH after drug exposure and demonstrated enhanced NK cytotoxicity for some drugs (Fig. 1 and Supplemental Fig. 3).

Cytotoxicity assay conducted as shown in (a). Huh7 cells were seeded in E-Plates, treated with (ASA) (200 μM), isoniazid (INAH) (2 mM), ketoconazole (KC) (30 μM), promethazine (PMZ) (10 μM) and valproic acid (VPA) (2 mM), and NK cells were added after washing for 24 h of co-culture. Cell index was recorded every 5 min. Delta cell index was calculated for each drug as depicted in (a). Data points represent biological replicates with different NK cell donors conducted in technical duplicates or triplicates. a Experimental procedure and representative experiment. b Quantification of killing assays for all drugs as depicted in (a). Analyzed for statistical significance by paired t test. A p of < 0.05 was considered significant (*p < 0.05, **p < 0.01)

IFN-γ levels are increased after NK cell co-culture with drug-treated Huh7 cells. Supernatants from experiments described in Fig. 3 were analyzed by ELISA for IFN-γ. Analyzed for statistical significance by paired t test. A p of < 0.05 was considered significant (*p < 0.05, **p < 0.01)
Blocking by specific antibodies
Our hypothesis implicates the activating receptors NKp30 and NKG2D as main mediators of the observed drug-dependent effects. Therefore, blocking these receptors should attenuate increased NK cell activation in a drug-specific manner. To test this, we used a neutralizing antibody against NKp30. Blocking NKp30 resulted in reduced NK cell-mediated killing of Huh7 cells treated with ASA, but also in the absence of any drug treatment. This is consistent with the fact that these cells already express low levels of B7-H6 on their surface (Fig. 2a). Notably, blocking of the NKp30 receptor inhibited the increase in NK cell-mediated killing of INAH- and PMZ-treated Huh7 cells, consistent with the upregulation of B7-H6 by these drugs. In contrast, the increased killing of KC-treated Huh7 cells was not blocked by anti-NKp30 antibodies, suggesting that the additional upregulation of NKG2D ligands may compensate for the loss of B7-H6-mediated NK cell activation. Blocking of NKG2D after VPA treatment has been previously described for hepatoma cells (Armeanu et al. 2005). These data support the hypothesis that the upregulation of activating NK cell ligands can make hepatocytes more susceptible to NK cell-mediated cytotoxicity (Fig. 5).

Blocking of NKp30 reduced the effect of INAH and PMZ. NK cells were pre-incubated with NKp30 antibody or an isotype control before co-culture with drug-treated Huh7 cells. Cytotoxicity during co-culture was measured as before by impedance. Huh7 cells were seeded in E-Plates and pretreated with a ASA, b INAH, c KC or d PMZ as before, while NK cells were preincubated with NKp30 antibody or an isotype control for 30 min on ice. Both cell types were washed before co-culture and then co-incubated in E-Plates for 24 h. Cell index was recorded every 5 min and deltaCI was calculated as previously shown in Fig. 3. Analyzed for statistical significance by paired t test. A p of < 0.05 was considered significant (*p < 0.05)
Discussion
Immune cells are known to play an important role in the development and progression of drug-induced liver injury (Adams et al. 2010; Mak and Uetrecht 2017) as well as liver fibrosis (Fasbender et al. 2016). In humans, NK cells are enriched in the liver compared to blood and are important regulators of liver homeostasis. Early activated and senescent hepatic stellate cells are directly killed by NK cells via activating receptors NKG2D (Melhem et al. 2006; Muhanna et al. 2011; Radaeva et al. 2006) and NKp46 (Gur et al. 2012). This interaction can be modulated by regulatory CD4 T cells (Langhans et al. 2015). Furthermore, NK cells contribute to the defense of viral infections in the liver (Kramer et al. 2012; Mantovani et al. 2015; Wijaya et al. 2019). However, much is still unknown about specific roles and interactions. Here, we provide evidence for a direct role of NK cells in the death of hepatocytes after drug exposure. We found a drug-specific increase in expression of activating NK cell ligands on drug-exposed primary human hepatocytes as well as hepatocyte cell lines which increased NK cell effector functions in co-culture experiments (Fig. 6).

