
Abstract
Summary
This population-based longitudinal follow-up study showed a protective effect of tea consumption against osteoporosis, particularly among women and middle-aged people. High tea consumption was also associated with a reduced risk of hip fracture.
Introduction
To investigate the association of tea consumption with the risks of osteoporosis and hip fracture.
Methods
This study used the Keelung Community-based Integrated Screening database and Taiwan’s National Health Insurance Research Database. A total of 42,742 subjects aged 45 to 74 years were enrolled. Each was classified as no tea consumption, low tea consumption, and high tea consumption, according to the results of an eating habits questionnaire. The diagnosis of osteoporosis and hip fracture was based on BMD measured by dual-energy X-ray absorptiometry and the X-ray findings. The median follow-up time was 8.5 years.
Results
As compared with the no tea consumption group, the osteoporosis HRs for the low tea consumption and high tea consumption groups were 0.88 (95% confidence interval (CI) 0.80–0.96) and 0.87 (95% CI 0.80–0.94), respectively. Among those participants aged 59 or below, the osteoporosis HRs for low tea consumption and high tea consumption (vs. no tea consumption) were 0.85 (95% CI 0.74–0.96) and 0.79 (95% CI 0.69–0.90). The HRs of hip fracture for the low tea consumption and high tea consumption groups (vs. no tea consumption) were 0.85 (95% CI 0.67–1.08) and 0.69 (95% CI 0.55–0.86), respectively.
Conclusion
Tea consumption was linked to a lower risk of osteoporosis, particularly among women and middle-aged people. High tea consumption was also associated with a reduced risk of hip fracture.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteoporosis is a chronic metabolic bone disease characterized by decreased bone mineral density (BMD) and deterioration of bony microarchitecture, resulting in bone fragility and greater susceptibility to fragility fractures [1]. Among fragility fractures, those of the hip have the most severe consequences, including significant morbidity and mortality, and increased socioeconomic and public-health burdens [2, 3].
Tea and tea-extract flavonoids, such as catechins, thearubigins, and theaflavins, have osteoprotective effects on bone biology because of their antioxidant and anti-inflammatory properties [4,5,6]. In animal-model studies, tea and tea-extract flavonoids have been found to protect against bone loss and microstructural deterioration, resulting in enhanced BMD and bone strength [7,8,9]. Most previous observational studies have also concluded that tea consumption had a positive effect on BMD [10, 11]. Although research on animal and human subjects has demonstrated that tea intake has a beneficial effect on bone health, previous studies have yielded inconsistent associations between tea consumption and the risk of hip fracture. Some prospective cohort studies have reported a null association between tea consumption and such risk [10, 12, 13], and other cohort studies have reported that tea consumption reduced such risk [14, 15]. Among the few cohort studies that simultaneously investigated the effects of tea intake on osteoporosis and hip fractures, the results were also inconsistent. Chen et al. showed that tea intake in postmenopausal women was positively associated with BMD, but tea intake had no significant impact on fracture risk [10]. Conversely, Myers et al. enrolled women aged more than 75 years and found that tea intake was not positively associated with hip BMD, but that — when high — it was associated with lower risks of osteoporotic fractures [15]. Moreover, because those two studies only recruited postmenopausal or older women, the interrelationship of tea consumption, osteoporosis, and hip fractures in men and middle age women remains unclear. As the associations between tea consumption and the risk of osteoporosis and hip fracture in men and middle age women are relatively under-studied, we therefore conducted this population-based, longitudinal follow-up study to investigate the impact of tea consumption on the risk of osteoporosis and hip fracture to help fill those gaps.
Materials and methods
Data sources
This study’s cohort was drawn from individuals who took part in the Keelung Community-based Integrated Screening (KCIS) project, which has been conducted by the Health Bureau of Keelung City, Taiwan, since the beginning of 1999 [16]. The KCIS project initially intended to screen for five types of cancer (cervical, breast, colorectal, oral cancer, and hepatocellular carcinoma) and three chronic diseases (hypertension, diabetes, and hyperlipidemia). Data on demographic characteristics and lifestyle habits — smoking, alcohol consumption, physical activity, diet, etc. — were collected using a structured questionnaire. The details of the KCIS database have been described in previous studies [16, 17]. By the time our study commenced, KCIS had screened and collected data on 109,425 people.
