
Abstract
Summary
A total of 2,266 postmenopausal Chinese women were followed for 4.5 years to determine the incidence of new fractures. The positive predictive value, negative predictive value, sensitivity and specificity of different treatment strategies were compared. Using a fixed optimal threshold calculated from receiver operating characteristics (ROC) curve had the highest sensitivity but lowest specificity.
Introduction
There is no specific intervention threshold based on FRAX to guide treatment for Asian populations. This prospective study sought to determine the impact of applying different intervention thresholds to a cohort of Chinese postmenopausal women.
Methods
This study was part of the Hong Kong Osteoporosis Study. A total of 2,266 treatment-naïve postmenopausal women underwent clinical risk factor and BMD assessments. The subjects were followed to assess fractures. We calculated the FRAX probability of major osteoporotic fractures corresponding to women with prior fractures but no other clinical risk factors. Different treatment strategies which include treating women with prior fractures, women with age-specific FRAX probability corresponding to those with prior fractures, women with osteoporosis as well as women with FRAX probability above a fixed cut-off based on optimizing sensitivity and specificity on the ROC curve were compared.
Results
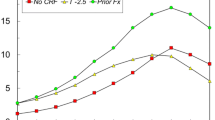
The mean age at baseline was 62.1 ± 8.5 years, and the mean follow-up time was 4.5 ± 2.8 years. One hundred six new major osteoporotic fractures were reported. An optimal (FRAX, with BMD) cut-off point of 9.95 % was identified. All strategies had negative predictive value of >90 %. Using a fixed cut-off had the highest sensitivity (62.3 %) but lowest specificity (73.5 %) and positive predictive value (10.3 %). Using a fixed cut-off would direct treatment from younger women with lower absolute risk to elderly women with higher absolute risk.
Conclusion
Targeting only women with prior fractures is unlikely to reduce fracture burden. Other treatment strategies with higher sensitivity need to be considered but they have different shortcomings


Similar content being viewed by others


References
Siris ES, Chen YT, Abbott TA et al (2004) Bone mineral density thresholds for pharmacological intervention to prevent fractures. Arch Intern Med 164(10):1108–1112
Schuit SC, Van der Klift M, de Laet CE et al (2004) Fracture incidence and association with bone mineral density in elderly men and women: the Rotterdam study. Bone 34(1):195–202
Pasco JA, Seeman E, Henry MJ et al (2006) The population burden of fractures originates in women with osteopenia not osteoporosis. Osteoporos Int 17(9):1404–1409
Kanis JA, Oden A, Johnell O et al (2007) The use of clinical risk factors enhances the performance of BMD in the prediction of hip and osteoporotic fractures in men and women. Osteoporos Int 18:1033–1046
McCloskey E, Kanis JA (2012) FRAX updates 2012. Curr Opin Rheumatol 24(5):554–560
Nguyen ND, Frost SA, Center JR et al (2008) Development of prognostic nomograms for individualizing 5-year and 10-year fracture risks. Osteoporos Int 19:1431–1444
Hippisley-Cox J, Coupland C (2009) Predicting risk of osteoporotic fracture in men and women in England and Wales: prospective derivation and validation of QFractureScores. BMJ 339:b4229
Cooper C, Melton LJ (1992) Hip fractures in the elderly: a world-wide projection. Osteoporos Int 2:285–289
Kanis JA, on behalf of the World Health Organization Scientific Group (2008) Assessment of osteoporosis at the primary health-care level. Technical Report. WHO Collaborating Centre, University of Sheffield, UK. http://www.shef.ac.uk/FRAX/pdfs/WHO_Technical_Report.pdf. Assessed 8 January 2013
Kanis JA, McCloskey EV, Johansson H et al (2008) Case finding for the management of osteoporosis with FRAX—assessment and intervention thresholds for the UK. Osteoporos Int 19:1395–1408
Compston J, Cooper A, Cooper C et al (2009) Guidelines for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK. Maturitas 62:105–108
Briot K, Cortet B, Thomas T et al (2012) 2012 update of French guidelines for the pharmacological treatment of postmenopausal osteoporosis. Joint Bone Spine 79:304–313
Kanis JA, McCloskey EV, Johansson H, Scientific Advisory Board of the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO) and the Committee of Scientific Advisors of the International Osteoporosis Foundation (IOF) et al (2013) European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int 24(1):23–57