Graphical summary of our findings. See text for details
The expression of activating ligands for NK cell receptors is usually restricted to infected or transformed cells. The ligands for NKG2D are related to MHC class I proteins, but the expression of NKG2D ligands is restricted or absent on normal cells. They are upregulated under conditions of stress and disease such as pathogen infection or tumor transformation, often involving DNA-damage pathways, which renders these cells susceptible to NK cell lysis (Raulet et al. 2013). B7-H6, the ligand for NKp30 (Brandt et al. 2009), is not detected in normal human tissues, but is selectively expressed on a variety of human tumor cell lines, including T and B lymphomas, melanomas, and carcinomas. Therefore, it is likely that the drugs in our study act via a stress mechanism to induce the expression of activating ligands for NKG2D and NKp30. Surprisingly, this seems to be a very drug-specific effect that does not appear to be connected to the drug metabolism and mode of action. Previous studies have shown that some ligands for activating NK cell receptors can be shed from the surface of cells (Deng et al. 2015; Schlecker et al. 2014). Indeed, we observed soluble B7-H6 in the supernatant of drug-exposed hepatocytes (Supplemental Fig. 4). While this did not inhibit NK cell cytotoxicity in our in vitro assays, soluble B7-H6 and other NK ligands shed by drug-exposed hepatocytes could influence NK cell reactivity in vivo.
The liver contains two well-characterized NK cell sub-populations. Liver resident (lrNK) NK cells do not enter circulation while the conventional, non-resident NK cell population (cNK) can also be detected in the peripheral blood. In our study, we used activated peripheral blood NK cells, which resemble cNK during inflammation. In the present study, a co-culture system of human NK cells and liver cells was applied, where a direct contact between both cell types can be established. This may differ from the in vivo situation, where immune cells in the lumen of liver sinosoids are separated from hepatocytes by liver sinusoidal endothelial cells (LSEC). However, LSEC contain numerous fenestrations and it has been shown that their size is large enough to allow a direct interaction of cytotoxic T cells with hepatocytes in vivo (Warren et al. 2006). Therefore, NK cell receptors may also contact activating ligands on hepatocytes through the fenestrae of LSEC. It is interesting to note that lrNK cells possess memory-like features (Watzl et al. 2014). Mice exposed to haptens demonstrated enhanced activation of NK cells upon repeated exposure. (Paust et al. 2010). This memory-like effect could also play an important role in DILI, as repeated exposure to the same drugs possibly generates memory-like NK cells with enhanced effector functions.
The role of NK cells in liver injury is likely context dependent and may even change during the progression of the same liver disease. While the killing of hepatocytes by NK cells represents a direct injury to the liver, the removal of stressed or damaged hepatocytes by NK cells could also be beneficial. Stressed hepatocytes produce IL-33, which activates ILC2 (McHedlidze et al. 2013; Weiskirchen and Tacke 2017). The production and release of IL-5 and IL-13 by ILC2 contributes to liver injury. Killing of activated hepatic stellate cells—which also present activating ligands for NK cells during early activation and senescence—is known to inhibit the development of liver fibrosis (Fasbender et al. 2016; Gur et al. 2012; Melhem et al. 2006; Radaeva et al. 2006, 2007). In addition, IFN-γ can act on a number of cells dependent on the state of the liver (Horras et al. 2011). During the early stages and probably before the progression to fibrosis, NK cells and IFN-γ exert mostly anti-fibrotic functions (Gao et al. 2007). IFN-γ can act on hepatic stellate cells to prevent their activation directly or to stimulate the upregulation of activating NK cell ligands. Treatment with exogenous IFN-γ attenuated liver fibrosis in CCl4-induced murine models (Rockey and Chung 1994). In contrast, IFN-γ produced by NK cells can be a negative regulator of liver regeneration (Sun and Gao 2004; Wei et al. 2010). Exogenous IFN-γ had the same effect, while depletion of NK cells enhanced the proliferation of hepatocytes (Sun and Gao 2004). In humans elevated levels of IFN-γ correlated with liver disease severity regardless of the underlying cause (Attallah et al. 2016). Taken together, these studies indicate that IFN-γ might be beneficial during the early stages of liver damage, but could have a negative effect during advanced stages of liver disease and liver regeneration.
