
Abstract
Summary
This study describes the development of a decision aid (DA), aimed at supporting patients in their decision whether to start anti-osteoporosis medication. People with recent fractures or osteoporosis and health professionals were supportive of the DA initiative. An experimental study been started to assess (cost-)effectiveness of the DA.
Purpose
At fracture liaison services (FLS), patients with a recent fracture ánd osteoporosis or a prevalent vertebral fracture are advised to start anti-osteoporosis medication (AOM). This study describes the development of a decision aid (DA) to support patients and healthcare providers (HCPs) in their decision about whether to start AOM.
Methods
The DA was developed according to International Patient Decision Aid Standards (IPDAS). A systematic procedure was chosen including scope, design, prototype development, and alpha testing. A previously developed DA for women with osteoporosis was used as a basis. Furthermore, input from literature searches, the Dutch guideline on management of osteoporosis, and from people with a fracture or osteoporosis was used. The updated DA was evaluated during alpha testing.
Results
The DA facilitates the decision of patients whether to initiate AOM treatment and provides information on fractures and osteoporosis, general risk factors that increase the likelihood of a subsequent fracture, the role of lifestyle, personalized risk considerations of a subsequent fracture with and without AOM treatment, and AOM options and their characteristics in an option grid. Alpha testing with 15 patients revealed that patient preferences and needs were adequately presented, and several suggestions for improvement (e.g. adding more specific information, simplifying terminology, improving icon use) were accounted for. Participants from the alpha testing recommended use of the DA during outpatient visits.
Conclusion
Professionals and persons with osteoporosis were supportive of the proposed DA and its usability. The DA could help in a shared decision-making process between patients and HCPs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Over past decades, major advances have been made in the effectiveness of treating osteoporosis or fragility fractures. However, a substantial treatment gap exists between recommended anti-osteoporosis medication (AOM) and the actual prescription initiation or patient adherence. Defined as the percentage of eligible individuals not receiving treatment with anti-osteoporosis medication, the treatment gap actually increased in Europe from 55% in 2010 to 71% in 2019 [1, 2]. Furthermore, only between 17 and 75% of patients eligible for treatment are adherent 1 year after initiation [3].
Medication non-adherence is multidimensional (comprising initiation, implementation, or persistence) and multifactorial. Non-adherence can be condition-related (e.g. polypharmacy and medical history), patient-related (e.g. lower education levels, lack of perceived benefits of therapy), therapy-related (e.g. medication side effects, complex medication administration instructions, and medication regimens), health system-based (e.g. fragmented care and lack of patient education and support services), and related to socio-economic factors (e.g. lower income level and lack of medical insurance coverage) [4]. Among the factors contributing to non-adherence, insufficient information and unaddressed patient values and preferences are specifically important [5,6,7]. Shared decision-making (SDM) with decision aids (DAs) offers incorporation of best available evidence on benefits and harms of treatment options whilst simultaneously accounting for patients’ values and preferences through patient-centred care [6,7,8,9].
Fracture liaison services (FLS) have been developed and implemented to identify and evaluate patients who had a recent fracture and have osteoporosis or prevalent vertebral fractures. It is well known that these patients are at high risk for recurrent fractures and pre-emptive treatment is both highly successful and cost-effective [2, 10]. One of the challenges is the high proportion of patients who do not respond to their FLS invitation [11]. If patients do respond and are eligible for AOM, treatment initiation and medication adherence remain low. A study among Dutch patients visiting the FLS and eligible for AOM revealed between 60 and 72% do not initiate or adhere to AOM [2, 12]. FLS therefore represents an opportunity to substantially reduce the subsequent fracture risk by improving treatment uptake and adherence [2, 3, 6, 10]. By integrating SDM using DAs within FLS, high-quality decisions can be established, as patients are fully informed by facts and best available evidence on treatment options and can assimilate those facts into their needs, values, and preferences [13, 14].