Orimo H, Hayashi Y, Fukunaga M et al (2001) Diagnostic criteria for primary osteoporosis: year 2000 revision. J Bone Miner Metab 19:331–337
Tosteson AN, Melton LJ 3rd, Dawson-Hughes B, National Osteoporosis Foundation Guide Committee et al (2008) Cost-effective osteoporosis treatment thresholds: the United States perspective. Osteoporos Int 19(4):437–447
Dawson-Hughes B, Tosteson AN, Melton LJ 3rd, National Osteoporosis Foundation Guide Committee et al (2008) Implications of absolute fracture risk assessment for osteoporosis practice guidelines in the USA. Osteoporos Int 19(4):449–458
OSHK Task Group for Formulation of 2013 OSHK Guideline for Clinical Management of Postmenopausal Osteoporosis in Hong Kong, Ip I, Cheung SK, Cheung TC et al (2013) The Osteoporosis Society of Hong Kong (OSHK): 2013 OSHK guideline for clinical management of postmenopausal osteoporosis in Hong Kong. Hong Kong Med J 19(Suppl 2):1–40
Cheung EY, Bow CH, Cheung CL et al (2012) Discriminative value of FRAX for fracture prediction in a cohort of Chinese postmenopausal women. Osteoporos Int 23(3):871–878
Bewick V, Cheek L, Ball J (2004) Statistics review 13: receiver operating characteristic curves. Crit Care 8(6):508–512
Youden WJ (1950) Index for rating diagnostic tests. Cancer 3(1):32–33
Perkins NJ, Schisterman EF (2006) The inconsistency of “optimal” cut-points using two ROC based criteria. Am J Epidemiol 163(7):670–675
Coffin M, Sukhatme S (1997) Receiver operating characteristic studies and measurement errors. Biometrics 53:823–837
Sharir T, Berman DS, Waechter PB et al (2001) Quantitative analysis of regional motion and thickening by gated myocardial perfusion SPECT: normal heterogeneity and criteria for abnormality. J Nucl Med 42:1630–1638
Report of Hospital Authority, Hong Kong, 1996
Lippuner K, Johansson H, Borgström F et al (2012) Cost-effective intervention thresholds against osteoporotic fractures based on FRAX® in Switzerland. Osteoporos Int 23(11):2579–2589
Lippuner K (2012) Osteoporosis—whom to treat? The importance of FRAX® in Switzerland. Ther Umsch 69(3):207–213
Bolland MJ, Grey A (2010) Disparate outcomes from applying U.K. and U.S. osteoporosis treatment guidelines. J Clin Endocrinol Metab 95(4):1856–1860
Orimo H, Nakamura T, Hosoi T et al (2012) Japanese 2011 guidelines for prevention and treatment of osteoporosis—executive summary. Arch Osteoporos 7(1–2):3–20
Fujiwara S, Nakamura T, Orimo H (2008) Development and application of a Japanese model of the WHO fracture risk assessment tool (FRAX). Osteoporos Int 19(4):429–435
Kanis JA, Johansson H, Oden A et al (2012) The distribution of FRAX(®)-based probabilities in women from Japan. J Bone Miner Metab 30(6):700–705
Committee for Medicinal Products for Human Use (CHMP) (2006) Guideline on the evaluation of Medicinal products in the treatment of primary osteoporosis. CHMP, London, Ref CPMP/EWP/552/95Rev.2. Nov 2006
Kanis JA, McCloskey E, Johansson H et al (2012) FRAX with and without BMD. Calcif Tissue Int 90:1–13
Kanis JA, Johansson H, Ode'n A et al (2009) Bazedoxifene reduces vertebral and clinical fractures in postmenopausal women at high risk assessed with FRAX. Bone (NY) 44:1049–1054
McCloskey EV, Johansson H, Ode'n A et al (2009) Ten-year fracture probability identifies women who will benefit from clodronate therapy—additional results from a double blind, placebo controlled randomised study. Osteoporos Int 20:811–818
McCloskey EV, Johansson H, Oden A et al (2012) Denosumab reduces the risk of all osteoporotic fractures in postmenopausal women, particularly in those with moderate to high fracture risk as assessed with FRAX. J Bone Miner Res 27(7):1480–1486
Kanis JA, Oden A, Johansson H (2012) Pitfalls in the external validation of FRAX. Osteoporos Int 23(2):423–431
Acknowledgments
We would like to acknowledge the staff of the Osteoporosis Centre, Queen Mary Hospital, and the Osteoporosis and Endocrine Research Fund, University of Hong Kong. We would also like to thank Xiao SM for statistical support.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cheung, E., Cheung, CL., Kung, A.W.C. et al. Possible FRAX-based intervention thresholds for a cohort of Chinese postmenopausal women. Osteoporos Int 25, 1017–1023 (2014). https://doi.org/10.1007/s00198-013-2553-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-013-2553-9