In mice, treatment with INAH resulted in increased NK cell infiltration into the liver, which supports a role of NK cells in DILI (Mak and Uetrecht 2015). However, it should also be noted that some of the drugs used in this study were also reported to affect NK cell functions (Gergely et al. 1984; Ogbomo et al. 2007; Ravn et al. 1995; Rychlik et al. 1988; Shi et al. 2016). Therefore, future studies need to address the in vivo relevance of our findings in a mouse model. However, it is important to conduct experiments with primary human cells and cell lines in vitro, as findings from murine studies often differ from human studies (Mestas and Hughes 2004). In humans, NK cells are more abundant in the liver compared to mice. Additionally, murine NK cells differ in their receptor repertoire and there is no known mouse homolog for the NKp30 receptor. While the in vivo consequences of the interaction between NK cells and hepatocytes depend on the context and the underlying disease as well as the drug, expression of activating NK cell ligands on hepatocytes could serve as a biomarker for the stress induced by the drugs. As drugs such as INAH are known to be idiosyncratic, these biomarkers could provide an early warning for the development of fibrosis and contribute to tailor-made individual treatment options.
In conclusion, we demonstrated that exposure of hepatocytes to in vivo relevant concentrations of DILI-mediating drugs induces expression of activating ligands and triggers hepatocyte killing by NK cells.
References
Adams DH, Ju C, Ramaiah SK, Uetrecht J, Jaeschke H (2010) Mechanisms of immune-mediated liver injury. Toxicol Sci 115(2):307–321. https://doi.org/10.1093/toxsci/kfq009
Andrea Cossarizza HDC, Radbruch A, Acs A, Adam D, Adam-Klages S, Agace WW, Aghaeepour N, Akdis M, Allez M, Almeida LN, Alvisi G, Anderson G, Andrä I, Annunziato F, Anselmo A, Bacher P, Baldari CT, Bari S, Barnaba V, Barros-Martins J, Battistini L, Bauer W, Baumgart S, Baumgarth N, Baumjohann D, Baying B, Bebawy M, Becher B, Beisker W, Benes V, Beyaert R, Blanco A, Boardman DA, Bogdan C, Borger JG, Borsellino G, Boulais PE, Bradford JA, Brenner D, Brinkman RR, Brooks AES, Busch DH, Büscher M, Bushnell TP, Calzetti F, Cameron G, Cammarata I, Cao X, Cardell SL, Casola S, Cassatella MA, Cavani A, Celada A, Chatenoud L, Chattopadhyay PK, Chow S, Christakou E, Čičin-Šain L, Clerici M, Colombo FS, Cook L, Cooke A, Cooper AM, Corbett AJ, Cosma A, Cosmi L, Coulie PG, Cumano A, Cvetkovic L, Dang VD, Dang-Heine C, Davey MS, Davies D, De Biasi S, Del Zotto G, Cruz GVD, Delacher M, Bella SD, Dellabona P, Deniz G, Dessing M, Di Santo JP, Diefenbach A, Dieli F, Dolf A, Dörner T, Dress RJ, Dudziak D, Dustin M, Dutertre C-A, Ebner F, Eckle SBG, Edinger M, Eede P, Ehrhardt GRA, Eich M, Engel P, Engelhardt B, Erdei A, Esser C, Everts B, Evrard M, Falk CS, Fehniger TA, Felipo-Benavent M, Ferry H, Feuerer M, Filby A, Filkor K, Fillatreau S, Follo M, Förster I, Foster J, Foulds GA, Frehse B, Frenette PS, Frischbutter S, Fritzsche W, Galbraith DW, Gangaev A, Garbi N, Gaudilliere B, Gazzinelli RT, Geginat J, Gerner W, Gherardin NA, Ghoreschi K, Gibellini L, Ginhoux F, Goda K, Godfrey DI, Goettlinger C, González-Navajas JM, Goodyear CS, Gori A, Grogan JL, Grummitt D, Grützkau A, Haftmann C, Hahn J, Hammad H, Hämmerling G, Hansmann L, Hansson G, Harpur CM, Hartmann S, Hauser A, Hauser AE, Haviland DL (2019) Guidelines for the use of flow cytometry and cell sorting in immunological studies. Eur J Immunol 49(10):1457–1973