In 2016, Hiligsmann et al. developed a 4-page DA for post-menopausal women with osteoporosis, addressing (i) information about osteoporosis and the individualized fracture risk, (ii) clarification of the decision that should be taken with an explanation of the risk of future fracture without medication treatment (natural course), (iii) explanation of the reduction in fracture risk when accepting medication treatment, and (iv) an overview summary (option grid) of first and second line treatment options with medication information such as mode and frequency of administration [15]. Overall, healthcare providers (HCPs) and patients expressed a positive attitude towards the intended use of the proposed DA [15]. However, for use in FLS, adjustments to this DA are required, as the risk of a subsequent fracture without medication (natural course) is much higher in patients with recent fractures and osteoporosis or vertebral fractures. Additionally, the DA for post-menopausal women with osteoporosis had not yet included the potential harms of AOM or option grid and there was no specific page to allow patients to deliberate on the choice or for expression of personal preference and deliberation. The need for a high-quality DA for use in the FLS was further motivated by a planned experimental study to evaluate effectiveness and cost-effectiveness of SDM using a DA combined with motivation interviewing [15, 16]. The aim of this study is to report on the development and usability of a DA in a Dutch FLS setting.
Methods
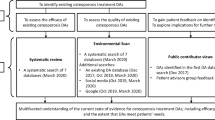
Updating and adjustment of the existing DA were performed in concordance with the updated International Patient Decision Aid Standards (IPDAS) and the recent Dutch guidelines on SDM [17,18,19,20]. Whilst the final version of the DA will be used in an experimental study (referred to as the ‘beta test’), this paper describes all steps except the beta testing. The key elements of the development and testing process are shown in Fig. 1.

Development model of our decision aid based on Witteman et al. [18] and role of steering group and patients. *The Beta testing is performed in an ongoing trial. HCP, healthcare professionals
Prior to initiating the scope phase, a steering group of ten persons was assembled, including HCPs (endocrinologists, rheumatologists, an osteoporosis nurse practitioner) and research experts (an epidemiologist, health technology assessment expert, implementation scientist, and a shared decision-making expert). We collaborated from the onset with the Dutch Osteoporosis Association (DOA), and had regular contact with the Associations’ chair to ensure the DA was aligned with their vision and mission. Although patients were not involved in the steering group, they were actively involved as participant or advisor at several stages of the study; in line with the IPDAS recommendations (Fig. 1) [17, 18].
Scope
From the outset, the SDM tool should support persons over the age of fifty (i) who had a recent fracture, (ii) attended the FLS, and (iii) had a treatment indication for AOM, in their decision to start AOM, and make lifestyle changes. In line with advices on SDM in the Netherlands, management options should follow the most recent Dutch management recommendations which contains general lifestyle recommendations as well as first and second line medication options for patient sub-groups [21]. The steering group agreed to develop a paper DA to be administered by an HCP during the FLS visit. A paper format was preferred by the steering group, as we learned from a previous developed DA that patients like to take the DA home, especially because it includes the notes by the HCP on personal risk factors, specific decision, and future appointment [22].
As a further context to the scope, unlike many other international osteoporosis treatment guidelines, the Dutch guideline advises anti-osteoporosis treatment in persons with osteoporosis and/or (prevalent) grade 3 (> 40% reduction in vertebral height) or grade 2 (25–40% reduction in vertebral height) vertebral fractures [23]. Finally, it is worth mentioning that in the Netherlands, FLS are run by qualified osteoporosis nurses that followed a 2-year specific training which ensures they are knowledgeable on fractures and osteoporosis and have the appropriate communication skills.
Design
The previously developed DA on AOM in post-menopausal women with osteoporosis served as a basis [16], although for FLS three aspects needed to be further clarified or adjusted: (a) the risk of subsequent fractures following a recent fracture, with or without initiation of AOM, (b) potential first and alternative medication options including potential barriers, such as treatment burden and risk of side effects, and (c) a section on formal deliberation on options and final decisions [15]. Several sources were identified to address these aspects, including (i) a systematic literature review (SLR) on the rate of subsequent fractures in patients with a recent fracture who did or did not visit FLS [24], (ii) the national Dutch guideline on osteoporosis and fracture prevention to identify medication options for the target population [21, 25], and (iii) a grey literature search to find DAs that provided examples of ways in which medication side effects can be presented and how personal preferences and values can be included in the final decision. The SLR was done to investigate the recurrent fracture rate in osteoporosis patients with recent fractures attending FLS and we used the fracture rate in the control group of studies with good quality as recurrence rate when no AOM would be started [24].
