
Abstract
Summary
This large-scale prospective study showed that a significant association between longer duration of daily outdoor walking and reduced osteoporosis risk was found among older adults, particularly among those with a low genetic predisposition to osteoporosis, which highlighted the importance of outdoor walking as a simple, cost-effective adjunct for preventing osteoporosis.
Purpose
The available cross-sectional data and small-scale studies indicate that outdoor walking benefits bone metabolism. Nevertheless, there is a scarcity of comprehensive prospective research investigating the enduring correlation between outdoor walking and osteoporosis. This study aims to conduct a prospective analysis of the correlation between outdoor walking and osteoporosis while also examining potential variations influenced by genetic susceptibility to osteoporosis.
Methods
24,700 older adults without osteoporosis at baseline were enrolled. These individuals were followed up until December 31, 2021, during which data on outdoor walking was gathered. The genetic risk score for osteoporosis was comprised of 14 single-nucleotide polymorphisms.
Results
4,586 cases of osteoporosis were identified throughout a median follow-up period of 37.3 months. Those who walked outside for > 30 but ≤ 60 min per day had a hazard ratio (HR) of 0.83 (95% confidence interval (CI): 0.72–0.95) for incident osteoporosis, whereas those who walked outside for > 60 min per day had an HR of 0.60 (95% CI: 0.39–0.92). We found that osteoporosis risk exhibited a declining trend in individuals with low genetic risk. Individuals walking outside for > 60 min per day tended to have the lowest overall osteoporosis risk among those with high genetic risk.
Conclusions
A significant negative correlation exists between an extended period of daily outdoor walking and osteoporosis incidence risk. This correlation is particularly pronounced among individuals with low genetic risk. The results above underscore the significance of outdoor walking as a simple and economical adjunct to public health programs to prevent osteoporosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Osteoporosis is a widespread global systemic skeletal disorder, distinguished by reduced bone mass and increased susceptibility to bone fragility. In cross-sectional research conducted in mainland China, the prevalence of osteoporosis among persons aged 40 years or older was 5.0% among men and 20.6% among women. Additionally, the prevalence of vertebral fractures was 10.5% among men and 9.7% among women [1]. The future is expected to see a significant rise in the prevalence of osteoporosis and the incidence of fragility fractures in China, mostly due to the fast development of the aging population in the country [2]. According to projections, it is anticipated that China will experience approximately 5.99 million osteoporosis-related fractures annually by the year 2050, with a confidence interval (CI) of 5.44 to 6.55 million. The economic burden associated with these fractures is estimated to be around $25.43 billion, with a CI of $23.92 to $26.95 billion. This represents a 2.7-fold increase compared to the figures recorded in 2010 [3]. Notably, a portion of these fractures could have been prevented by adopting healthier lifestyle behaviors, such as engaging in regular physical activity. As shown by several studies and expert recommendations, physical exercise is widely acknowledged as a key approach to promoting bone health [4]. The World Health Organization, for instance, advises individuals to engage in a minimum of 150 min per week of moderate-intensity aerobic physical activity or a minimum of 75 min per week of vigorous-intensity aerobic physical activity [5]. According to recent data, a significant number of individuals globally, estimated by 31.1% (95% CI 30.9–31.2), engage in insufficient physical activity. This prevalence varies across regions, ranging from 17.0% (16.8–17.2) in southeast Asia to around 43% in the Americas and the eastern Mediterranean. The prevalence of inactivity tends to increase with advancing age, exhibits greater rates among women, and is more pronounced in high-income nations [6]. One prevalent barrier to physical activity is a demanding schedule, ascribed to occupational and familial obligations, including job engagements, domestic tasks, and childcare duties. Therefore, it is crucial to integrate uncomplicated and efficient physical activity into demanding daily routines to surmount the obstacles above and enhance general well-being.
Engaging in outdoor walking is a convenient and straightforward way to incorporate physical activity into a busy daily routine. Previous studies have suggested that aerobic walking may offer benefits for bone health by reducing bone turnover markers, preventing bone loss, and preserving bone mineral density (BMD) [7,8,9]. However, conflicting results have been reported in meta-analyses of both randomized and non-randomized controlled trials [10,11,12,13]. Some meta-analyses indicate a limited or negligible effect of walking on specific BMD sites [10,11,12,13]. This discrepancy underscores the need for further research to clarify the relationship between outdoor walking and bone metabolism in older adults. By unraveling these associations, we can develop targeted interventions and recommendations to enhance bone health and overall well-being in older adults.
The etiology of osteoporosis in older adults is often attributed to the intricate interplay between lifestyle factors and genetic variations. Those with high hereditary risk and those with low levels of physical exercise are associated with increased susceptibility to developing osteoporosis [14,15,16]. Nevertheless, little research has been conducted on whether the correlation between daily outdoor walking and the incidence of osteoporosis in older adults is influenced by genetic susceptibility to osteoporosis. Our research aims to elucidate the potential correlation between regular outdoor walking and a susceptibility to osteoporosis. Additionally, we want to investigate the potential influence of genetic predisposition to osteoporosis on this relationship.