Armeanu S, Bitzer M, Lauer UM et al (2005) Natural killer cell-mediated lysis of hepatoma cells via specific induction of NKG2D ligands by the histone deacetylase inhibitor sodium valproate. Cancer Res 65(14):6321–6329. https://doi.org/10.1158/0008-5472.CAN-04-4252
Atienzar FA, Tilmant K, Gerets HH et al (2011) The use of real-time cell analyzer technology in drug discovery: defining optimal cell culture conditions and assay reproducibility with different adherent cellular models. J Biomol Screen 16(6):575–587. https://doi.org/10.1177/1087057111402825
Atienzar FA, Gerets H, Tilmant K, Toussaint G, Dhalluin S (2013) Evaluation of impedance-based label-free technology as a tool for pharmacology and toxicology investigations. Biosensors (Basel) 3(1):132–156. https://doi.org/10.3390/bios3010132
Attallah AM, El-Far M, Zahran F et al (2016) Interferon-gamma is associated with hepatic dysfunction in fibrosis, cirrhosis, and hepatocellular carcinoma. J Immunoassay Immunochem 37(6):597–610. https://doi.org/10.1080/15321819.2016.1179646
Bacon L, Eagle RA, Meyer M, Easom N, Young NT, Trowsdale J (2004) Two human ULBP/RAET1 molecules with transmembrane regions are ligands for NKG2D. J Immunol 173(2):1078–1084
Bahram S, Inoko H, Shiina T, Radosavljevic M (2005) MIC and other NKG2D ligands: from none to too many. Curr Opin Immunol 17(5):505–509. https://doi.org/10.1016/j.coi.2005.07.016
Brandt CS, Baratin M, Yi EC et al (2009) The B7 family member B7–H6 is a tumor cell ligand for the activating natural killer cell receptor NKp30 in humans. J Exp Med 206(7):1495–1503. https://doi.org/10.1084/jem.20090681
Byrd A, Hoffmann SC, Jarahian M, Momburg F, Watzl C (2007) Expression analysis of the ligands for the natural killer cell receptors NKp30 and NKp44. PLoS ONE ONE 2(12):e1339. https://doi.org/10.1371/journal.pone.0001339
Chalupny NJ, Sutherland CL, Lawrence WA, Rein-Weston A, Cosman D (2003) ULBP4 is a novel ligand for human NKG2D. Biochem Biophys Res Commun 305(1):129–135
Cosman D, Müllberg J, Sutherland CL et al (2001) ULBPs, novel MHC class I-related molecules, bind to CMV glycoprotein UL16 and stimulate NK cytotoxicity through the NKG2D receptor. Immunity 14(2):123–133
Deng W, Gowen BG, Zhang L et al (2015) Antitumor immunity. A shed NKG2D ligand that promotes natural killer cell activation and tumor rejection. Science 348(6230):136–139. https://doi.org/10.1126/science.1258867
Fasbender F, Watzl C (2018) Impedance-based analysis of natural killer cell stimulation. Sci Rep. https://doi.org/10.1038/s41598-018-23368-5
Fasbender F, Widera A, Hengstler JG, Watzl C (2016) Natural killer cells and liver fibrosis. Front Immunol 7:19. https://doi.org/10.3389/fimmu.2016.00019
Gao B, Radaeva S, Jeong WI (2007) Activation of natural killer cells inhibits liver fibrosis: a novel strategy to treat liver fibrosis. Expert Rev Gastroenterol Hepatol 1(1):173–180. https://doi.org/10.1586/17474124.1.1.173