Furthermore, two focus groups were created with patients to understand their preferences about (i) communication of the potential harms of AOM and (ii) content of the section on final deliberation to start a specific treatment. Examples from DAs retrieved from the grey literature search were used to stimulate discussions. Information on the attributes/characteristics of the different AOMs to be included in the option grid had been collected in the context of the DA on post-menopausal osteoporosis [15]. Patients at risk of fractures were eligible to participate after attending a follow-up visit at the FLS of Maastricht University Medical Center (MUMC +), which serves as a regional and academic hospital. Efforts were made to include both males and females, and persons with diverse educational backgrounds. Oral informed consent was acquired. Due to time constraints only field notes were taken during the focus groups, which served as the basis to make adjustments in next steering group meetings. Results from focus group interviews were analyzed according to field notes. Before inclusion in the DA, information retrieved from the various sources was discussed repeatedly with HCPs who are involved in osteoporosis research and management.
Prototype
An initial prototype was developed by integrating the additional/updated information in the available DA. Prior to alpha testing, the prototype was piloted among three female medical support staff members.
Alpha testing
Alpha testing comprised readability, comprehensibility, and usability, and was assessed among (a) patients from the MUMC + and (b) members of the (lay) research panel of the Dutch Osteoporosis Association (DOA). Consecutive osteoporosis patients who attended the FLS for a follow-up visit after AOM initiation and agreed to participate in the individual interviews were included. The DOA chair invited the members of their panel of twenty experts by experience through our invitation and information letter. The first five persons that accepted the invitation received the DA and open-ended digital questionnaire for feedback. A digital questionnaire was chosen upon request by the Osteoporosis Society’s director. The intention was to include at least ten patients and at least five DOA members. This step was undertaken after adjusting the prototype based on feedback from the focus group patient interviews.
Interviews with patients from the FLS applied a cognitive debriefing approach and were executed by a research nurse and junior researcher (NR), who had been trained in interview methods. First, patients were asked to read each page of the DA prototype out loud and repeat the content of the page in his/her own words. Next, the interviewer asked about readability (difficult words or sentences) and comprehensibility of text and figures. At the end of the page-by-page debriefing, patients were asked whether the DA had improved their understanding of future fracture risk and the effect on this risk of both lifestyle changes and AOM. The patients were asked their opinion about the usability of several additional generic information folders. Following the open-ended questions, patients received a questionnaire and were asked to score five questions on amount of information, information clarity, design, patients’ comfort with decision responsibility, and DA recommendation on a 7-point Likert scale (1 being the lowest score and 7 being the highest). Interviews were audio-recorded and transcribed verbatim. Transcripts and field notes were summarized thematically per page and for the entire DA. After every three interviews, feedback from patients was discussed with at least two steering group members who decided whether and how to make changes. For major adjustments, agreement of the full steering group was sought.
The DOA members commented on the penultimate version (version 3) of the prototype. The DOA members were asked to score the same 7-point Likert scale questions and were invited in five open-ended questions to comment on overall readability, comprehensibility, and usability of the DA (Supplementary Table 1). Written comments were linked to the themes that had been identified in the patient interviews and new themes were added when applicable. In a final step, the steering group considered the remaining feedback and agreed on the final prototype.
Setting and ethical approval
This study was conducted in the Department of Internal Medicine, Division of Rheumatology at the MUMC + . The study was approved by the institutional review board from the MUMC + (2028–0507-A-10). All participants provided informed consent.
