
Abstract
Summary
X-ray, CT and DXA enable diagnosis of vertebral deformities. For this study, level of agreement of vertebral deformity diagnosis was analysed. We showed that especially on subject level, these imaging techniques could be used for opportunistic screening of vertebral deformities in COPD patients.
Introduction
X-ray and CT are frequently used for pulmonary evaluation in patients with chronic obstructive pulmonary disease (COPD) and also enable to diagnose vertebral deformities together with dual-energy X-ray absorptiometry (DXA) imaging. The aim of this research was to study the level of agreement of these imaging modalities for diagnosis of vertebral deformities from T4 to L1.
Methods
Eighty-seven subjects (mean age of 65; 50 males; 57 COPD patients) who had X-ray, chest CT (CCT) and DXA were included. Evaluable vertebrae were scored twice using SpineAnalyzer™ software. ICCs and kappas were calculated to examine intra-observer variability. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and area under the receiver operating characteristic curve (AUROC) were calculated to compare vertebral deformities diagnosed on the different imaging modalities.
Results
ICCs for height measurements were excellent (> 0.94). Kappas were good to excellent (0.64–0.77). At vertebral level, the AUROC was 0.85 for CCT vs. X-ray, 0.74 for DXA vs. X-ray and 0.77 for DXA vs. CCT. Sensitivity (51%–73%) and PPV (57%–70%) were fair to good; specificity and NPV were excellent (≥ 96%). At subject level, the AUROC values were comparable.
Conclusions
Reproducibility of height measurements of vertebrae is excellent with all three imaging modalities. On subject level, diagnostic performance of CT (PPV 79–82%; NPV 90–93%), and to a slightly lesser extend of DXA (PPV 73–77%; NPV 80–89%), indicates that these imaging techniques could be used for opportunistic screening of vertebral deformities in COPD patients.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
There is an increasing awareness of the risk of vertebral fractures (VFs) in patients with chronic obstructive pulmonary disease (COPD); nevertheless, COPD-associated osteoporosis is largely undertreated [1].
The reported prevalence of VFs in elderly subjects varies from 5.0% up to 17.8% [2,3,4], depending on factors such as age, sex and race. Among patients with COPD, the prevalence of VFs is even higher, ranging from 26.8% up to 79.4% [5,6,7,8,9,10].
Presence of VFs is associated with increased morbidity, such as back pain, height loss [11], change in posture [12, 13], increased risk for subsequent non-vertebral [14,15,16,17] and vertebral [15, 17, 18] fractures and mortality [19, 20]. Presence of VFs is also associated with respiratory function in COPD patients [1, 10] as well as in patients without known lung diseases [21]. More specifically, Watanabe et al. found an association between the presence of VFs and the ratio between forced expiratory volume in 1 s and forced vital capacity (FEV1/FVC) and between VF severity and FVC [10] in patients with COPD.
Even though VFs occur in a substantial proportion of the elderly population, they are often undiagnosed [22] due to the absence of high impact trauma and lack of typical signs and symptoms of an acute fracture.
Chest X-ray and computed tomography (CCT) of the chest are regularly performed in clinical practice for pulmonary evaluation in COPD patients. Vertebral deformities can be diagnosed on X-ray and CCT images and also on lateral dual-energy X-ray absorptiometry (DXA) images. In clinical practice, these three imaging techniques are often applied in COPD patients, but radiological reports on diagnosed deformities may not always be congruent [23,24,25,26].
Comparisons between imaging modalities found in literature mostly concern DXA and X-ray images. In a systematic review, Lee et al. [26] concluded that in general, sensitivity is modest and specificity is high when comparing deformities on DXA to X-ray. Takada et al. compared deformities on CT lateral scout views to X-ray [24] and showed good agreement in the total thoracolumbar area (T4-L4), with best agreement in the lumbar part of the spine (L1-L4).
Data about the comparison of vertebral deformities on DXA and X-ray are sparse, and to our knowledge, there is no study yet regarding the number and severity of vertebral deformities when comparing the three imaging modalities.
Therefore, the aim of this research was to study the level of agreement of these imaging modalities for diagnosis of vertebral deformities from T4 to L1.
Methodology
Subjects
For this study, we used data of subjects included in a clinical trial related to osteoporosis in COPD patients (NCT01067248) at the Catharina Hospital (Eindhoven, the Netherlands) between February 2010 and September 2011 (approved by medical ethical committee of the Catharina hospital, M09-1971). The purpose clinical trial was to investigate the pathophysiologic mechanism of osteoporosis in COPD [27].