The present study used the KCIS data from 2005 to 2012 and linked them to Taiwan’s National Health Insurance (NHI) research database (NHIRD) and to the Mortality Registry from 2000 to 2015, both of which were found within the Health and Welfare Data Science Center database at National Taiwan University’s Health Data Research Center (HDRC). Taiwan’s National Health Insurance program is a single-payer, compulsory social insurance program, and the NHIRD covers more than 99% of the country’s population. Therefore, by linking these databases, a large-scale representative sample was assembled for analysis.
Study subjects and design
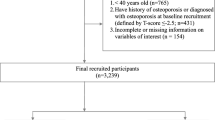
We implemented a longitudinal follow-up study to investigate the impact of tea consumption on osteoporosis and hip fracture. We used the weekly frequency of tea consumption to classify the KCIS-screened subjects into three groups — no tea consumption (NTC), low tea consumption (LTC), and high tea consumption (HTC), such frequency-based classification of tea consumption has been used in previous research [18]. The information on tea consumption was obtained according to the answers the participants had provided on KCIS-administered eating habits questionnaire, which is part of the structured questionnaire in KCIS project. The types of tea in the eating habits questionnaire included green tea, black tea, oolong tea, and other types of tea. Specifically, those answers had been provided on a five-point scale, with 1 = seven times/week or more, 2 = five to six times/week, 3 = three to four times/week, 4 = one or two times/week, and 5 = rarely or never. Our NTC group was defined as subjects who answered “5,” our LTC group as those who answered “3” or “4,” and our HTC group as those who answered “1” or “2.” Further details of the recruitment process for each group are shown in Fig. 1.

Flowchart illustrating the enrollment process of the study population
The inclusion criteria for subjects were (1) that they had tea-drinking data from their first screening in KCIS database between 2005 and 2012, which was defined as the index date; and (2) that they were between 45 and 74 years old on their respective index dates. Based on these criteria, a total of 45,667 subjects were included at this stage. Then, after linking these individuals’ screening information from the KCIS database to their medical information from the NHIRD, we excluded subjects who had been diagnosed with osteoporosis (International Classification of Diseases, Ninth Revision, Clinical Modification, [ICD-9-CM] code 733.0) or hip fracture (ICD-9-CM code 820) within 1 year before their index dates, and therefore, we can identify newly diagnosed osteoporosis and hip fracture cases as the outcome events during the follow-up. The diagnosis of osteoporosis in Taiwan’s NHI is made by physicians based on BMD measured by dual-energy X-ray absorptiometry. A T-score of less than − 2.5 is defined as osteoporosis. The diagnosis of hip fracture is made by doctors based on the X-ray findings. After excluding 1332 subjects with a history of osteoporosis or hip fracture, 44,335 subjects were left.
Based on consideration of the risk factors for osteoporosis and/or hip fracture, we adjusted our analysis model by incorporating a range of relevant comorbidities, demographic factors, and lifestyle factors [19, 20]. NHIRD medical records were used as the source of data on these comorbidities, which included cancer (ICD-9-CM codes 140–208), diabetes (ICD-9-CM code 250), hyperlipidemia (ICD-9-CM code 272), hypertension (ICD-9-CM codes 401–405), coronary heart disease (ICD-9-CM codes 410–414 and 429.2), and stroke (ICD-9-CM codes 430–438). Given comorbidity was deemed to have been present if the patient had at least one hospital discharge or two outpatient visits with the relevant diagnosis code(s) within 12 months before his/her index date.
The demographic and lifestyle factors included sex, age, body mass index (BMI, calculated with weight in kilograms divided by height in meters squared), smoking, alcohol consumption, education level, and physical activity (PA). The information on lifestyle factors and tea consumption was obtained simultaneously using a structured questionnaire in the KCIS project. Based on the weekly PA time, we categorized the subjects into three PA groups as in our previous publication [21]: (1) a no PA group, comprising subjects who answered “Never” to the PA question; (2) a low PA group, consisting of subjects whose weekly PA times were less than 90 min; and (3) a high PA group, which included subjects whose weekly PA times were 90 min or more. We chose 90 min as the cut-off point between low PA and high PA because a prior population-based study in Taiwan showed that 90 min a week of PA reduced mortality from all causes [22].