Results
Design
SLR on recurrent fracture rate
As part of the SLR, two retrospective studies described the risk of failing to treat recurrent fractures among patients older than 50 years, who suffered a recent fracture in the Netherlands [26, 27]. In line with the Dutch guideline on osteoporosis and fracture prevention, three DAs were developed depending on risk of recurrent fracture and the preferred first line AOM. The first DA applies to patients with a recent fracture that is not a ‘major’ fracture (i.e. not a hip, pelvis, or vertebral facture and not multiple fractures), indicating an intermediate risk for subsequent fractures (14% in the next 5 years) and for whom antiresorptives are recommended as first choice. The second DA is aimed to be used in patients with a major fracture (except for women with new or prevalent vertebral fractures), indicating a sub-group with a high subsequent fracture risk (25% in the next 5 years) and recommended to start antiresorptives as first choice treatment. The third DA was intended for women at high risk because of a major fracture including a new or prevalent vertebral fracture, for whom an anabolic agent is recommended as first choice of anti-osteoporosis treatment [21]. The treatment effectiveness displayed in all three DAs was 40% [8, 26].
Focus groups
Two focus groups revealed that patients preferred visualization of fracture risk with and without AOM by icon arrays, using broken bones over sad faces. Patients further agreed on the value of an option grid to provide an overview of AOM and information on benefits (i.e. effectiveness for the different fractures sites, medication administration, frequency, duration, and requirement of an HCP to administer the medication) and recommended to add information on potential harms (i.e. side effects and required precautions before and during treatment) to the option grid. For side effects, patients agreed they wanted to be informed on ‘common but less severe’ reactions (e.g. gastro-intestinal upset) as well as ‘rare but potentially severe’ side effects. For the final deliberation, patients demonstrated a preference for a simple interactive approach together with a specialized nurse guided by three questions: was the information provided clear, was additional information needed, and what was the final choice (whether to start with treatment or not, and if so, with which AOM). They liked information on the next steps (e.g. drug initiation, control visit) and on contact details for questions if anything were unclear before the new clinical visit/consultation.
Steering group
During the meetings of the steering group, it was emphasized the DA needed to be user-friendly, refrain from difficult medical terminology, and omit duplicate information. Suggestions were also given to balance the completeness of options whilst maintaining comprehensibility of their characteristics without too much detail (e.g. effectiveness, mode, and duration of administration).
Prototype
Each DA consisted of eight pages (Table 1). As an example, the third DA version can be found in Appendix 1. Wherever possible, text was accompanied by illustrative icons, e.g. the effect of medication on the risk of a subsequent fracture.
Alpha testing
The ten patients with an osteoporosis treatment indication who were recruited and who attended the FLS and five members of the DOA represented the population of interest (Supplementary Table 2). Of note, all participants had osteoporosis but one of the DOA members and one patient recruited from the FLS had not sustained a fracture. The FLS patient had a severely bruised finger, but revision of the X-ray could not confirm a fracture.
Figure 2 illustrates the answers to five usability questions asked of the patient group and DOA members per DA version. Overall, patients provided better scores compared to DOA members: patients were more satisfied, especially regarding the amount and clarity of the information (Fig. 2). Patients and DOA members recommended the use of this DA in clinical practice and scored this question the highest (7 versus 6.2). Of note, scores from the three last persons (in view of consecutive adjustment) demonstrated the highest scores, specifically increasing the most as more adjustments were made in response to the questions regarding design, patients’ comfort with decision responsibility, and DA recommendation. Interviewees often requested more detailed information, e.g. inclusion of physiotherapists in the region, inclusion of more rare health conditions as a risk factor for osteoporosis, specifications on lifestyle in relation to bone health.

Overview of results from five questions using a 7-point Likert scale, divided into a patient group (n = 10) and DOA members (n = 5). Results are illustrated with the mean per DA adaptation. Answers ranged on a scale from 1 to 7, with 1 being the lowest score and 7 being the highest. DA, decision aid; DOA, Dutch Osteoporosis Association
Table 2 summarizes the results of the open-ended questions for the patients and DOA member group per theme, per DA adjustment version. Overall, the content was clear to the patients and some of the DOA members (Supplementary Table 1). The option grid with AOM information was especially appreciated and well-understood. Except for the interpretation of the figures presenting the risk of recurrent fractures with and without medication, the overall layout and design was experienced as clear, easy to read, and eye-catching. All ten FLS patients and five DOA members experienced the DA as useful for outpatient visits and would recommend that it be used routinely. Main points of improvement highlighted by the patient group included clarification of difficult terms such as ‘calcium intake’ and ‘corticosteroids’, and consideration of visual impairments (e.g. colour blindness) with regard to the figures. For all these suggestions, adjustments were made (e.g. colours in the icon array were changed from red and green into red and blue). Most patients and two DOA members felt more detailed information was needed to understand illustrations such as the illustration on page one regarding the cross-section of the bone, or types of medication on page six with their side effects. This confirms that the DA should not be provided outside the clinical visits.