Methods
Study design and population
Our Kunshan Cohort consisted of 50,000 participants prospectively recruited across eight community health service centers within the Kunshan between 2014 and 2023. This cohort is based on a class A tertiary hospital of Kunshan, with the partner university, the Kunshan Health and Family Planning Information Center, primary hospitals, and community health service centers. The data of the Kunshan cohort were from the electronic health records (EHR), which were recruited from the annual health examinations of all older adults in Kunshan [17,18,19]. The genotyoing data were extracted from the residual blood samples after health examination [17,18,19]. Kushan’s local hospital’s research ethics committee approved conducting this investigation, with informed consent obtained from all participating individuals.
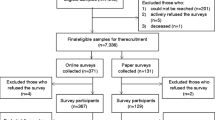
Due to the restricted number of participants from 2014 to 2017 and the absence of long-term follow-up for participants recruited in the Kunshan cohort between 2022 and 2023, an initial inclusion of 49,513 participants from the Kunshan cohort between 2017 and 2021 was made. Participants who were younger than 60 years old (n = 12,815), had pre-existing osteoporosis at the beginning of the study (n = 2,769), did not have follow-up data (n = 1,513), or had missing data on biochemical markers (n = 591) were eliminated from the analysis. In addition, those who engaged in activities other than outdoor walking (n = 4,631) and those who participated in outdoor walking exercise but did not engage in daily outdoor walking (n = 2,494) were subsequently eliminated from the analysis. The current study comprised 24,700 participants (Figure S1).
Exposure
The data about individuals' daily outdoor walking habits was obtained via a face-to-face questionnaire. Participants were asked a specific series of questions, including the inquiry: "Have you participated in any physical activities within the previous year with the intention of enhancing your overall well-being?" Participants who responded “yes” were classed as exercisers, while those who responded “no” were labeled non-exercisers. Participants who responded favorably were then asked to provide further information on their primary exercise preference during the previous year. The specific question posed was, "What has been your most significant mode of physical activity?" If the answer indicated engagement in low-intensity outdoor walking, individuals were next queried about the frequency of their low-intensity outdoor walking activities during the previous month. The range of responses included 0–7 days each week. In instances where the response indicated a frequency of 7 days per week, participants were asked the following question to ascertain the mean duration of daily outdoor walking: "Over the previous month, what was the average duration (in minutes) of your daily outdoor walking activities?" In this study, the researchers categorized the duration of daily outdoor walking into four groups. The first group consisted of individuals who did not engage in outdoor walking (n = 16,491). The second group included individuals who engaged in daily outdoor walking for ≤ 30 min (n = 3,840). The third group consisted of individuals who engaged in daily outdoor walking for > 30 min but ≤ 60 min (n = 3,814). Lastly, the fourth group included individuals who engaged in daily outdoor walking for > 60 min (n = 555).
Osteoporosis ascertainment
Table S1 presents the criteria for prevalent and incident osteoporosis. The identification of prevalent osteoporosis was conducted using many data sources, including outpatient records, self-reported medical history, prescription information, and imaging procedures for BMD, such as B-mode ultrasonography and dual-energy X-ray absorptiometry. Incident osteoporosis cases were diagnosed using particular codes from the International Classification of Diseases 10th edition (ICD-10). These codes, namely M80, M81, and M82, were used to identify and document cases in the outpatient records of the community health care center, which were connected to the EHR database for Kunshan [20,21,22,23,24]. This research used data from the community health care center from January 1, 2017, to December 31, 2021.
Covariates
Covariates, like sex, age, health and medical history, and educational attainment, were obtained through face-to-face questionnaires during the baseline recruitment. During the first assessment visit, height, weight, and waist circumference were assessed by trained nurses. The BMI was computed by dividing an individual's weight by the square of their height in meters. Data regarding smoking, alcohol intake, hypertension, diabetes mellitus (DM), dyslipidemia, stroke, coronary artery disease (CAD), cancer, depression, calcium and vitamin D supplementation, and hormone medication was routinely obtained as part of the participants’ health and medical history during the baseline recruitment. Detailed information regarding calcium and vitamin D supplementation and hormone medication is presented in Table S2, Table S3, and Table S4, respectively. The calculation of the genetic risk score (GRS) for osteoporosis was conducted using 14 single-nucleotide polymorphisms (SNPs) that have been previously identified as being linked to osteoporosis in genome-wide association studies of fractures, as outlined in prior research conducted inside the UK Biobank [14]. Table S5 presents comprehensive data about the 14 specific SNPs chosen for analysis. An elevated GRS was associated with an increased susceptibility to osteoporosis. The distribution of osteoporosis-GRS in the Kunshan Cohort is shown in Figure S2. The duration of the follow-up period was determined by calculating the time elapsed from the initial recruiting date to the earliest occurrence of three events: being lost to follow-up, experiencing death, or reaching the censoring date (December 31, 2021).