Details of the clinical trial as well as inclusion and exclusion criteria were described elsewhere [27]. In short, Caucasian males and postmenopausal females aged 50 years or older with moderate to very severe COPD (classified according to the Global Initiative for Chronic Obstructive Pulmonary disease, GOLD [28]), with either osteoporosis or normal BMD (based on lowest T-score of the lumbar spine (L1-L4), femoral neck and total hip), and either with or without vertebral deformities were included, as well as age-matched subjects without COPD.
For the purpose of this study, only subjects with complete availability of an X-ray, a CCT and a DXA with lateral imaging of the spine were included for this study.
Imaging
Lateral X-ray images of the thoracic spine (the current gold standard for assessment of vertebral deformities according to the Dutch guidelines [29]) were obtained by digital radiography (exposure at 125 kV; Digital Diagnost, Philips Health Care, Eindhoven, the Netherlands).
Lateral DXA images of the spine were obtained using a Hologic Discovery A (S/N83295) DXA scanner (Hologic, Tromp Medical Engineering BV, Castricum, the Netherlands). Both X-ray and DXA images were digitally available as Dicom files.
CCT scans of the chest were obtained using either a Philips Brilliance 64 (slice thickness 1 or 0.625) or a Philips iCT 256 scanner (slice thickness 1.25) (both 120 kVp, 350-mm field of view; Philips Health Care, Eindhoven, the Netherlands). To combine information of the sagittal reformats and to mimic the visualisation of the vertebrae on X-ray and DXA, all sagittal reformats containing the spine were superposed into one image: contrast was adjusted in the reformats to (partly) eliminate soft tissue, after which the sagittal reformats were superposed to create simulated X-ray images based on CCT using Matlab version R2013a (MathWorks®).
Vertebral deformity assessment
For morphometric assessment of height loss at posterior, middle and anterior site, SpineAnalyzer™ software (Optasia Medical, Cheadle, UK) was used. This software semi-automatically detects the vertebral shape (height and deformation) on lateral X-ray [30] or DXA [31] images based on user indicated points centred in the vertebrae. Details about the methodology were described elsewhere [30, 31]. All of the automatically detected points of the six-point morphometry were manually checked and adjusted if necessary, to make sure the height measurements were in accordance with human interpretation of the image (i.e. no diagnosis of vertebral deformities due to fusion of adjacent vertebrae or Schmorl’s nodes). Vertebrae that were not evaluable because of anomalies or other deformities were not included in the analyses. Since deformations were scored based on height measurements and not all qualitative features of morphology were taken into account while grading the deformations, we measured vertebral deformities rather than vertebral fractures.
Based on the measured amount of height loss, the vertebrae were scored according to the cut-off values for vertebral height loss according to the method initially described by Genant et al. [32] as no deformity (height loss < 20%: grade 0), mild deformity (20% ≤ height loss < 25%: grade 1), moderate deformity (25% ≤ height loss < 40%: grade 2) or severe deformity (height loss > 40%: grade 3).
Outcome measures automatically generated by SpineAnalyzer were absolute height (at posterior, middle and anterior site), deformity in percentage (wedge, biconcave, crush) and deformity grade (0–3).
For all image modalities (X-ray, CCT and DXA), vertebrae between T4 and L1 were evaluated by one experienced operator (MvD). The operator was trained to apply SpineAnalyzer software by a medical consultant of the software company. All images from one modality were assessed in random order. If all images from one modality were scored, the next modality was scored, again in random order. The second round of evaluation took place with at least 6 weeks in between repeated measures to exclude the change of a recall bias of the previous evaluation round.
To compare the number and severity of vertebral deformities on different image modalities, average heights at the posterior, middle and anterior site were calculated based on the two evaluation rounds. Based on the calculated average heights, deformity in percentage was calculated, resulting in deformity grades (0–3).
After scoring of the individual imaging modalities, the images were compared between modalities to cross-check vertebral levels. In case of discrepancy, a correction was made in vertebral levels based on anatomical landmarks visible in both images, in order to make sure the levels of vertebrae were matched when comparing the different imaging modalities.
Statistics
Since SpineAnalyzer was validated for X-ray and DXA images, but not yet for CCT-based images, we calculated intraclass correlation coefficients (ICC; two-way random, absolute agreement, single rater) for absolute height measurements (posterior, middle and anterior) for all three imaging modalities. Kappa was calculated for diagnosing a vertebral deformity regardless of grade (grade 1–3) or deformity grade 2–3. Kappa and ICC values were interpreted according to Cicchetti et al. [33]: below 0.40, the level of clinical significance was poor; between 0.40 and 0.59, it was fair; between 0.60 and 0.74, it was good; and equal to or above 0.75, it was excellent.