Gergely P, Nekam K, Lang I, Kalmar L, Gonzalez-Cabello R, Perl A (1984) Ketoconazole in vitro inhibits mitogen-induced blastogenesis, antibody-dependent cellular cytotoxicity, natural killer activity and random migration of human leukocytes. Immunopharmacology 7(3–4):167–170. https://doi.org/10.1016/0162-3109(84)90033-x
Godoy P, Hewitt NJ, Albrecht U et al (2013) Recent advances in 2D and 3D in vitro systems using primary hepatocytes, alternative hepatocyte sources and non-parenchymal liver cells and their use in investigating mechanisms of hepatotoxicity, cell signaling and ADME. Arch Toxicol 87(8):1315–1530. https://doi.org/10.1007/s00204-013-1078-5
Grinberg M, Stober RM, Edlund K et al (2014) Toxicogenomics directory of chemically exposed human hepatocytes. Arch Toxicol 88(12):2261–2287. https://doi.org/10.1007/s00204-014-1400-x
Gur C, Doron S, Kfir-Erenfeld S et al (2012) NKp46-mediated killing of human and mouse hepatic stellate cells attenuates liver fibrosis. Gut 61(6):885–893. https://doi.org/10.1136/gutjnl-2011-301400
Horras CJ, Lamb CL, Mitchell KA (2011) Regulation of hepatocyte fate by interferon-gamma. Cytokine Growth Factor Rev 22(1):35–43. https://doi.org/10.1016/j.cytogfr.2011.01.001
Kho D, MacDonald C, Johnson R et al (2015) Application of xCELLigence RTCA biosensor technology for revealing the profile and window of drug responsiveness in real time. Biosensors (Basel) 5(2):199–222. https://doi.org/10.3390/bios5020199
Kramer B, Korner C, Kebschull M et al (2012) Natural killer p46High expression defines a natural killer cell subset that is potentially involved in control of hepatitis C virus replication and modulation of liver fibrosis. Hepatology 56(4):1201–1213. https://doi.org/10.1002/hep.25804
Langhans B, Alwan AW, Kramer B et al (2015) Regulatory CD4(+) T cells modulate the interaction between NK cells and hepatic stellate cells by acting on either cell type. J Hepatol 62(2):398–404. https://doi.org/10.1016/j.jhep.2014.08.038
Larson AM, Polson J, Fontana RJ et al (2005) Acetaminophen-induced acute liver failure: results of a United States multicenter, prospective study. Hepatology 42(6):1364–1372. https://doi.org/10.1002/hep.20948
Lewis JH, Ahmed M, Shobassy A, Palese C (2006) Drug-induced liver disease. Curr Opin Gastroenterol 22(3):223–233. https://doi.org/10.1097/01.mog.0000218958.40441.fd
Mak A, Uetrecht J (2015) The combination of anti-CTLA-4 and PD1-/- mice unmasks the potential of isoniazid and nevirapine to cause liver injury. Chem Res Toxicol 28(12):2287–2291. https://doi.org/10.1021/acs.chemrestox.5b00305
Mak A, Uetrecht J (2017) Immune mechanisms of idiosyncratic drug-induced liver injury. J Clin Transl Res 3(1):145–156
Mantovani S, Mele D, Oliviero B, Barbarini G, Varchetta S, Mondelli MU (2015) NKp30 isoforms in patients with chronic hepatitis C virus infection. Immunology 146(2):234–242. https://doi.org/10.1111/imm.12495
McHedlidze T, Waldner M, Zopf S et al (2013) Interleukin-33-dependent innate lymphoid cells mediate hepatic fibrosis. Immunity 39(2):357–371. https://doi.org/10.1016/j.immuni.2013.07.018
Melhem A, Muhanna N, Bishara A et al (2006) Anti-fibrotic activity of NK cells in experimental liver injury through killing of activated HSC. J Hepatol 45(1):60–71. https://doi.org/10.1016/j.jhep.2005.12.025