The questionnaire used to collect education level classified it as “lower” if they had only attended elementary school; “median” if they had been to junior or senior high school; and “higher” if they had attended a university and/or other tertiary institution. Missing lifestyle data led to the exclusion of a further 1593 subjects, leaving a final sample of 42,742 (NTC, n = 17,511; LTC, n = 11,208; HTC, n = 14,023).
Ethics statement
The present study was approved by the National Taiwan University Hospital Research Ethics Committee (NTUH-REC No.: 201802004RIND). This study analyzed existing data from the Keelung Community-based Integrated Screening database and Taiwan’s National Health Insurance Research Database. To protect privacy, all identification numbers linked to information about individuals in the two databases were encrypted before data processing. Additionally, the health data used in this study could only be accessed in an access-controlled, privacy-protected room within the HDRC. Accordingly, the present study used pre-existing de-identified data released for research purposes; the requirement for informed consent was waived.
Occurrence of osteoporosis and hip fracture
The primary outcome of this study was newly diagnosed osteoporosis or hip fracture. The subjects were tracked from their index dates to either the first occurrences of osteoporosis or hip fracture, or if there were no such occurrences, to the end of 2015. Newly diagnosed osteoporosis was indicated by at least one inpatient discharge or two outpatient visits with ICD-9-CM code 733.0, and newly diagnosed hip fracture, by at least one inpatient discharge with ICD-9-CM code 820 during follow-up. The occurrence of a second hip fracture was not included as an outcome event.
Statistical analysis
All analyses were performed using SAS version 9.4 software (SAS Institute, Cary, NC). We examined inter-group differences in the demographic, lifestyle, and comorbidity variables using chi-square testing and analysis of variance (ANOVA). The incidence rate was calculated as the number of osteoporosis or hip-fracture events in a tea group, divided by the total follow-up time of that group (per 1000 person-years). Cox proportional-hazard regression was then applied to estimate the effect of tea-group membership on each of the two target medical conditions. Also, because the association of tea consumption with osteoporosis might vary by sex or age, we used stratified analysis to account for those factors separately. All p values reported are 2-sided, and the significance level was set at < 0.05.
Results
Table 1 shows the baseline characteristics of women. There were significant inter-group differences in age, body mass index (BMI), lifestyle factors, and comorbidities (diabetes, hypertension, hyperlipidemia, coronary heart disease, stroke, and cancer) among the NTC, LTC, and HTC groups in women. The baseline characteristics of men are presented in Table 2. There were notable inter-group differences in age, BMI, lifestyle factors, and comorbidities (hypertension, hyperlipidemia, coronary heart disease, and stroke) among the NTC, LTC, and HTC groups in men. The median follow-up time was 8.5 years, with an interquartile range of 3.3 years.
Risk of osteoporosis
The number of osteoporosis events and hazard ratio of osteoporosis for the three groups is presented in Table 3. During the follow-up period, 3278 cases of osteoporosis were identified. Our analytical results showed that the LTC and HTC groups both had a significantly lower risk of developing osteoporosis than the NTC group.
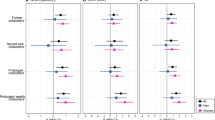
Table 3 also showed the sex-stratified and age-stratified HRs for osteoporosis for the three tea-consumption groups. In the sex-stratified analysis, women who drank tea had a lower risk of osteoporosis than women who never drank any. Compared with the NTC group, the multivariate-adjusted HR (aHR) for the LTC group was 0.86 (95% CI 0.78–0.95), and the aHR for the HTC group was 0.88 (95% CI 0.80–0.97). For the men stratum, the same analyses were not statistically significant. Compared with the NTC group, the aHR for the LTC group was 1.03 (95% CI 0.81–1.32), and the aHR for the HTC group was 0.82 (95% CI 0.66–1.03). The age-stratified analysis showed that tea consumption was negatively associated with osteoporosis in the middle-aged stratum (45 to 59 years). Compared with the NTC group, the aHR for the LTC and the HTC groups were 0.85 (95% CI 0.74–0.96), and 0.79 (95% CI 0.69–0.90), respectively. However, there was no significant association in the old-aged stratum (60 to 74 years). Compared with the NTC group, the aHR for the LTC and HTC groups were 0.90 (95% CI 0.79–1.02) and 0.94 (95% CI 0.83–1.05), respectively.