Statistical analysis
The continuous data were reported using either the mean plus standard deviation (SD) or the median with the interquartile range (IQR). Categorical data was represented using numerical values, specifically numbers (n) and percentages (%), to describe its features. To compare participants who engage in daily outdoor walking for varying durations, we employed a one-way analysis of variance (ANOVA) for continuous data and either c2 or Fisher's exact tests for categorical data. The study utilized Cox regression models to evaluate the correlation between outdoor walking and the occurrence of osteoporosis. The findings were reported in hazard ratios (HRs) accompanied by 95% CIs. Among Cox regression analysis, the duration of daily outdoor walking was treated as a categorical variable, with four distinct categories: none (indicating no outdoor walking), ≤ 30 min/day, > 30 but ≤ 60 min/day, and > 60 min/day. Each statistical model's reference category was set as "none" (i.e., no outdoor walking). The study employed restricted cubic spline regression analysis to examine the potential dose–response association between the continuous variable of daily outdoor walking duration (as opposed to duration categories) and the progression of osteoporosis.
The multivariable models sequentially evaluated the subsequent covariates: No modifications were made to Model 1. Model 2 was updated to account for demographic variables, smoking behavior, alcohol consumption, the presence of comorbidities, calcium and vitamin D supplementation, as well as hormone prescription. Model 3 was additionally altered to include osteoporosis-GRS, the first 10 primary components of ancestry, and genotype measurement batches. In Model 3, the analysis was conducted with a sample size of 13,426 participants, as 11,274 participants lacked the GRS.
To investigate the potential influence of genetic predisposition on the relationship between outdoor walking and the incidence of osteoporosis, we performed stratified analyses, which involved dividing people into groups based on the dichotomies of osteoporosis-GRS. Multiple secondary analyses were conducted. Initially, we performed stratified analyses to investigate the correlations between daily outdoor walking and occurrences of osteoporosis events, considering various factors, such as demographic data, smoking status, drinking status, comorbidities, calcium and vitamin D supplementation, and hormone medication. The joint test investigated the interactions between outdoor walking and the specified subgroups. Furthermore, a series of sensitivity analyses were performed in which subjects with hypertension, CAD, DM, stroke, cancer, depression, and dyslipidemia at baseline were systematically excluded in each replication. In addition, sensitivity analyses systematically eliminated participants taking calcium supplements and vitamin D supplements at baseline in each iteration. Besides, those undergoing hormone treatment were deliberately omitted from the study sample. Subsequently, the primary analyses were repeated to mitigate the potential influence of reverse causality. Furthermore, we conducted separate primary analyses for men and women.
The statistical analyses were conducted using R Statistics version 4.0.2, developed by the R Foundation. A significance level of p < 0.05 was employed for all statistical tests, with two-sided testing being utilized.
Results
Baseline characteristics
A total of 24,700 participants were included in the study, with a mean age of 68.4 ± 5.8 years. Of these participants, 51.9% were women. Among the participants, 16,491 reported no outdoor walking, 3,840 reported walking for ≤ 30 min/day, 3,814 reported walking for > 30 but ≤ 60 min/day, and 555 reported walking for > 60 min/day (Table 1). Individuals with a longer duration of outdoor walking were found to have a higher likelihood of having a higher BMI, larger waist circumference, and higher educational attainment than others without outdoor walking. They were also more likely to have prevalent DM and were less likely to be female or have prevalent depression. Furthermore, they were less likely to use calcium supplements and hormone medication at the baseline assessment.
Association between outdoor walking and osteoporosis incidence
Over 37.3 months, a total of 4,586 cases of osteoporosis were recorded. The incidence of osteoporosis per 100 individuals exhibited a sequential decrease with increasing duration of daily outdoor walking, with rates of 19.67, 18.65, 14.94, and 10.09, respectively. In the Cox regression analyses, it was discovered that there was a negative association between outdoor walking and the incidence of osteoporosis (Table 2). In the unadjusted model (Model 1), the HRs for different durations of daily outdoor walking were compared to the reference group (no outdoor walking). The HRs were 0.95 (95% CI: 0.87–1.03), 0.80 (95% CI: 0.73–0.88), and 0.54 (95% CI: 0.41–0.70) for individuals who walked for ≤ 30 min, > 30 but ≤ 60 min, and > 60 min/day, respectively (p for trend < 0.001). In Model 3, the risks associated with outdoor walking for osteoporosis were examined after adjusting for all relevant factors. Compared to the reference group (individuals who did not engage in outdoor walking), the HRs for osteoporosis were found to be 1.03 (95% CI: 0.91–1.16), 0.83 (95% CI: 0.72–0.95), and 0.60 (95% CI: 0.39–0.92) for individuals who walked for ≤ 30 min/day, > 30 but ≤ 60 min/day, and > 60 min/day, respectively. These findings were consistent with the results obtained from the statistical analysis of other models (Table 2). Furthermore, the adjusted restricted cubic spline regression analysis showed that the incidence of osteoporosis decreased with increasing the duration of daily outdoor walking (Fig. 1).