Mestas J, Hughes CCW (2004) Of mice and not men: Differences between mouse and human immunology. J Immunol 172(5):2731–2738. https://doi.org/10.4049/jimmunol.172.5.2731
Moodley K, Angel CE, Glass M, Graham ES (2011) Real-time profiling of NK cell killing of human astrocytes using xCELLigence technology. J Neurosci Meth 200(2):173–180. https://doi.org/10.1016/j.jneumeth.2011.07.005
Muhanna N, Abu Tair L, Doron S et al (2011) Amelioration of hepatic fibrosis by NK cell activation. Gut 60(1):90–98. https://doi.org/10.1136/gut.2010.211136
Ochi M, Ohdan H, Mitsuta H et al (2004) Liver NK cells expressing TRAIL are toxic against self hepatocytes in mice. Hepatology 39(5):1321–1331. https://doi.org/10.1002/hep.20204
Ogbomo H, Michaelis M, Kreuter J, Doerr HW, Cinatl J Jr (2007) Histone deacetylase inhibitors suppress natural killer cell cytolytic activity. FEBS Lett 581(7):1317–1322. https://doi.org/10.1016/j.febslet.2007.02.045
Ostapowicz G, Fontana RJ, Schiodt FV et al (2002) Results of a prospective study of acute liver failure at 17 tertiary care centers in the United States. Ann Intern Med 137(12):947–954
Paust S, Gill HS, Wang B-Z et al (2010) Critical role for the chemokine receptor CXCR6 in NK cell-mediated antigen-specific memory of haptens and viruses. Nat Immunol 11(12):1127–1135. https://doi.org/10.1038/ni.1953
Peng H, Tian Z (2015) Re-examining the origin and function of liver-resident NK cells. Trends Immunol 36(5):293–299. https://doi.org/10.1016/j.it.2015.03.006
Peper JK, Schuster H, Loffler MW, Schmid-Horch B, Rammensee HG, Stevanovic S (2014) An impedance-based cytotoxicity assay for real-time and label-free assessment of T-cell-mediated killing of adherent cells. J Immunol Methods 405:192–198. https://doi.org/10.1016/j.jim.2014.01.012
Pogge von Strandmann E, Simhadri VR, von Tresckow B et al (2007) Human leukocyte antigen-B-associated transcript 3 is released from tumor cells and engages the NKp30 receptor on natural killer cells. Immunity 27(6):965–974. https://doi.org/10.1016/j.immuni.2007.10.010
Prager I, Liesche C, van Ooijen H et al (2019) NK cells switch from granzyme B to death receptor-mediated cytotoxicity during serial killing. J Exp Med 216(9):2113–2127. https://doi.org/10.1084/jem.20181454
Radaeva S, Sun R, Jaruga B, Nguyen VT, Tian Z, Gao B (2006) Natural killer cells ameliorate liver fibrosis by killing activated stellate cells in NKG2D-dependent and tumor necrosis factor-related apoptosis-inducing ligand-dependent manners. Gastroenterology 130(2):435–452. https://doi.org/10.1053/j.gastro.2005.10.055
Radaeva S, Wang L, Radaev S, Jeong WI, Park O, Gao B (2007) Retinoic acid signaling sensitizes hepatic stellate cells to NK cell killing via upregulation of NK cell activating ligand RAE1. Am J Physiol Gastrointest Liver Physiol 293(4):G809–G816. https://doi.org/10.1152/ajpgi.00212.2007
Raulet DH, Gasser S, Gowen BG, Deng W, Jung H (2013) Regulation of ligands for the NKG2D activating receptor. Annu Rev Immunol 31:413–441. https://doi.org/10.1146/annurev-immunol-032712-095951
Ravn P, Linnet J, Klokker M, Pedersen BK (1995) Effects of isoniazid treatment on human lymphocyte proliferative response, lymphocyte subsets and natural-killer-cell activity. Immunopharmacology 30(3):247–253. https://doi.org/10.1016/0162-3109(95)00029-S