Risk of hip fracture
The number of hip-fracture events and adjusted HRs for hip fracture for the three tea-consumption groups is presented in Table 4. During the follow-up period, 454 cases of hip fracture were identified. Compared with the NTC group, the HTC group had a reduced risk of hip fracture (aHR = 0.69, 95% CI 0.55–0.86), but the LTC-NTC difference in such risk was non-significant (aHR = 0.85, 95% CI 0.67–1.08).
Discussion
The results of this population-based longitudinal follow-up study suggest that individuals who drink tea are at a lower risk of osteoporosis than those who do not. To the best of our knowledge, this is the first large-scale cohort study to show that the negative association between tea consumption and osteoporosis is more prominent in the middle-aged population (aged 45 to 59 years) than among the elderly (aged 60 to 74 years). In addition, we found that people who reported high tea consumption had a reduced risk of hip fracture compared with those who reported consuming no tea.
Prior studies, which mainly enrolled postmenopausal women, demonstrated that tea consumption might reduce osteoporosis risk [10, 11, 23, 24]. In contrast, a limited number of studies investigating the effect of tea consumption on osteoporosis among men reported a lack of protective effect [18, 25, 26]. Similar to previous studies, our study found that tea consumption was associated with a lower risk of osteoporosis in women, and there was a lack of significant association between tea consumption and osteoporosis in men. Moreover, while few previous studies have evaluated the protective effect of tea consumption against osteoporosis in the middle-aged population, our study showed that tea’s benefits were more prominent among middle-aged population (aged 45 to 59 years) than elderly people. Such findings could mean that policies encouraging regular tea consumption among middle-aged people (aged 45 to 59 years) might help reduce their risk of osteoporosis. However, the explanation for a more beneficial response in young adults is unclear. Further studies are needed to elucidate these findings.
Previous studies on the association between tea consumption and hip fracture have yielded inconclusive results. Myers et al. showed that higher tea consumption had a protective effect against osteoporotic fractures in women in Australia aged 75 and above [15]. In contrast, Chen et al. reported no significant association between tea consumption and hip fracture in postmenopausal women in the USA aged 50 to 79 [10]. However, these two studies may have limited generalizability, as they only recruited postmenopausal women who were willing to be followed up in clinical centers. Our study used a representative sample from a community-based screening program and showed that high tea consumption was associated with a lower risk of hip fracture (Table 4, aHR = 0.69, 95% CI 0.55–0.86).
Excessive oxidative stress or chronic inflammation can accelerate bone resorption and osteoporosis [6, 27]. Tea-extract flavonoids have antioxidant and anti-inflammatory properties and have been demonstrated to protect against bone loss and reduce the risk of osteoporosis [4, 28]. In ovariectomized animal models, green tea extract and black tea extract have been suggested to diminish the expression of the osteoclast-specific gene and proteins and inhibit the osteoclastogenesis, with an effective improvement of osteoporosis [8, 9]. Based on previous experimental evidence, then, our findings that tea consumption had a protective effect against osteoporosis are biologically plausible. However, many types of tea contain caffeine [29]. Previous studies have suggested that high caffeine intake accelerates bone loss in elderly women and is associated with an increased fracture risk [12, 13]. Therefore, further study is needed to investigate the optimal tea consumption to protect against osteoporosis.
While low BMD is one major measurable determinant of the risk of osteoporotic fractures, risk factors for hip fractures other than low BMD include those that affect the odds of trauma (e.g., fall) occurring, including neuromuscular impairment, cognitive impairment, physical inactivity, and use of sedative medications [30]. Previous studies have shown that tea and tea-extract flavonoids could improve self-reported alertness, are associated with a lower risk of cognitive impairment [31], and help maintain skeletal muscle health [32]. Consequently, they could decrease fall-related fragility hip fractures.