Other points of improvements for DOA members included the lack of information on the role of regional HCPs such as physiotherapists, inclusion of more extensive risk factors for fractures and osteoporosis (rare diseases), and additional information about medicines. With regard to extra information required on the role of specific diseases or lifestyle advice, the steering committee made a decision to limit the information, as most patients were already overwhelmed by the amount of information and HCPs can provide more details when needed. Contrary to persons participating in the focus groups, half of those participating in the alpha testing considered the page on deliberation as ‘scary’. This was likely a result of the context of the testing, where no real-life interaction could be simulated.
Discussion
This study reports on the development and usability of the DA by HCPs in the context of FLS for patients who have an indication for AOM and are over the age of 50. The strengths of this DA are its alignment with the new Dutch guideline on osteoporosis and fracture prevention, the involvement of relevant users (medical specialists, specialized nurses, the DOA members, and persons with a risk of fractures) and experts in shared decision-making, adherence to the IPDAS, and active involvement of patients throughout the process.
A challenge during the development related mainly to the data required to estimate the baseline risk of a subsequent fracture by recent fracture sufferers. Based on the Dutch guideline recommendations, three decision aids were created on the basis of future fracture risk and evidence of the effectiveness of treatment options (Appendix 2 illustrates the flowchart on selecting the most suitable DA for each patient) [21, 26]. Additional consultation with the specialized nurses indicated this would not be problematic in real life, as this distinction is representative of real practice. Along the same lines, communication of the rates of side effects was intensely discussed. The literature suggests a ‘best approach’ to communicate risk of side effects, chiefly because of the large differences in numeric literacy among patients [21, 26]. For this reason, and supported by patient preferences, the DA distinguishes between side effects that are ‘common but less severe’ and those that are ‘rare but potentially severe’.
All participants in the alpha testing recommended the usability of the DA in the FLS. They indicated that the preferences and needs of patients were adequately represented and emphasized the inclusion of lifestyle change as a strong point of the DA. During the initial interviews, a substantial number of textual enhancements were identified by patients and, due to subsequent adjustment, it was possible to evaluate these improvements during later interviews. Overall, DOA members were more demanding when answering questions about content, which is not surprising as they are trained to take a critical look at usual care. More often than patients, they suggested adding information on the potential diseases and causes underlying osteoporosis, and the need to change lifestyle behaviour by referral to HCPs such as physiotherapists to support behavioural change. However, the steering committee decided not to include such information, mainly to avoid diverting attention to aspects that are not within the scope of the DA. Importantly, our DA is professionally administered so that the specialized nurse is available to answer questions that might be appropriate or raised during consultation.
A systematic review and environmental scan performed by Paskins et al. analyzed the quality and effectiveness of osteoporosis treatment DAs [28]. At that time, there were only nine DAs available, all lacking several points of criteria later raised in the IPDAS development procedure. Despite this limitation, Paskins reported beneficial effects on decisional conflict, SDM, and accuracy of perceived fracture risk [28]. Our current DA is being tested at present in a trial including two hundred fifty patients from two Dutch FLS clinics and with adherence defined as an outcome [16]. As SDM alone is likely to be insufficient to ensure adherence, the trial will include motivational interviewing in the follow-up after 4 to 6 months, turning our intervention into a multi-component adherence intervention.