Associations between daily outdoor walking time and incidence of osteoporosis (estimates are from the restricted cubic spline regression analysis adjusted for demographic data, smoking status, drinking status, comorbidity, and medication use)
Association between outdoor walking and osteoporosis incidence among participants with different osteoporosis-GRS
An increase of one SD in osteoporosis-GRS was linked with a 44% increase in the probability of developing osteoporosis, with a 95% CI ranging from 1.18 to 1.77 (Table S6). In comparison to the reference group (individuals who did not engage in outdoor walking), individuals who walked for > 30 but ≤ 60 min/day exhibited a 25% (95% CI: 0.61–0.91) decreased risk of osteoporosis in individuals with a low osteoporosis-GRS (Table 3). In contrast, no statistically significant correlation was found among individuals with a high osteoporosis-GRS who engaged in outdoor walking for varying durations, as compared to the reference group that did not engage in outdoor walking (Table 3). Moreover, the adjusted restricted cubic spline regression analysis revealed that an increase in the duration of daily outdoor walking was associated with a decreasing trend in the risk of osteoporosis among individuals with both low and high genetic risk (Fig. 2).

Associations between daily outdoor walking time and incidence of osteoporosis by osteoporosis-genetic risk score group (estimates are from the restricted cubic spline regression analysis adjusted for demographic data, smoking status, drinking status, comorbidity, medication use, the first 10 primary components of ancestry, and genotype measurement batches)
Secondary analyses
In our stratified analyses, we found that the relationship between outdoor walking and the risk of osteoporosis was more pronounced in individuals without hypertension, individuals who did not take calcium supplements (p for interaction < 0.001, = 0.031, respectively) (Table S7). The sensitivity analyses assessed the impact of successively excluding participants with comorbidities at baseline, including hypertension, CAD, DM, stroke, cancer, depression, and dyslipidemia. Despite these exclusions, the observed effect of outdoor walking on osteoporosis occurrences remained consistent and reliable (Table S8). The sensitivity analyses, which sequentially excluded participants who were taking vitamin D and calcium supplements at the beginning of the study, were similar to the main analyses (Table S9). Similar findings were observed in sensitivity analyses that removed participants using hormone therapy (Table S10). After limiting the scope of our analysis to male participants, we observed that the correlation between outdoor walking and the incidence of osteoporosis remained statistically significant (Table S11). Upon limiting our analyses to female participants, we identified a noteworthy correlation between engaging in outdoor walking and the occurrence of osteoporosis among those who walked for > 30 min per day (Table S12).
Discussion
This research included a substantial sample size of 24,700 participants from the Kunshan cohort to investigate the correlation between outdoor walking, genetic susceptibility, and the likelihood of developing osteoporosis. Compared to those who did not engage in outdoor walking, those who engaged in regular outdoor walking had a reduced risk of osteoporosis, ranging from 17 to 40% after accounting for any confounding factors. The association showed a downward trend among individuals with low osteoporosis-GRS. Additionally, among individuals with a high osteoporosis-GRS, those walking for > 60 min per day had the lowest chance of developing osteoporosis.
This is the first large-scale study of whether or not regular outdoor walking decreases the risk of osteoporosis in the older adults. Existing research on the influence of walking on bone health presents conflicting findings. In a 12-month prospective study conducted in Tokyo, Japan, postmenopausal women with osteopenia/osteoporosis who engaged in daily outdoor walking demonstrated significant increases in lumbar (L2-L4) BMD. This was accompanied by reductions in urinary cross-linked N-terminal telopeptides of type I collagen levels and serum bone-specific alkaline phosphatase levels compared to a control group [7]. Additionally, a randomized controlled trial indicated that short-term (7 months) walking exercise with intensity above the anaerobic threshold effectively increased lumbar vertebrae BMD and decreased urinary calcium levels, suggesting the safety and efficacy of walking in preventing postmenopausal bone loss [8]. Another study illustrated that moderate-intensity treadmill walking exercise could lower bone resorption and bone turnover markers in menstruating women and menopausal women [9]. Conversely, a meta-analysis reported a significant positive effect of walking on lumbar BMD but not on the femur or calcaneus [10]. Another meta-analysis revealed that regular walking did not significantly impact BMD preservation in the spine of postmenopausal women, while displaying notable positive effects at the femoral neck [11]. Furthermore, a systematic review and meta-analysis highlighted that as a singular exercise therapy, walking showed no significant effects on BMD at the lumbar spine, radius, or for the whole body in perimenopausal and postmenopausal women. However, it did demonstrate significant and positive effects on femoral neck BMD in this population with duration exceeding 6 months [12]. Another systematic review and meta-analysis provided low-certainty evidence suggesting that physical activity had minimal impact on areal BMD at the total hip and little to no influence on areal BMD at the femoral neck, lumbar spine, and whole body [13]. However, previous studies were short-term results, the exercise of walking is an endurance exercise that requires long-term persistence, an insufficient dosage may not achieve adaptive changes. To date, no longitudinal population-based studies have reported long-term association between outdoor walking and incident osteoporosis. We first reported that a longer duration of daily outdoor walking was associated with a reduced risk of osteoporosis. This association persisted even after accounting for a wide range of confounding factors, such as demographic data, smoking status, alcohol consumption, comorbidities, medication use, and genetic predisposition to osteoporosis. While limited studies have explored the relationship between the daily outdoor walking duration of older adults and the incidence of osteoporosis, a randomized controlled study in 2012 investigated the association between T'ai-Chi practice and bone health in a group of 86 postmenopausal women aged 45–70 [25]. T'ai-chi was reported to increase bone production indicators, improve BMD in the femoral neck, and reduce the risk of osteoporosis [25]. Although the exercise methods are different, they are both low-intensity aerobic exercises, and highlight the relevance and need of incorporating simple exercise into daily life to increase physical activity levels and provide benefits for bone health.