The key strength of this study was its population-based design with long-term follow-up. In addition, our study at baseline recruited members of two groups — males and the middle-aged — that are relatively under-studied in the context of osteoporosis and hip fracture. Nevertheless, this observational study design is not able to establish a causal relationship. Moreover, there are several limitations of this study that should be acknowledged. First, the eating habits questionnaire used in KCIS recorded the frequency of tea consumption self-reported by screening participants without measuring the accurate dose of tea intake. In addition, detailed information about vitamin D and calcium intake is not available in the database. These factors were not included in the analysis. Thus, it is possible that residual confounding of the association between tea consumption and osteoporosis may have been present. Moreover, the benefit of tea consumption on bone health could be confounded by other nutritional factors, lifestyle factors, or substitute beverages such as coffee. Nevertheless, it has been suggested that caffeine generally plays a minor role in bone health [33].
Second, the diagnoses of osteoporosis, hip fractures, and medical comorbidities were determined using the ICD codes from the NHIRD, which could raise concerns about their accuracy. However, the NHI Bureau’s audit committees randomly sample its claim data and regularly review medical records to verify diagnostic accuracy, as well as the quality of care. Consequently, the NHIRD is a well-established research database, and the validity of its data has been demonstrated by independent studies [34]. However, since the DXA scanners used in the clinics of the NHI system were not all the same model, and the DXA scanners were not cross-validated, there may be measurement errors of BMD.
Third, because of an insufficient number of hip fracture events, subgroup analysis of the association between tea consumption of hip fracture was not performed. Further research on the impact of tea consumption on the risk of hip fracture stratified by age and sex is suggested. Fourth, the ethnicity of the participants was Taiwanese, and the results of this study may not be generalized to other ethnic groups.
In conclusion, the present population-based longitudinal follow-up study has shown that tea consumption was associated with a reduced risk of osteoporosis. Moreover, people with high tea consumption were at a lower risk of hip fracture. However, further studies are needed to investigate the mechanisms that underlie these findings.
Data availability
The data generated and analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Code availability
Not applicable.
References
Sozen T, Ozisik L, Basaran NC (2017) An overview and management of osteoporosis. Eur J Rheumatol 4:46–56. https://doi.org/10.5152/eurjrheum.2016.048
Strom O, Borgstrom F, Kanis JA, Compston J, Cooper C, McCloskey EV, Jonsson B (2011) Osteoporosis: burden, health care provision and opportunities in the EU: a report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch Osteoporos 6:59–155. https://doi.org/10.1007/s11657-011-0060-1
Abrahamsen B, van Staa T, Ariely R, Olson M, Cooper C (2009) Excess mortality following hip fracture: a systematic epidemiological review. Osteoporos Int 20:1633–1650. https://doi.org/10.1007/s00198-009-0920-3
Huang HT, Cheng TL, Lin SY, Ho CJ, Chyu JY, Yang RS, Chen CH, Shen CL (2020) Osteoprotective roles of green tea catechins. Antioxidants (Basel) 9:1136. https://doi.org/10.3390/antiox9111136
Bellavia D, Dimarco E, Costa V, Carina V, De Luca A, Raimondi L, Fini M, Gentile C, Caradonna F, Giavaresi G (2021) Flavonoids in bone erosive diseases: perspectives in osteoporosis treatment. Trends Endocrinol Metab 32:76–94. https://doi.org/10.1016/j.tem.2020.11.007