This study also has its limitations. The opinion of only one specialized osteoporosis nurse was included during the development of the DA. As we did not want to influence the opinion of the nurses before starting the intervention component of the ongoing trial, the opinion of the four osteoporosis nurses actively involved in the trial were not included in this development phase and their opinion will be identified during the process evaluation of the ongoing trial. Other limitations might be the lack of patient involvement as early as the steering group formation (IPDAS guidelines [17, 18]) but patients were actively involved in all other stages and had the opportunity to discuss all aspects of the DA. Furthermore, some patients are accustomed to the paternalistic model of the physician-patient relationship. This was also confirmed by previous studies [29, 30]. It should be noted that SDM is about collaborating with the patient to solve a problem; therefore, SDM should be considered with gradients that are congruent with patient values and preferences.
In addition, for the alpha testing, there was a difference in data collection methods between the two groups (patients were interviewed and received a survey, whilst DOA members only received a digital survey, albeit one more elaborate than the patients’ survey). These differences in collection methods probably contributed to discrepancies. As the DA was developed to be used as a HCP-administered tool, the more favorable feedback from those that had the face-to-face interview supports the importance of an administrator. To fully comprehend the feasibility and effects of the DA, the ongoing trial will report on the effectiveness and cost-effectiveness of the DA together with motivational interviewing [16]. Also, research should address difference in attitudes and preferences of persons towards SDM in order to enable decisions in line with (explicit/implicit) needs and preferences of these persons. Further limitations in the alpha testing were the relatively low sample size, partly related to COVID-pandemic, limiting generalizability, the lack of variation in ethnicity data, and use of educational level as surrogate for health literacy.
Before applying the DA in the FLS, nurses should be aware of the value of SDM and be trained in applying the DA during the clinical encounter. For the purpose of our ongoing trial, nurses will also apply the DA during a pilot study to identify and solve additional barriers and facilitators. This will include estimation of additional time for SDM. IT is well known that successful implementation of a DA will not only depend on the quality of the tool, but also on the support and self-efficacy of HCPs [31].
Conclusion
We established a DA specifically for Dutch osteoporosis patients who have an indication for AOM and are above the age of 50 through integration of patient needs and preferences, clinical expertise, user preferences, and iterative development. The tool’s utility during outpatient visits was recommended by patients, osteoporosis association members, and HCPs.
Data Availability
The data that supports the findings of this study are available on request from the corresponding author, LM. The data are not publicly available since they include information that might jeopardize the privacy of research participants.
References
Kanis JA, Norton N, Harvey NC, Jacobson T, Johansson H, Lorentzon M et al (2021) SCOPE 2021: a new scorecard for osteoporosis in Europe. Arch Osteoporos 16(1):82. https://doi.org/10.1007/s11657-020-00871-9
Borgström F, Karlsson L, Ortsäter G, Norton N, Halbout P, Cooper C et al (2020) Fragility fractures in Europe: burden, management and opportunities. Arch Osteoporos 15(1):59. https://doi.org/10.1007/s11657-020-0706-y
Fatoye F, Smith P, Gebrye T, Yeowell G (2019) Real-world persistence and adherence with oral bisphosphonates for osteoporosis: a systematic review. BMJ Open 9(4):e027049. https://doi.org/10.1136/bmjopen-2018-027049