Our research findings indicate a less pronounced association between engaging in outdoor walking and the susceptibility to osteoporosis among individuals with a high osteoporosis-GRS, as opposed to those with a low osteoporosis-GRS. The results of this study align with previous prospective cohort studies conducted on diabetes, another common metabolic disorder [25, 26]. These studies have also observed a notable interaction between physical activity and diabetes-GRS on the incidence of diabetes. At the same time, this interaction indicates that the prospective impact of physical activity may be less pronounced in individuals with a higher genetic risk for the disease [25, 26]. According to our research findings, among individuals with a high genetic predisposition to osteoporosis, the effect of daily outdoor walking duration on osteoporosis risk is smaller. At the same time, we found that among the older adults who consistently engage in outdoor walking, there is a higher level of education. However, they also exhibit higher BMI values, larger waist circumferences, and a higher incidence of diabetes. We believe this phenomenon may be related to the fact that Kunshan is located in an economically developed area. As a region that has long ranked as the top county-level city in China, Kunshan has a fast-paced lifestyle and high levels of competition. Individuals with higher education levels in this area often engage in intellectual activities and sedentary office work during their younger years, leading to a lack of time and opportunities for physical exercise, resulting in overweight body types, larger waist circumferences, and increased susceptibility to diabetes. Nevertheless, as these individuals age and enter retirement, they have more leisure time available and begin to recognize the importance of exercise for health. Consequently, they are more willing and have greater opportunities to participate in physical activities to improve their physical health and promote overall bodily balance. This may explain the seemingly contradictory results observed in our study. Furthermore, this transition and adjustment to a more active lifestyle partly reflect the correlation between life stages and health awareness. The present research also identified a correlation between the duration of daily outdoor walking and the likelihood of acquiring osteoporosis, specifically among those who do not have hypertension. Hypertension is a widespread chronic condition that has been acknowledged as a risk factor for the development of osteoporosis [27]. The findings of a retrospective research, including a sample size of 1,332 individuals, indicated a statistically significant association between hypertension and BMD. Specifically, the observed correlation between these two variables was negative (r = -0.28, p < 0.001) [28]. In addition, hypertension was associated with a shorter duration of daily outdoor walking in this study (median 40.0 vs. 60.0 min/day, p < 0.001). Furthermore, the relationship between outdoor walking and osteoporosis incidence was also observed among participants without calcium supplements. Calcium supplements are widely used, protecting against loss of bone density, and it has been recognized as protective factors for osteoporosis. A longitudinal study of 1,490 women found that the absence of calcium supplement usage is associated with lower levels of femoral neck BMD (median 0.92 vs. 0.96 g/cm2) and lumbar spine BMD (median 1.05 vs. 1.07 g/cm2) (p < 0.001, and 0.003, respectively) [29]. Moreover, the findings of a cross-sectional analysis indicate that exercise is a significant and independent factor in reducing the incidence of osteoporosis in both men and women [30]. When analyzing the impact of daily exercise on the incidence of osteoporosis in men and women individually, it was seen that the association was more significant in men. The adjusted odds ratio for men was 0.63, whereas for women it was 0.88 [31]. This finding aligns with our empirical findings that the correlation between outdoor walking activities and the susceptibility to osteoporosis is more pronounced among men. The potentially underlying mechanism to explain the above results is menopause, the most prominent difference between old-aged men and women in our analysis. Menopause in old women is characterized by the decline in ovarian function and the consequent decrease in estrogen levels, which disrupts the delicate balance between bone formation and resorption, leading to accelerated bone loss. In contrast, men do not experience the dramatic hormonal changes observed in women during aging, which may make them more responsive to exercise interventions. Significantly, our observations indicate that the correlation between outdoor walking and osteoporosis risk is more pronounced in men. This suggests that incorporating a routine of daily outdoor walking may serve as a viable intervention for mitigating osteoporosis in older men.