For comparison of vertebral deformities diagnosed on vertebral level between the three imaging modalities, lateral X-ray images were used as gold standard. Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated for diagnosing a vertebral deformity regardless of deformity grade, as well as for deformity grades 2 or higher. Furthermore, we calculated sensitivity, specificity, PPV, NPV of diagnosing a deformity on DXA compared to CCT.
In addition, we also calculated the area under the receiver operating characteristic curve (AUROC) to determine how well vertebral deformities can be diagnosed with CCT (compared to X-ray) and DXA (compared to X-ray and CCT). The AUROC was interpreted as a fail for values between 0.50 and 0.60; poor between 0.61 and 0.70; fair between 0.71 and 0.80; good between 0.81 and 0.90; and excellent if the value was above 0.90.
For comparison between the three imaging modalities on subject level, each of the images was scored as a vertebral deformity grades 0, 1, 2 or 3 according to the vertebrae with the highest deformity-grade visible between T4 and L1. If not all vertebrae between T4 and L1 were clearly evaluable, images were scored according to the vertebrae that were evaluable, i.e. the number of vertebrae evaluated per subject was not necessarily equal between imaging modalities.
All statistical analyses were performed in SPSS 24 (IBM) and MS Excel 2010.
Results
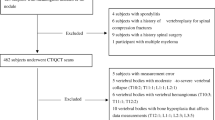
In the original study, 102 subjects were included (67 with and 35 without COPD; 48 with osteoporosis and 54 normal BMD; mean age of 65; 58 males and 44 females). Of those, 87 had complete assessment of X-ray, CCT and DXA of sufficient quality for height measurement of the vertebrae. Characteristics of these 87 included subjects are given in Table 1.
X-ray and CCT were made on the same day. The mean time interval with DXA was 157.6 days (standard deviation 166.6 days).
When scoring all vertebrae from T4 to L1, there were 766 vertebrae (88% of total) identified for height measurements on X-ray images, 787 (90%) on CCT and 718 (83%) on DXA. There were 593 (68.2%) vertebrae evaluable with all three imaging modalities, of which 50 (8.4%) showed a vertebral deformities grade 1–3 according to X-ray, 53 (8.9%) according to CCT and 45 (7.6%) according to DXA.
The distribution of deformities was not equal among vertebrae. By any method, most vertebral deformities were found in the mid-thoracic (T7/T8) and the thoracolumbar (T11/T12) area (Fig. 1). An example of vertebral deformities diagnosed on the three different imaging modalities can be found in the online supplementary material.

Vertebrae scored and deformities diagnosed on each image modality per location (T4-L1) in absolute numbers (a–c, maximum = 87) and percentages (d–f)
Intra-rater reliability on three different imaging techniques
ICCs showed excellent reproducibility of absolute height measurements for all three techniques (ICC > 0.94; Table 2). Kappas for diagnosing a vertebral deformity grade 1–3 or deformity grade 2–3 at vertebral level were good and even excellent for diagnosing deformity grade 2–3 on CCT (Table 3).
Agreement between X-ray, CCT and DXA at vertebral level
There were 725 matching vertebrae identified between T4 and L1 to compare between CCT and X-ray, 631 vertebrae for DXA and X-ray and 640 for DXA and CCT (Table 4).
Sensitivity of diagnosing a vertebral deformity regardless of grade (grade 1–3) was 73% for CCT compared to X-ray, 51% for DXA compared to X-ray and 57% for DXA compared to CCT. For diagnosing moderate or severe deformities (grade 2–3), sensitivity was to 72, 44 and 42% resp.
PPV for vertebral deformities regardless of grade (grade 1–3) was 70% for CCT compared to X-ray, 57% for DXA compared to X-ray and 69% for DXA compared to CCT. PPV was 78, 65 and 61% resp. when looking at grade 2–3 deformities only.
Specificity and NPV were ≥ 97% for all comparisons, for diagnosing deformity grade 1–3 as well as grade 2–3.
The AUROC values were good for CCT compared to X-ray (0.85–0.86) and fair for DXA compared to X-ray (0.72–0.74) or to CCT (0.71–0.77) (Table 4).