Hiligsmann M, Cornelissen D, Vrijens B, Abrahamsen B, Al-Daghri N, Biver E et al (2019) Determinants, consequences and potential solutions to poor adherence to anti-osteoporosis treatment: results of an expert group meeting organized by the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO) and the International Osteoporosis Foundation (IOF). Osteoporos Int 30(11):2155–2165. https://doi.org/10.1007/s00198-019-05104-5
Montori VM, Shah ND, Pencille LJ, Branda ME, Van Houten HK, Swiglo BA et al (2011) Use of a decision aid to improve treatment decisions in osteoporosis: the osteoporosis choice randomized trial. Am J Med 124(6):549–556. https://doi.org/10.1016/j.amjmed.2011.01.013
Pencille LJ, Campbell ME, Van Houten HK, Shah ND, Mullan RJ, Swiglo BA et al (2009) Protocol for the Osteoporosis Choice trial. A pilot randomized trial of a decision aid in primary care practice. Trials 10:113. https://doi.org/10.1186/1745-6215-10-113
Scoville EA, de Leon Ponce, Lovaton P, Shah ND, Pencille LJ, Montori VM (2011) Why do women reject bisphosphonates for osteoporosis?. A videographic study. PLoS One 6(4):e18468. https://doi.org/10.1371/journal.pone.0018468
Cornelissen D, de Kunder S, Si L, Reginster JY, Evers S, Boonen A et al (2020) Interventions to improve adherence to anti-osteoporosis medications: an updated systematic review. Osteoporos Int 31(9):1645–1669. https://doi.org/10.1007/s00198-020-05378-0
Ralston KAP, Hauser B, Paskins Z, Ralston SH (2022) Effective communication and the osteoporosis care gap. J Bone Mineral Res 37(11):2049–54. https://doi.org/10.1002/jbmr.4701
Chadha M, Shingare A, Prasanth A, Chauhan P, Shah NF (2018) Fracture liaison service: prevention by coordination. Indian J Endocrinol Metab 22(6):719–721. https://doi.org/10.4103/ijem.IJEM_606_18
van den Berg P, van Haard PMM, Geusens PP, van den Bergh JP, Schweitzer DH (2020) Characterization of fracture liaison service non-responders after invitation by home visits and questionnaires. Osteoporos Int 31(10):2007–2015. https://doi.org/10.1007/s00198-020-05442-9
Dunnewind T (2017) Economic consequences and potential preventable costs related to osteoporosis in the Netherlands. Value Health 20(6):762–8. https://doi.org/10.1016/j.jval.2017.02.006
Ratliff A (1999) What is a good decision. Eff Clin Pract 2:184–197
Stacey D, Légaré F, Lewis K, Barry MJ, Bennett CL, Eden KB, Holmes-Rovner M, Llewellyn-Thomas H, Lyddiatt A, Thomson R, Trevena L (2017) Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev (4). https://doi.org/10.1002/14651858.CD001431.pub5
Hiligsmann M, Ronda G, van der Weijden T, Boonen A (2016) The development of a personalized patient education tool for decision making for postmenopausal women with osteoporosis. Osteoporos Int 27(8):2489–2496. https://doi.org/10.1007/s00198-016-3555-1
Cornelissen D, Boonen A, Evers S, van den Bergh JP, Bours S, Wyers CE et al (2021) Improvement of osteoporosis Care Organized by Nurses: ICON study - protocol of a quasi-experimental study to assess the (cost)-effectiveness of combining a decision aid with motivational interviewing for improving medication persistence in patients with a recent fracture being treated at the fracture liaison service. BMC Musculoskelet Disord 22(1):913. https://doi.org/10.1186/s12891-021-04743-2
Stacey D, Volk RJ (2021) The International Patient Decision Aid Standards (IPDAS) collaboration: evidence update 2.0. Med Decis Making 41(7):729–33. https://doi.org/10.1177/0272989x211035681
Witteman HO, Maki KG, Vaisson G, Finderup J, Lewis KB, Dahl Steffensen K et al (2021) Systematic development of patient decision aids: an update from the IPDAS collaboration. Med Decis Making 41(7):736–754. https://doi.org/10.1177/0272989x211014163
Coulter A, Stilwell D, Kryworuchko J, Mullen PD, Ng CJ, van der Weijden T (2013) A systematic development process for patient decision aids. BMC Med Inform Decis Mak 13 Suppl 2(Suppl 2):S2. https://doi.org/10.1186/1472-6947-13-s2-s2
van der Weijden T, Dreesens D, Faber MJ, Bos N, Drenthen T, Maas I et al (2019) Developing quality criteria for patient-directed knowledge tools related to clinical practice guidelines. A development and consensus study. Health Expect 22(2):201–8. https://doi.org/10.1111/hex.12843