Kimball JS, Johnson JP, Carlson DA (2021) Oxidative stress and osteoporosis. The Journal of bone and joint surgery American 103:1451–1461. https://doi.org/10.2106/jbjs.20.00989
Siu WS, Ko CH, Shiu HT, Li KK, Shum WT, Leung PC, Zhang JF (2021) Green tea extract synergistically enhances the effectiveness of an antiresorptive drug on management of osteoporosis induced by ovariectomy in a rat model. Exp Ther Med 21:328. https://doi.org/10.3892/etm.2021.9759
Wu X, Xie CQ, Zhu QQ et al (2018) Green tea (Camellia sinensis) aqueous extract alleviates postmenopausal osteoporosis in ovariectomized rats and prevents RANKL-induced osteoclastogenesis in vitro. Food Nutr Res 62.https://doi.org/10.29219/fnr.v62.1478
Liang Q, Lv M, Zhang X, Hu J, Wu Y, Huang Y, Wang X, Sheng J (2018) Effect of black tea extract and thearubigins on osteoporosis in rats and osteoclast formation in vitro. Front Physiol 9:1225. https://doi.org/10.3389/fphys.2018.01225
Chen Z, Pettinger MB, Ritenbaugh C, LaCroix AZ, Robbins J, Caan BJ, Barad DH, Hakim IA (2003) Habitual tea consumption and risk of osteoporosis: a prospective study in the women’s health initiative observational cohort. Am J Epidemiol 158:772–781. https://doi.org/10.1093/aje/kwg214
Devine A, Hodgson JM, Dick IM, Prince RL (2007) Tea drinking is associated with benefits on bone density in older women. Am J Clin Nutr 86:1243–1247. https://doi.org/10.1093/ajcn/86.4.1243
Dai Z, Jin A, Soh AZ, Ang LW, Yuan JM, Koh WP (2018) Coffee and tea drinking in relation to risk of hip fracture in the Singapore Chinese Health Study. Bone 112:51–57. https://doi.org/10.1016/j.bone.2018.04.010
Hallstrom H, Wolk A, Glynn A, Michaelsson K (2006) Coffee, tea and caffeine consumption in relation to osteoporotic fracture risk in a cohort of Swedish women. Osteoporos Int 17:1055–1064. https://doi.org/10.1007/s00198-006-0109-y
Shen Q, Yu C, Guo Y et al (2018) Habitual tea consumption and risk of fracture in 0.5 million Chinese adults: a prospective cohort study. Nutrients 10:1633. https://doi.org/10.3390/nu10111633
Myers G, Prince RL, Kerr DA, Devine A, Woodman RJ, Lewis JR, Hodgson JM (2015) Tea and flavonoid intake predict osteoporotic fracture risk in elderly Australian women: a prospective study. Am J Clin Nutr 102:958–965. https://doi.org/10.3945/ajcn.115.109892
Chiu YH, Chen LS, Chan CC, Liou DM, Wu SC, Kuo HS, Chang HJ, Chen TH (2006) Health information system for community-based multiple screening in Keelung, Taiwan (Keelung Community-based Integrated Screening No. 3). Int J Med Inform 75:369–383. https://doi.org/10.1016/j.ijmedinf.2005.07.033
Chen TH, Chiu YH, Luh DL et al (2004) Community-based multiple screening model: design, implementation, and analysis of 42,387 participants. Cancer 100:1734–1743. https://doi.org/10.1002/cncr.20171
Li X, Qiao Y, Yu C et al (2019) Tea consumption and bone health in Chinese adults: a population-based study. Osteoporos Int 30:333–341. https://doi.org/10.1007/s00198-018-4767-3
Nguyen TV, Center JR, Eisman JA (2004) Osteoporosis: underrated, underdiagnosed and undertreated. Med J Aust 180:S18-22. https://doi.org/10.5694/j.1326-5377.2004.tb05908.x
Kanis JA, Borgstrom F, De Laet C, Johansson H, Johnell O, Jonsson B, Oden A, Zethraeus N, Pfleger B, Khaltaev N (2005) Assessment of fracture risk. Osteoporos Int 16:581–589. https://doi.org/10.1007/s00198-004-1780-5
Feng SH, Chen LS, Yeh KC, Pan SL (2021) Physical activity and the risk of hemorrhagic stroke: a population-based longitudinal follow-up study in Taiwan. Front Med (Lausanne) 8:791772. https://doi.org/10.3389/fmed.2021.791772
Wen CP, Wai JP, Tsai MK, Yang YC, Cheng TY, Lee MC, Chan HT, Tsao CK, Tsai SP, Wu X (2011) Minimum amount of physical activity for reduced mortality and extended life expectancy: a prospective cohort study. Lancet 378:1244–1253. https://doi.org/10.1016/s0140-6736(11)60749-6