Agreement between X-ray, CCT and DXA at subject level
At subject level, sensitivity of diagnosing subjects with a vertebral deformity grade 1–3 was 86% for CCT compared to X-ray, 69% for DXA compared to X-ray and 68% for DXA compared to CCT. Sensitivity was 74, 58 and 59% resp. for diagnosing vertebral deformity grades 2–3.
PPV was 79% for CCT compared to X-ray, 77% for DXA compared to X-ray and 84% for DXA compared to CCT for all grades of vertebral deformities, and 82, 73 and 67% resp. for vertebral deformity grades 2–3.
Specificity of diagnosing subjects with a vertebral deformity grade 1–3 was 85% for CCT compared to X-ray, 87% for DXA compared to X-ray and 90% for DXA compared to CCT. Specificity was 96, 94 and 93% resp. for subjects with vertebral deformity grades 2–3.
NPV was 90% for CCT compared to X-ray, 80% for DXA compared to X-ray and 79% for DXA compared to CCT and was 93, 89 and 90% resp. when looking at vertebral deformity grades 2–3.
AUROC values were good for CCT compared to X-ray (0.85) and fair for DXA compared to X-ray (0.76–0.78) or to CCT (0.76–0.79) (Table 5).
Discussion
This study showed that reproducibility of height measurement of vertebrae is very good on all three imaging modalities. We also showed that diagnosis of vertebral deformities on vertebral level results in higher sensitivity, PPV, NPV and AUROC value on CCT than DXA when compared to X-ray, but that CCT and DXA showed the same level of specificity. Also on subject level, sensitivity is higher with CCT than with DXA compared to X-ray, except for specificity when looking at vertebral deformity grades 1–3 (85 vs. 87%).
Our reproducibility results for X-ray, CCT and DXA are similar to the results presented by Kim et al. [23], in which SpineAnalyzer software was used to measure vertebral deformities on CCT lateral scout views.
In literature, there are several studies comparing vertebral deformities diagnosed on DXA to X-ray, mostly from T4 to L4, reporting a sensitivity between 57 and 100% and a specificity between 89 and 100% on vertebral level [25, 34,35,36,37,38,39,40,41]. We found comparable specificity (97%) but lower sensitivity (51%) when comparing DXA to X-ray images from T4 to L1. Also, on subject level, we found lower sensitivity (69%) but comparable specificity (87%) compared to other studies (sensitivity 69–97%, specificity 74–100%) [34, 36,37,38,39, 41,42,43,44]. One reason could be that most other studies included the lumbar spine in the analysis, in which vertebral deformities are less frequent, while we measured T4 to L1. Some studies pointed out that sensitivity and specificity are not uniformly distributed over the spine. In general, sensitivity is lower in the upper thoracic area [39, 42, 45] due to lower image quality especially in the upper thoracic levels, which may also partly explain the lower sensitivity in our study.
On vertebral level, we found the lowest number of grade 1–3 vertebral deformities on DXA images (7.6% of all vertebrae evaluated by all three imaging modalities), followed by X-ray (8.4%) and most vertebral deformities on CCT images (8.9%). Because we found more deformities (grade 1–3) on CCT images, the results suggest that CCT might be a more sensitive method to diagnose vertebral deformities than the current gold-standard X-ray.
We found a modest PPV (57–70%) but a very high NPV (96–97%) on vertebral level. On subject level, diagnostic performance of CT (PPV: 79–82%; NPV: 90–93%) was somewhat better than of DXA (PPV: 73–77%; NPV: 80–89%) compared to X-ray. This suggests that CCT and, to a slightly lesser extent, DXA images made for other medical purposes could be appropriately used for vertebral deformity screening in clinical practice, where DXA has the advantage of lower radiation exposure.
Our study has some limitations.
It should be noted that the subjects in our study population were selected for having either normal BMD or osteoporosis and that a large proportion of this population had COPD. It is expected that COPD patients (65.5% of our study population) and subjects with osteoporosis (46%) have a higher prevalence of vertebral deformities than healthy subjects. Prevalence of a condition (vertebral deformities) does influence PPV and NPV, so our results can only be applied to populations with a similar prevalence of vertebral deformities. However, in populations with high prevalence of vertebral deformities, looking for vertebral deformities on medical images made for other indications is probably of more interest than in low-risk patient groups.
Since DXA scans were performed later than X-ray and CCT, with an average time interval of 157 ± 166.6 days, this could have influenced our results, due to (new) vertebral deformities that may occur within 1 year, especially if subjects already have vertebral deformities [18].
