
Abstract
Summary
Assessment and intervention thresholds are developed and proposed in men aged over 50 years and postmenopausal women for the UK based on fracture probability from the WHO fracture risk assessment tool (FRAX®).
Introduction
The FRAX® tool has recently become available to compute the 10-year probability of fractures in men and women from clinical risk factors (CRFs) with or without the measurement of femoral neck bone mineral density (BMD). The aim of this study was to develop a case-finding strategy for men and women from the UK at high risk of osteoporotic fracture by delineating the fracture probabilities at which BMD testing or intervention should be recommended.
Methods
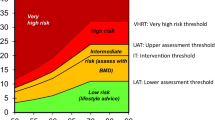
Fracture probabilities were computed using the FRAX® tool calibrated to the epidemiology of fracture and death in the UK. The relationship between cost effectiveness and fracture probability used the source data from a prior publication that examined the cost effectiveness of generic alendronate in the UK. An intervention threshold was set by age in men and women, based on the fracture probability equivalent to that of women with a history of a prior osteoporosis related fracture. In addition, assessment thresholds for the use of BMD testing were explored. Assessment thresholds for the measurement of BMD followed current practice guidelines where individuals were considered to be eligible for assessment in the presence of one or more CRF. An upper assessment threshold (i.e. a fracture probability above which patients could be treated without recourse to BMD) was based on optimisation of the positive predictive value of the assessment tool. The consequences of assessment and intervention thresholds on the requirement for BMD test and interventions were assessed using the distribution of clinical risk factors and femoral neck BMD for women in the source cohorts used for the development of the FRAX® models
Results
Treatment was cost effective at all ages when the 10-year probability of a major fracture exceeded 7%. The intervention threshold at the age of 50 years corresponded to a 10-year probability of a major osteoporotic fracture of 7.5%. This rose progressively with age to 30% at the age of 80 years, so that intervention was cost effective at all ages. Assessment thresholds for testing with BMD (6–9% at the age of 50 years) also rose with age (18–36% at the age of 80 years). The use of these thresholds in a case-finding strategy would identify 6–20% of women as eligible for BMD testing and 23–46% as eligible for treatment, depending on age. The same threshold can be used in men.
Conclusion
The study provides a method of developing management algorithms for osteoporosis from the estimation of fracture probabilities, rather than those based on BMD alone or BMD with single or multiple CRFs.




Similar content being viewed by others

References
Royal College of Physicians (1999) Osteoporosis: clinical guidelines for the prevention and treatment 1999. Royal College of Physicians, London
Royal College of Physicians and Bone and Tooth Society of Great Britain (2000) Update on pharmacological interventions and an algorithm for management 2000. Royal College of Physicians, London
Royal College of Physicians (2002) Glucocorticoid-induced osteoporosis. Guidelines on prevention and treatment. Bone and Tooth Society of Great Britain, National Osteoporosis Society and Royal College of Physicians. Royal College of Physicians, London
Kanis JA, Delmas P, Burckhardt P, Cooper C, Torgerson D, European Foundation for Osteoporosis and Bone Disease (1997) Guidelines for diagnosis and management of osteoporosis, Osteoporos Int 7:390–406
Kanis JA, Burlet N, Cooper C, Delmas PD, Reginster J-Y, Borgstrom F, Rizzoli R, European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO) (2008) European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int 19:399–428
European Community (1998) Report on osteoporosis in the European Community. EC, Strasbourg
Kanis JA (2002) Diagnosis of osteoporosis and assessment of fracture risk. Lancet 359:1929–1936