The precise pathogenic mechanisms that underlie the correlation between outdoor walking and bone metabolism and the consequences of osteoporosis remain uncertain. However, the reported connection between outdoor walking and a reduced risk of osteoporosis is significantly reasonable. Walking is classified as a form of moderate aerobic activity, which has been found to benefit bone mass by reducing bone turnover, bone resorption, and urinary calcium excretion. Therefore, engaging in regular outdoor walking has the potential to be a beneficial kind of physical activity for enhancing bone health [8]. The application of mechanical stress on the skeletal structure is a key mechanism for inducing bone formation during lower limb exercise. Consequently, engaging in regular lower limb exercise may potentially enhance bone density and strength. Indeed, engaging in outdoor walking as a prevalent, secure, and conveniently accessible daily physical activity resulted in beneficial alterations in bone metabolism. Several studies have demonstrated that walking notably impacts bone mineral content and areal BMD in young women [32]. Additionally, it has been found to elicit favorable improvements in knee muscle strength among women with low bone mass [33]. Furthermore, walking has effectively mitigated bone loss in postmenopausal women with pre-diabetes and non-alcoholic fatty liver disease, thereby reducing the likelihood of developing osteoporosis [34]. Engaging in walking has been found to potentially mitigate the likelihood of developing osteoporosis, as it has been observed to elevate serum ionized calcium levels while concurrently reducing parathyroid hormone and c-terminal telopeptide of type I collagen levels. These factors have been identified as being closely linked to the development of osteoporosis.
Engaging in outdoor walking is a readily accessible exercise that effectively sustains moderate intensity. In contrast to structured physical activities, such as formal training regimens, outdoor walking does not require specialized equipment, specific expertise, or specialized attire. Moreover, individuals who lack familiarity with exercise can readily engage in this activity with relative ease and success. Ultimately, unlike other physical activities, outdoor walking does not have temporal restrictions, which is a prevalent factor resulting in decreased involvement in alternative forms of physical exercise. This makes it a more accessible option for individuals with limited availability or scheduling constraints, thereby promoting higher levels of engagement. Therefore, outdoor walking is highly recommended for older adults as a preventive against osteoporosis.
The present study possesses multiple notable strengths. The utilization of a prospective design, large sample size, implementation of a long-term follow-up period spanning 37.3 months, and utilization of high-quality data derived from the Kunshan cohort are advantageous factors. These factors enable the consideration of a wide range of confounding variables and ensure enough statistical power. Moreover, the study cohort primarily consisted of individuals aged 60 years and older from the Kunshan community, ensuring homogeneity among the participants. Furthermore, the GRS for osteoporosis was computed using a set of 14 SNPs recently identified in a thorough genome-wide association research. This enabled us to provide precise predictions regarding the genetic risk associated with this condition.
However, some limitations should be taken into account in the present study. Initially, data regarding the duration of daily outdoor walking was obtained by self-administered questionnaires, a method that is vulnerable to reporting bias. Furthermore, depending mainly on diagnosis codes for osteoporosis assessment, especially when individuals may not undergo dual-energy X-ray absorptiometry scans due to factors such as limited mobility, may diminish the likelihood of identifying osteoporosis. In addition, despite our comprehensive consideration of numerous confounding variables and the implementation of multiple sensitivity analyses, it is important to acknowledge that the inherent nature of observational research introduces the likelihood of remaining confounding and potential bias. Thirdly, the GRS demonstrates potential limitations when extrapolated to populations of diverse genetic backgrounds due to its development primarily in individuals of white British genetic origin. Furthermore, the participants in our study were exclusively selected from the Kunshan region and identified as members of the Han ethnic group. Consequently, it is imperative to perform additional research, including other geographical and ethnic groupings. Fifthly, our study primarily focuses on the impact of low-intensity outdoor walking on the incidence of osteoporosis in the older adults. Subsequent research is necessary to further explore the effects of outdoor walking at different intensities on the occurrence of osteoporosis. Lastly, although this real-world observational study strongly supports the beneficial effects of walking exercise on osteoporosis, causal inferences cannot be drawn.
Conclusion
The findings of our study indicate that a longer duration of daily outdoor walking is correlated with a reduced risk of osteoporosis, particularly among older adults with a low genetic propensity to develop the condition. While our research has demonstrated a correlation between walking and bone health, it is crucial to recognize that walking can serve as an indicator for other beneficial activities and lifestyle factors. Therefore, we suggest incorporating walking as a part in the promotion of overall bone health. Consequently, it is advisable to consider additional beneficial activities and lifestyle factors, such as nutrition, resistance training, and weight-bearing exercises, alongside the encouragement of walking, to effectively maintain optimal bone health.
Data availability
Data from the Kunshan cohort is available to researchers under reasonable access. Requests to access this cohort should be directed to Zhou Kaixin’s Research Group in Guangzhou Laboratory.