After recalculation of results with exclusion of 32 resp. 19 subjects with a DXA delay of more than 6 resp. 12 months, no differences were found (data not shown). Therefore, we have no reason to believe that the time interval between DXA and the other two imaging modalities may have influenced sensitivity, specificity, PPV, NPV and AUROC for DXA.
Another limitation is the difference between vertebral fractures and vertebral deformities. When diagnosing vertebral fractures in clinical practice, qualitative features of morphology and medical context should be taken into account. We scored the vertebral deformities based on height measurements using SpineAnalyzer, and although we avoided misclassification of deformities due to fusion of adjacent vertebrae or Schmorl’s nodes, we have not taken all qualitative features of morphology and medical context into account. Therefore, we cannot be entirely sure we measured fractures exclusively and no deformations due to degenerative remodelling.
Our main focus of interest was the influence of the different imaging modalities on visualisation of deformations, and therefore, we have chosen to measure deformities rather than only fractures. Whether a mild deformity on an image in clinical setting is an osteoporotic fracture or a deformity of other nature (such as degenerative deformation) should be evaluated by the treating physician, who is familiar with the clinical context.
Lastly, it should be noted that we only investigated vertebrae from T4 to L1. In X-ray and CCT images made for pulmonary evaluation, often only the thoracic vertebrae and possibly L1 are visible and therefore our findings cannot be applied to the lumbar spine.
Conclusion
This study showed that reproducibility of height measurement of vertebrae is excellent with all three imaging modalities. On vertebral level, the NPV is very high but PPV is lower, especially for DXA. On subject level, diagnostic performance of CT (PPV 79–82%; NPV 90–93%), and to a slightly lesser extend of DXA (PPV 73–77%; NPV 80–89%), indicates that these imaging techniques could be used for opportunistic screening for vertebral deformities in patients with COPD.
References
Okazaki R, Watanabe R, Inoue D (2016) Osteoporosis associated with chronic obstructive pulmonary disease. J Bone Metab 23(3):111–120. https://doi.org/10.11005/jbm.2016.23.3.111
Conradie M, Conradie MM, Scher AT, Kidd M, Hough S (2015) Vertebral fracture prevalence in black and white south African women. Arch Osteoporos 10(1):203. https://doi.org/10.1007/s11657-015-0203-x
Marwaha RK, Tandon N, Gupta Y, Bhadra K, Narang A, Mani K, Mithal A, Kukreja S (2012) The prevalence of and risk factors for radiographic vertebral fractures in older Indian women and men: Delhi vertebral osteoporosis study (DeVOS). Arch Osteoporos 7(1-2):201–207. https://doi.org/10.1007/s11657-012-0098-8
Tracy JK, Meyer WA, Grigoryan M, Fan B, Flores RH, Genant HK, Resnik C, Hochberg MC (2006) Racial differences in the prevalence of vertebral fractures in older men: the Baltimore Men's osteoporosis study. Osteoporos Int 17(1):99–104. https://doi.org/10.1007/s00198-005-1919-z
Jorgensen NR, Schwarz P, Holme I, Henriksen BM, Petersen LJ, Backer V (2007) The prevalence of osteoporosis in patients with chronic obstructive pulmonary disease: a cross sectional study. Respir Med 101(1):177–185. https://doi.org/10.1016/j.rmed.2006.03.029
McEvoy CE, Ensrud KE, Bender E, Genant HK, Yu W, Griffith JM, Niewoehner DE (1998) Association between corticosteroid use and vertebral fractures in older men with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 157(3 Pt 1):704–709. https://doi.org/10.1164/ajrccm.157.3.9703080
Nuti R, Siviero P, Maggi S, Guglielmi G, Caffarelli C, Crepaldi G, Gonnelli S (2009) Vertebral fractures in patients with chronic obstructive pulmonary disease: the EOLO study. Osteoporos Int 20(6):989–998. https://doi.org/10.1007/s00198-008-0770-4