Rockey DC, Chung JJ (1994) Interferon gamma inhibits lipocyte activation and extracellular matrix mRNA expression during experimental liver injury: implications for treatment of hepatic fibrosis. J Investig Med 42(4):660–670
Rychlik G, Rychlik E, Wasik M (1988) Influence of promethazine on immune-reactions. 1. Characterization of promethazine effects on natural-killer cell-mediated cyto-toxicity. Immunopharmacology 15(2):117–122. https://doi.org/10.1016/0162-3109(88)90058-6
Schlecker E, Fiegler N, Arnold A et al (2014) Metalloprotease-mediated tumor cell shedding of B7–H6, the ligand of the natural killer cell-activating receptor NKp30. Cancer Res 74(13):3429–3440. https://doi.org/10.1158/0008-5472.CAN-13-3017
Shi X, Li M, Cui M et al (2016) Epigenetic suppression of the antitumor cytotoxicity of NK cells by histone deacetylase inhibitor valproic acid. Am J Cancer Res 6(3):600–614
Sun R, Gao B (2004) Negative regulation of liver regeneration by innate immunity (natural killer cells/interferon-gamma). Gastroenterology 127(5):1525–1539. https://doi.org/10.1053/j.gastro.2004.08.055
Warren A, Le Couteur DG, Fraser R, Bowen DG, McCaughan GW, Bertolino P (2006) T lymphocytes interact with hepatocytes through fenestrations in murine liver sinusoidal endothelial cells. Hepatology 44(5):1182–1190. https://doi.org/10.1002/hep.21378
Watzl C (2014) How to trigger a killer: modulation of natural killer cell reactivity on many levels. Adv Immunol 124:137–170. https://doi.org/10.1016/B978-0-12-800147-9.00005-4
Watzl C, Urlaub D, Fasbender F, Claus M (2014) Natural killer cell regulation—beyond the receptors. F1000Prime Rep 6:87. https://doi.org/10.12703/P6-87
Wei HR, Wei HM, Wang H, Tian ZG, Sun RI (2010) Activation of natural killer cells inhibits liver regeneration in toxin-induced liver injury model in mice via a tumor necrosis factor-alpha-dependent mechanism. Am J Physiol Gastr L 299(1):G275–G282. https://doi.org/10.1152/ajpgi.00026.2010
Weiskirchen R, Tacke F (2017) Interleukin-33 in the pathogenesis of liver fibrosis: alarming ILC2 and hepatic stellate cells. Cell Mol Immunol 14(2):143–145. https://doi.org/10.1038/cmi.2016.62
Wijaya RS, Read SA, Schibeci S et al (2019) KLRG1+ natural killer cells exert a novel antifibrotic function in chronic hepatitis B. J Hepatol 71(2):252–264. https://doi.org/10.1016/j.jhep.2019.03.012
Acknowledgements
Open Access funding provided by Projekt DEAL. The authors thank Wiebke Albrecht, Tim Brecklinghaus and Agata Widera for their support. This work was supported by a grant from the DFG to Carsten Watzl (WA 1552/8-1) and Jan G. Hengstler (HE 2509/14-1).
Author information
Authors and Affiliations
Contributions
FF conceived the hypothesis. FF, MO, RS and SM conducted experiments. FF, JH and CW designed experiments, analyzed data and wrote the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fasbender, F., Obholzer, M., Metzler, S. et al. Enhanced activation of human NK cells by drug-exposed hepatocytes. Arch Toxicol 94, 439–448 (2020). https://doi.org/10.1007/s00204-020-02668-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00204-020-02668-8