Hirata H, Kitamura K, Saito T, Kobayashi R, Iwasaki M, Yoshihara A, Watanabe Y, Oshiki R, Nishiwaki T, Nakamura K (2016) Association between dietary intake and bone mineral density in Japanese postmenopausal women: the Yokogoshi cohort study. Tohoku J Exp Med 239:95–101. https://doi.org/10.1620/tjem.239.95
Guo M, Qu H, Xu L, Shi DZ (2017) Tea consumption may decrease the risk of osteoporosis: an updated meta-analysis of observational studies. Nutr Res 42:1–10. https://doi.org/10.1016/j.nutres.2017.02.010
Hossein-Nezhad A, Maghbooli Z, Shafaei A, Javadi E, Larijani B (2007) Relationship between tea drinking and bone mineral density in Iranian population. Iran J Public Health 36(Supple 1):57–62. https://ijph.tums.ac.ir/index.php/ijph/article/view/1527
Wu CH, Yang YC, Yao WJ, Lu FH, Wu JS, Chang CJ (2002) Epidemiological evidence of increased bone mineral density in habitual tea drinkers. Arch Intern Med 162:1001–1006. https://doi.org/10.1001/archinte.162.9.1001
Cervellati C, Bonaccorsi G, Cremonini E, Romani A, Fila E, Castaldini MC, Ferrazzini S, Giganti M, Massari L (2014) Oxidative stress and bone resorption interplay as a possible trigger for postmenopausal osteoporosis. Biomed Res Int 2014:569563. https://doi.org/10.1155/2014/569563
Shen CL, Chyu MC (2016) Tea flavonoids for bone health: from animals to humans. J Investig Med 64:1151–1157. https://doi.org/10.1136/jim-2016-000190
Chin JM, Merves ML, Goldberger BA, Sampson-Cone A, Cone EJ (2008) Caffeine content of brewed teas. J Anal Toxicol 32:702–704. https://doi.org/10.1093/jat/32.8.702
Cummings-Vaughn LA, Gammack JK (2011) Falls, osteoporosis, and hip fractures. Med Clin North Am 95:495-506 x. https://doi.org/10.1016/j.mcna.2011.03.003
Zhang J, Wang A, Zhang X, Chen S, Wu S, Zhao X, Zhang Q (2020) Association between tea consumption and cognitive impairment in middle-aged and older adults. BMC Geriatr 20:447. https://doi.org/10.1186/s12877-020-01848-6
Luk HY, Appell C, Chyu MC, Chen CH, Wang CY, Yang RS, Shen CL (2020) Impacts of green tea on joint and skeletal muscle health: prospects of translational nutrition. antioxidants (Basel) 9:1050. https://doi.org/10.3390/antiox9111050
Wikoff D, Welsh BT, Henderson R et al (2017) Systematic review of the potential adverse effects of caffeine consumption in healthy adults, pregnant women, adolescents, and children. Food Chem Toxicol 109:585–648. https://doi.org/10.1016/j.fct.2017.04.002
Wen CP, Tsai SP, Chung WS (2008) A 10-year experience with universal health insurance in Taiwan: measuring changes in health and health disparity. Ann Intern Med 148:258–267. https://doi.org/10.7326/0003-4819-148-4-200802190-00004
Funding
This research was supported by grant MOST 107–2314-B-002–051 from the Ministry of Science and Technology, Executive Yuan, Republic of China, which placed no restrictions on its publications.
Author information
Authors and Affiliations
Contributions
YPH, LSC, and SLP designed the research; YPH, SHF, YSL, and SLP conducted the research; YPH and SLP analyzed the data; YPH, LSC, SHF, YSL, and SLP wrote the manuscript; and YPH, LSC, SHF, YSL, and SLP had primary responsibility for final content. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
For this type of study formal consent is not required.
Informed consent
Not applicable.
Consent for publication
Consent for submission and publication has been received from all the authors.
Conflict of interest
None.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Huang, YP., Chen, LS., Feng, SH. et al. Tea consumption and the risks of osteoporosis and hip fracture: a population-based longitudinal follow-up study. Osteoporos Int 34, 101–109 (2023). https://doi.org/10.1007/s00198-022-06569-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-022-06569-7