Ogura-Tomomatsu H, Asano K, Tomomatsu K, Miyata J, Ohmori N, Kodama M, Ueda S, Takihara T, Tanaka K, Kamiishi N, Suzuki Y, Fukunaga K, Oguma T, Sayama K, Betsuyaku T (2012) Predictors of osteoporosis and vertebral fractures in patients presenting with moderate-to-severe chronic obstructive lung disease. Copd 9(4):332–337. https://doi.org/10.3109/15412555.2012.667850
Papaioannou A, Parkinson W, Ferko N, Probyn L, Ioannidis G, Jurriaans E, Cox G, Cook RJ, Kumbhare D, Adachi JD (2003) Prevalence of vertebral fractures among patients with chronic obstructive pulmonary disease in Canada. Osteoporos Int 14(11):913–917. https://doi.org/10.1007/s00198-003-1449-5
Watanabe R, Tanaka T, Aita K, Hagiya M, Homma T, Yokosuka K, Yamakawa H, Yarita T, Tai N, Hirano J, Inoue D, Okazaki R (2015) Osteoporosis is highly prevalent in Japanese males with chronic obstructive pulmonary disease and is associated with deteriorated pulmonary function. J Bone Miner Metab 33(4):392–400. https://doi.org/10.1007/s00774-014-0605-7
Pluijm SM, Tromp AM, Smit JH, Deeg DJ, Lips P (2000) Consequences of vertebral deformities in older men and women. J Bone Miner Res 15(8):1564–1572. https://doi.org/10.1359/jbmr.2000.15.8.1564
Cortet B, Roches E, Logier R, Houvenagel E, Gaydier-Souquieres G, Puisieux F, Delcambre B (2002) Evaluation of spinal curvatures after a recent osteoporotic vertebral fracture. Joint Bone Spine 69(2):201–208
Wei Y, Tian W, Zhang GL, Lv YW, Cui GY (2017) Thoracolumbar kyphosis is associated with compressive vertebral fracture in postmenopausal women. Osteoporos Int 28(6):1925–1929. https://doi.org/10.1007/s00198-017-3971-x
Ismail AA, Cockerill W, Cooper C, Finn JD, Abendroth K, Parisi G, Banzer D, Benevolenskaya LI, Bhalla AK, Armas JB, Cannata JB, Delmas PD, Dequeker J, Dilsen G, Eastell R, Ershova O, Falch JA, Felsch B, Havelka S, Hoszowski K, Jajic I, Kragl U, Johnell O, Lopez Vaz A, Lorenc R, Lyritis G, Marchand F, Masaryk P, Matthis C, Miazgowski T, Pols HA, Poor G, Rapado A, Raspe HH, Reid DM, Reisinger W, Janott J, Scheidt-Nave C, Stepan J, Todd C, Weber K, Woolf AD, Ambrecht G, Gowin W, Felsenberg D, Lunt M, Kanis JA, Reeve J, Silman AJ, O'Neill TW (2001) Prevalent vertebral deformity predicts incident hip though not distal forearm fracture: results from the European prospective osteoporosis study. Osteoporos Int 12(2):85–90. https://doi.org/10.1007/s001980170138
Karlsson MK, Kherad M, Hasserius R, Nilsson JA, Redlund-Johnell I, Ohlsson C, Lorentzon M, Mellstrom D, Rosengren BE (2016) Characteristics of prevalent vertebral fractures predict new fractures in elderly men. J Bone Joint Surg Am 98(5):379–385. https://doi.org/10.2106/JBJS.15.00328
Schousboe JT, Vo T, Taylor BC, Cawthon PM, Schwartz AV, Bauer DC, Orwoll ES, Lane NE, Barrett-Connor E, Ensrud KE (2016) Prediction of incident major osteoporotic and hip fractures by trabecular bone score (TBS) and prevalent radiographic vertebral fracture in older men. J Bone Miner Res 31(3):690–697. https://doi.org/10.1002/jbmr.2713
Black DM, Arden NK, Palermo L, Pearson J, Cummings SR (1999) Prevalent vertebral deformities predict hip fractures and new vertebral deformities but not wrist fractures. Study of osteoporotic fractures research group. J Bone Miner Res 14(5):821–828. https://doi.org/10.1359/jbmr.1999.14.5.821
Lindsay R, Silverman SL, Cooper C, Hanley DA, Barton I, Broy SB, Licata A, Benhamou L, Geusens P, Flowers K, Stracke H, Seeman E (2001) Risk of new vertebral fracture in the year following a fracture. JAMA 285(3):320–323. https://doi.org/10.1001/jama.285.3.320
Johnell O, Kanis JA, Oden A, Sernbo I, Redlund-Johnell I, Petterson C, De Laet C, Jonsson B (2004) Mortality after osteoporotic fractures. Osteoporos Int 15(1):38–42. https://doi.org/10.1007/s00198-003-1490-4