References
Cauley JA, Giangregorio L (2020) Physical activity and skeletal health in adults. Lancet Diabetes Endocrinol 8:150–162. https://doi.org/10.1016/S2213-8587(19)30351-1
Wang L, Yu W, Yin X et al (2021) Prevalence of osteoporosis and fracture in China: the China osteoporosis prevalence study. JAMA Netw Open 4:e2121106. https://doi.org/10.1001/jamanetworkopen.2021.21106
Si L, Winzenberg TM, Jiang Q et al (2015) Projection of osteoporosis-related fractures and costs in China: 2010–2050. Osteoporos Int 26:1929–1937. https://doi.org/10.1007/s00198-015-3093-2
Gignac MA, Cott C, Badley EM (2000) Adaptation to chronic illness and disability and its relationship to perceptions of independence and dependence. J Gerontol B Psychol Sci Soc Sci 55:P362-372. https://doi.org/10.1093/geronb/55.6.p362
World Health Organization (2010) Global recommendations on physical activity for health. Geneva. https://www.ncbi.nlm.nih.gov/books/NBK305057/
Hallal PC, Andersen LB, Bull FC et al (2012) Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet 380:247–257. https://doi.org/10.1016/S0140-6736(12)60646-1
Yamazaki S, Ichimura S, Iwamoto J et al (2004) Effect of walking exercise on bone metabolism in postmenopausal women with osteopenia/osteoporosis. J Bone Miner Metab 22:500–508. https://doi.org/10.1007/s00774-004-0514-2
Hatori M, Hasegawa A, Adachi H et al (1993) The effects of walking at the anaerobic threshold level on vertebral bone loss in postmenopausal women. Calcif Tissue Int 52:411–414. https://doi.org/10.1007/BF00571327
Kitareewan W, Boonhong J, Janchai S, Aksaranugraha S (2011) Effects of the treadmill walking exercise on the biochemical bone markers. J Med Assoc Thai 94(Suppl 5):S10-16
Palombaro KM (2005) Effects of walking-only interventions on bone mineral density at various skeletal sites: a meta-analysis. J Geriatr Phys Ther 28:102–107. https://doi.org/10.1519/00139143-200512000-00006
Martyn-St James M, Carroll S (2008) Meta-analysis of walking for preservation of bone mineral density in postmenopausal women. Bone 43:521–531. https://doi.org/10.1016/j.bone.2008.05.012
Ma D, Wu L, He Z (2013) Effects of walking on the preservation of bone mineral density in perim and postmenopausal women: a systematic review and meta-analysis. Menopause 20:1216–1226. https://doi.org/10.1097/GME.0000000000000100
Ashe MC, Santos IKD, Edward NY, et al (2021) Physical activity and bone health in men: a systematic review and meta-analysis. J Bone Metab 28:27–39. https://doi.org/10.11005/jbm.2021.28.1.27
Morris JA, Kemp JP, Youlten SE, et al (2019) An atlas of genetic influences on osteoporosis in humans and mice. Nat Genet 51:258–266. https://doi.org/10.1038/s41588-018-0302-x
Ralston SH, Uitterlinden AG (2010) Genetics of osteoporosis. Endocr Rev 31:629–662. https://doi.org/10.1210/er.2009-0044
Chilibeck PD, Vatanparast H, Cornish SM et al (2011) Evidence-based risk assessment and recommendations for physical activity: arthritis, osteoporosis, and low back pain. Appl Physiol Nutr Metab 36(Suppl 1):S49-79. https://doi.org/10.1139/h11-037
Liu Y, Pan Y, Tian Z et al (2023) Association of mitochondrial DNA copy number with chronic kidney disease in older adults. BMC Geriatr 23:514. https://doi.org/10.1186/s12877-023-04203-7
Wu P, Liu Z, Tian Z et al (2023) CYP2C19 loss-of-function variants associated with long-term ischemic stroke events during clopidogrel treatment in the Chinese population. Clin Pharmacol Ther 114:1126–1133. https://doi.org/10.1002/cpt.3028
Chen F, Pan Y, Liu Z et al (2022) Impact of visit-to-visit triglyceride-glucose index variability on the risk of cardiovascular disease in the elderly. Int J Endocrinol 2022:5125884. https://doi.org/10.1155/2022/5125884
Kwon MJ, Park JY, Kim SG et al (2022) Potential association of osteoporosis and not osteoporotic fractures in patients with gout: a longitudinal follow-up study. Nutrients 15:134. https://doi.org/10.3390/nu15010134
Jung S, Han S, Kwon H-Y (2018) Dose-intensity of bisphosphonates and the risk of osteonecrosis of the jaw in osteoporosis patients. Front Pharmacol 9:796. https://doi.org/10.3389/fphar.2018.00796
Argesanu RD, Armean P, Georgescu D, et al (2022) Challenges in utilization of osteoporosis healthcare services during COVID-19 pandemic in Romania – a nationwide population study. Maedica (Bucur) 17:253–258. https://doi.org/10.26574/maedica.2022.17.2.253
Kim SY, Yoo DM, Kwon MJ et al (2022) Increased risk of temporomandibular joint disorder in osteoporosis patients: a longitudinal study. Front Endocrinol (Lausanne) 13:835923. https://doi.org/10.3389/fendo.2022.835923
Kim E-S, Kim C (2021) The association between continuity of care and surgery in lumbar disc herniation patients. Sci Rep 11:5550. https://doi.org/10.1038/s41598-021-85064-1
Wayne PM, Kiel DP, Buring JE et al (2012) Impact of Tai Chi exercise on multiple fracture-related risk factors in post-menopausal osteopenic women: a pilot pragmatic, randomized trial. BMC Complement Altern Med 12:7. https://doi.org/10.1186/1472-6882-12-7
Wu Y, Luo M, Tan X, Chen L (2022) Stair climbing, genetic predisposition, and the risk of incident type 2 diabetes: a large population-based prospective cohort study. J Sport Health Sci 12:158–166. https://doi.org/10.1016/j.jshs.2022.10.002