(2022) Osteoporose en fractuurpreventie: Federatie Medisch Specialisten. https://richtlijnendatabase.nl/richtlijn/osteoporose_en_fractuurpreventie/startpagina_-_osteoporose_en_fractuurpreventie.html. Accessed 21 December 2022
Te Kampe R, Boonen A, Jansen T, Janssen M, de Vries H, van Durme C (2022) Development of a patient decision aid for the initiation of urate-lowering therapy in gout patients. RMD Open 8(1). https://doi.org/10.1136/rmdopen-2021-001979
Griffith JF (2015) Identifying osteoporotic vertebral fracture. Quant Imaging Med Surg 5(4):592–602. https://doi.org/10.3978/j.issn.2223-4292.2015.08.01
Li N, Hiligsmann M, Boonen A, van Oostwaard MM, de Bot RTAL, Wyers CE et al (2021) The impact of fracture liaison services on subsequent fractures and mortality: a systematic literature review and meta-analysis. Osteoporos Int 32(8):1517–1530. https://doi.org/10.1007/s00198-021-05911-9
(2022) Farmacotherapeutisch kompas: Zorginstituut Nederland. https://www.farmacotherapeutischkompas.nl/. Accessed 5 Dec 2022
Huntjens KM, van Geel TA, van den Bergh JP, van Helden S, Willems P, Winkens B et al (2014) Fracture liaison service: impact on subsequent nonvertebral fracture incidence and mortality. J Bone Joint Surg Am 96(4):e29. https://doi.org/10.2106/jbjs.L.00223
van Geel TA, Huntjens KM, van den Bergh JP, Dinant GJ, Geusens PP (2010) Timing of subsequent fractures after an initial fracture. Curr Osteoporos Rep 8(3):118–122. https://doi.org/10.1007/s11914-010-0023-2
Paskins Z, Torres Roldan VD, Hawarden AW, Bullock L, Meritxell Urtecho S, Torres GF et al (2020) Quality and effectiveness of osteoporosis treatment decision aids: a systematic review and environmental scan. Osteoporos Int 31(10):1837–1851. https://doi.org/10.1007/s00198-020-05479-w
Carrissa Abigail Roxas M, Jimeno C, Palileo-Villanueva L, Macalalad-Josue AA, Sandoval MA, Fernandez JA (2020) Development of a patient decision aid for the treatment of osteoporosis among Filipino postmenopausal women. J ASEAN Fed Endocr Soc 35(1):93–101. https://doi.org/10.15605/jafes.035.01.15
McCaffery KJ, Smith SK, Wolf M (2010) The challenge of shared decision making among patients with lower literacy: a framework for research and development. Med Decis Making 30(1):35–44. https://doi.org/10.1177/0272989x09342279
Silvia KA, Sepucha KR (2006) Decision aids in routine practice: lessons from the breast cancer initiative. Health Expect 9(3):255–264. https://doi.org/10.1111/j.1369-7625.2006.00393.x
Acknowledgements
We would like to thank the patients and specialized nurses (Mehmet Elmacioglu, Astrid Kessels, and Claudia Vaessens – Deckers) who participated in the study. In addition, we would like to thank Suus Koene, office manager within the Department of Health Services Research at Maastricht University, for her help with the layout of the decision aid.
Funding
This study was funded by the ZonMw research line Rational Pharmacotherapy, grant number 848016001. METC study number is METC2028-0507-A-10.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The department of Marloes van Onna has received consultancy fees from Novartis, Pfizer, and Galapagos and a research grant from Pfizer. The department of Annelies Boonen has received consultancy fees from AbbVie, Novartis, and Galapagos. Mickaël Hiligsmann has received research grants paid to his institution by Amgen, Radius Health, and ViiV Healthcare, and consultancy fees from UCB. The department of Joop P. van den Bergh has received consultancy fees from UCB and Amgen. Dennis Cornelissen, Nele Raskin, Marsha van Oostwaard, Caroline E. Wyers, Trudy van der Weijden, Sandrine Bours, and Lieke Maas declare no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Maas, L., Raskin, N., van Onna, M. et al. Development and usability of a decision aid to initiate anti-osteoporosis medication treatment in patients visiting the fracture liaison service with a recent fracture. Osteoporos Int 35, 69–79 (2024). https://doi.org/10.1007/s00198-023-06906-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-023-06906-4