Kado DM, Browner WS, Palermo L, Nevitt MC, Genant HK, Cummings SR (1999) Vertebral fractures and mortality in older women: a prospective study. Study of osteoporotic fractures research group. Arch Intern Med 159(11):1215–1220. https://doi.org/10.1001/archinte.159.11.1215
Harrison RA, Siminoski K, Vethanayagam D, Majumdar SR (2007) Osteoporosis-related kyphosis and impairments in pulmonary function: a systematic review. J Bone Miner Res 22(3):447–457. https://doi.org/10.1359/jbmr.061202
Gehlbach SH, Bigelow C, Heimisdottir M, May S, Walker M, Kirkwood JR (2000) Recognition of vertebral fracture in a clinical setting. Osteoporos Int 11(7):577–582. https://doi.org/10.1007/s001980070078
Kim YM, Demissie S, Eisenberg R, Samelson EJ, Kiel DP, Bouxsein ML (2011) Intra-and inter-reader reliability of semi-automated quantitative morphometry measurements and vertebral fracture assessment using lateral scout views from computed tomography. Osteoporos Int 22(10):2677–2688. https://doi.org/10.1007/s00198-011-1530-4
Takada M, Wu CY, Lang TF, Genant HK (1998) Vertebral fracture assessment using the lateral scoutview of computed tomography in comparison with radiographs. Osteoporos Int 8(3):197–203. https://doi.org/10.1007/s001980050054
Lee JH, Cho SK, Han M, Lee S, Kim JY, Ryu JA, Choi YY, Bae SC, Sung YK (2014) Validity and role of vertebral fracture assessment in detecting prevalent vertebral fracture in patients with rheumatoid arthritis. Joint Bone Spine 81(2):149–153. https://doi.org/10.1016/j.jbspin.2013.07.003
Lee JH, Lee YK, Oh SH, Ahn J, Lee YE, Pyo JH, Choi YY, Kim D, Bae SC, Sung YK, Kim DY (2016) A systematic review of diagnostic accuracy of vertebral fracture assessment (VFA) in postmenopausal women and elderly men. Osteoporos Int 27(5):1691–1699. https://doi.org/10.1007/s00198-015-3436-z
Romme EA, Murchison JT, Phang KF, Jansen FH, Rutten EP, Wouters EF, Smeenk FW, Van Beek EJ, Macnee W (2012) Bone attenuation on routine chest CT correlates with bone mineral density on DXA in patients with COPD. J Bone Miner Res 27(11):2338–2343. https://doi.org/10.1002/jbmr.1678
Rabe KF, Hurd S, Anzueto A, Barnes PJ, Buist SA, Calverley P, Fukuchi Y, Jenkins C, Rodriguez-Roisin R, van Weel C, Zielinski J (2007) Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med 176(6):532–555. https://doi.org/10.1164/rccm.200703-456SO
CBO (2011) Richtlijn Osteoporose en fractuurpreventie derde herziening (2011). http://www.ephor.nl/media/1112/richtlijn-osteoporose-28-04-2011.pdf
Brett A, Miller CG, Hayes CW, Krasnow J, Ozanian T, Abrams K, Block JE, van Kuijk C (2009) Development of a clinical workflow tool to enhance the detection of vertebral fractures: accuracy and precision evaluation. Spine (Phila Pa 1976) 34(22):2437–2443. https://doi.org/10.1097/BRS.0b013e3181b2eb69
van der Velde R, Ozanian T, Dumitrescu B, Haslam J, Staal J, Brett A, van den Bergh J, Geusens P (2015) Performance of statistical models of shape and appearance for semiautomatic segmentations of spinal vertebrae T4-L4 on digitized vertebral fracture assessment images. Spine J 15(6):1248–1254. https://doi.org/10.1016/j.spinee.2015.02.018
Genant HK, Wu CY, van Kuijk C, Nevitt MC (1993) Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res 8(9):1137–1148. https://doi.org/10.1002/jbmr.5650080915
Cicchetti C (1994) Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol Assess 6(4):284–290. https://doi.org/10.1037/1040-3590.6.4.284
Bazzocchi A, Spinnato P, Fuzzi F, Diano D, Morselli-Labate AM, Sassi C, Salizzoni E, Battista G, Guglielmi G (2012) Vertebral fracture assessment by new dual-energy X-ray absorptiometry. Bone 50(4):836–841. https://doi.org/10.1016/j.bone.2012.01.018
Binkley N, Krueger D, Gangnon R, Genant HK, Drezner MK (2005) Lateral vertebral assessment: a valuable technique to detect clinically significant vertebral fractures. Osteoporos Int 16(12):1513–1518. https://doi.org/10.1007/s00198-005-1891-7