Chai H, Ge J, Li L et al (2021) Hypertension is associated with osteoporosis: a case-control study in Chinese postmenopausal women. BMC Musculoskelet Disord 22:253. https://doi.org/10.1186/s12891-021-04124-9
AI-Hariri M, Aldhafery B (2020) Association of hypertension and lipid profile with osteoporosis. Scientifica (Cairo) 2020:7075815. https://doi.org/10.1155/2020/7075815
Bailey RL, Zou P, Wallace TC et al (2020) Calcium supplement use is associated with less bone mineral density loss, but does not lessen the risk of bone fracture across the menopause transition: data from the study of women’s health across the nation. JBMR Plus 4:e10246. https://doi.org/10.1002/jbm4.10246
Yang C-Y, Lai JC-Y, Huang W-L, et al (2021) Effects of sex, tobacco smoking, and alcohol consumptionosteoporosis development: evidence from Taiwan biobankparticipants. Tob Induc Dis 19:1–8. https://doi.org/10.18332/tid/136419
Shin CS, Choi HJ, Kim MJ et al (2010) Prevalence and risk factors of osteoporosis in Korea: a community-based cohort study with lumbar spine and hip bone mineral density. Bone 47:378–387. https://doi.org/10.1016/j.bone.2010.03.017
Kato T, Tomioka T, Yamashita T et al (2020) Nordic walking increases distal radius bone mineral content in young women. J Sports Sci Med 19:237–244
Ossowski ZM, Skrobot W, Aschenbrenner P et al (2016) Effects of short-term Nordic walking training on sarcopenia-related parameters in women with low bone mass: a preliminary study. Clin Interv Aging 11:1763–1771. https://doi.org/10.2147/CIA.S118995
Du X, Zhang C, Zhang X et al (2021) The Impact of Nordic walking on bone properties in postmenopausal women with pre-diabetes and non-alcohol fatty liver disease. Int J Environ Res Public Health 18:7570. https://doi.org/10.3390/ijerph18147570
Acknowledgements
The authors would like to acknowledge all Kunshan cohort participants and staff for their contributions to the health of mankind.
Funding
This study is supported by the National Key Research and Development Program of China (Grant/Award Number: 2020YFC2006100), China Postdoctoral Science Foundation (Grant/Award Number: 2022M711439), Elderly Health Research Project of Jiangsu Province (Grant/Award Number: LKZ2022020), Suzhou Key Clinical Diagnosis and Treatment Technology Project (Grant/Award Number: LCZX202024), Suzhou Collaborative Innovation Research Project of Medical and Industrial Integration (Grant/Award Number: SLJ2022023), Medical Education Collaborative Innovation Fund of Jiangsu University (Grant/Award Number: JDYY2023058), Kunshan Innovation Capacity Building Program (Grant/Award Number: KZ2023005), Kunshan Science and Technology Program of Social Development (Grant/Award Number: KSZ2301), Key Project of Guangren Foundation Research Program (Clinical Research Specialization) at Kunshan First People’s Hospital (Grant/Award Number: KRY-YN2022003). The funders of the study had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
Chong Li, and Kai-Xin Zhou conceived and designed the study, analyzed and interpreted data, and revised the manuscript; Yu-Shan Yue and Yang Liu analyzed and interpreted data, drafted the manuscript and revised the manuscript; Ke Lu and Qin Shi revised it critically. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. All authors have read and approved the final version of the manuscript, and agree with the order of presentation of the authors.
Corresponding authors
Ethics declarations
Ethics statement
The study protocol was established, according to the ethical guidelines of the Helsinki Declaration and was approved by the ethics committee of a class A tertiary hospital of Kunshan. Informed consent of all participants has been obtained (IEC-C-007-A07-V3.0).
Sponsor’s role
The funders had no input into the conduct of the study and the interpretation of results.
Conflicts of interest
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Highlights
We certify that this work is novel for the following reasons. Firstly, it is the largest prospective cohort study demonstrating the long-term association between daily outdoor walking duration and osteoporosis risk among older adults. Secondly, it is the first study which reported whether association between daily outdoor walking duration and osteoporosis risk among older adults was affected by genetic variants. Thirdly, through a large, homogeneous prospective cohort, a significant association between longer duration of daily outdoor walking and reduced osteoporosis risk was found among older adults, particularly among older adults with a low genetic predisposition to osteoporosis.
Why does this paper matter?
Outdoor walking is a simple and cost-effective adjunct exercise method that can be easily incorporated into busy daily life. This study indicates that longer duration of daily outdoor walking is suitable for preventing osteoporosis, especially in older adults with low genetic predisposition to osteoporosis.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Yue, YS., Liu, Y., Lu, K. et al. Outdoor walking, genetic predisposition, and the risk of incident osteoporosis among older adults: A prospective large population-based cohort study. Osteoporos Int (2024). https://doi.org/10.1007/s00198-024-07122-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00198-024-07122-4