Damiano J, Kolta S, Porcher R, Tournoux C, Dougados M, Roux C (2006) Diagnosis of vertebral fractures by vertebral fracture assessment. J Clin Densitom 9(1):66–71. https://doi.org/10.1016/j.jocd.2005.11.002
Diacinti D, Del Fiacco R, Pisani D, Todde F, Cattaruzza MS, Arima S, Romagnoli E, Pepe J, Cipriani C, Minisola S (2012) Diagnostic performance of vertebral fracture assessment by the lunar iDXA scanner compared to conventional radiography. Calcif Tissue Int 91(5):335–342. https://doi.org/10.1007/s00223-012-9643-0
Diacinti D, Guglielmi G, Pisani D, Argiro R, Serafini C, Romagnoli E, Minisola S, Catalano C, David V (2012) Vertebral morphometry by dual-energy X-ray absorptiometry (DXA) for osteoporotic vertebral fractures assessment (VFA). Radiol Med 117(8):1374–1385. https://doi.org/10.1007/s11547-012-0835-5
Domiciano DS, Figueiredo CP, Lopes JB, Kuroishi ME, Takayama L, Caparbo VF, Fuller P, Menezes PF, Scazufca M, Bonfa E, Pereira RM (2013) Vertebral fracture assessment by dual X-ray absorptiometry: a valid tool to detect vertebral fractures in community-dwelling older adults in a population-based survey. Arthritis Care Res (Hoboken) 65(5):809–815. https://doi.org/10.1002/acr.21905
Hospers IC, van der Laan JG, Zeebregts CJ, Nieboer P, Wolffenbuttel BH, Dierckx RA, Kreeftenberg HG, Jager PL, Slart RH (2009) Vertebral fracture assessment in supine position: comparison by using conventional semiquantitative radiography and visual radiography. Radiology 251(3):822–828. https://doi.org/10.1148/radiol.2513080887
Rea JA, Li J, Blake GM, Steiger P, Genant HK, Fogelman I (2000) Visual assessment of vertebral deformity by X-ray absorptiometry: a highly predictive method to exclude vertebral deformity. Osteoporos Int 11(8):660–668. https://doi.org/10.1007/s001980070063
Chapurlat RD, Duboeuf F, Marion-Audibert HO, Kalpakcioglu B, Mitlak BH, Delmas PD (2006) Effectiveness of instant vertebral assessment to detect prevalent vertebral fracture. Osteoporos Int 17(8):1189–1195. https://doi.org/10.1007/s00198-006-0121-2
Sullivan S, Wagner J, Resnick NM, Nelson J, Perera SK, Greenspan SL (2011) Vertebral fractures and the misclassification of osteoporosis in men with prostate cancer. J Clin Densitom 14(3):348–353. https://doi.org/10.1016/j.jocd.2011.05.003
Vokes TJ, Dixon LB, Favus MJ (2003) Clinical utility of dual-energy vertebral assessment (DVA). Osteoporos Int 14(11):871–878. https://doi.org/10.1007/s00198-003-1461-9
Deleskog L, Laursen NO, Nielsen BR, Schwarz P (2016) Vertebral fracture assessment by DXA is inferior to X-ray in clinical severe osteoporosis. Osteoporos Int 27(7):2317–2326. https://doi.org/10.1007/s00198-016-3532-8
Acknowledgements
This work was funded by Stichting De Weijerhorst
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
MJ van Dort has nothing to disclose.
EAPM Romme has nothing to disclose.
FWJM Smeenk has nothing to disclose.
PPPM Geusens reports grants and speaker fees from Amgen, grants from Pfizer, grants from MSD, grants from UCB, grants from Abbott, grants and speaker fees from Lilly, grants from BMS, grants from Novartis, grants from Roche, grants from Will Pharma, outside the submitted work.
EFM Wouters reports personal fees from Nycomed, personal fees from Boehringer, grants and speaker fees from AstraZeneca, grants and speaker fees from GSK, speaker fees from Novartis, speaker fees from Chiesi, outside the submitted work.
JP van den Bergh reports grants from Eli Lilly, grants from Will Pharma, grants from Amgen, outside the submitted work.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

{kind=link}
{kind=link}
Cite this article
van Dort, M.J., Romme, E.A.P.M., Smeenk, F.W.J.M. et al. Diagnosis of vertebral deformities on chest CT and DXA compared to routine lateral thoracic spine X-ray. Osteoporos Int 29, 1285–1293 (2018). https://doi.org/10.1007/s00198-018-4412-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-018-4412-1