De Laet C, Oden A, Johansson H, Johnell O, Jonsson B, Kanis JA (2005) The impact of the use of multiple risk indicators for fracture on case-finding strategies: a mathematical approach. Osteoporos Int 16:313–318
Kanis JA, Borgstrom F, De Laet C, Johansson H, Johnell O, Jonsson B et al (2005) Assessment of fracture risk. Osteoporos Int 16:581–589
Kanis JA, Oden A, Johnell O, Johansson H, De Laet C, Brown J et al (2007) The use of clinical risk factors enhances the performance of BMD in the prediction of hip and osteoporotic fractures in men and women. Osteoporos Int 18:1033–1046
Kanis JA, Johnell O, Oden A, Johansson H, McCloskey EV (2008) FRAX® and the assessment of fracture probability in men and women from the UK. Osteoporos Int 19:385–397
Committee for Medicinal Products for Human Use (CHMP) (2006) Guideline on the evaluation of medicinal products in the treatment of primary osteoporosis. Ref CPMP/EWP/552/95Rev.2. London, CHMP. Nov 2006
Kanis JA, Borgstrom F, Zethraeus N, Johnell O, Oden A, Jonsson B (2005) Intervention thresholds for osteoporosis in the UK. Bone 36:22–32
De Laet C, Kanis JA, Oden A, Johanson H, Johnell O, Delmas P et al (2005) Body mass index as a predictor of fracture risk: a meta-analysis. Osteoporos Int 16:1330–1338
Kanis JA, Johnell O, De Laet C, Johansson H, Oden A, Delmas P et al (2004) A meta-analysis of previous fracture and subsequent fracture risk. Bone 35:375–82
Kanis JA, Johansson H, Oden A, Johnell O, De Laet C, Eisman J et al (2004) A family history of fracture and fracture risk. Bone 35:1029–1037
Kanis JA, Johansson H, Oden A, Johnell O, De Laet C, Melton LJ III et al (2004) A meta-analysis of prior corticosteroid use and fracture risk. J Bone Miner Res 19:893–899
Kanis JA, Johnell O, Oden A, Johansson H, De Laet C, Eisman JA et al (2005) Smoking and fracture risk: a meta-analysis. Osteoporos Int 16:222–228
Kanis JA, Johansson H, Johnell O, Oden A, De Laet C, Eisman J et al (2005) Alcohol intake as a risk factor for fracture. Osteoporos Int 16:737–42
Kanis JA, on behalf of the World Health Organization Scientific Group (2008) Assessment of osteoporosis at the primary health-care level. Technical Report. WHO Collaborating Centre, University of Sheffield, UK
World Health Organization (2007) Assessment of osteoporosis at the primary health care level. Summary Report of a WHO Scientific Group. WHO, Geneva www.who.int/chp/topics/rheumatic/en/index.html
Kanis JA, Adams J, Borgström F, Cooper C, Jönsson B, Preedy D et al (2008) The cost-effectiveness of alendronate in the management of osteoporosis. Bone 42:4–15
Stevenson M, Lloyd Jones M, De Nigris E, Brewer N, Davis S, Oakley J (2005) A systematic review and economic evaluation of alendronate, etidronate, risedronate, raloxifene and teriparatide for the prevention and treatment of postmenopausal osteoporosis. Health Technol Assess 9:1–160
Eichler HG, Kong SX, Gerth WC, Mavros P, Jonsson B (2004) Use of cost-effectiveness analysis in health-care resource allocation decision-making: how are cost-effectiveness thresholds expected to emerge. Value Health 7:518–528
Kanis JA, Jonsson B (2002) Economic evaluation of interventions for osteoporosis. Osteoporos Int 13:765–767
Kanis JA, Stevenson M, McCloskey EV, Davis S, Lloyd-Jones M (2007) Glucocorticoid-induced osteoporosis: a systematic review and cost-utility analysis. Health Technol Assess 11:1–256
National Institute for Clinical Excellence (2004) Guide to the methods of technology appraisal. Abbo Litho Sales, London
National Institute for Health and Clinical Excellence (2007) Final appraisal determination. Alendronate, etidronate, risedronate, raloxifene, strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women. NICE, London
Kanis JA, Brazier JE, Stevenson M, Calvert NW, Lloyd Jones M (2002) Treatment of established osteoporosis: a systematic review and cost-utility analysis. Health Technol Assess 6:1–146
Kanis JA, Borgstrom F, Johnell O, Jönsson B (2004) Cost-effectiveness of risedronate for the treatment of osteoporosis and prevention of fractures in postmenopausal women. Osteoporos Int 15:862–871
Kanis JA, Borgstrom F, Johnell O, Oden A, Sykes D, Jönsson B (2005) Cost-effectiveness of raloxifene in the UK. An economic evaluation based on the MORE study. Osteoporosis Int 16:15–25
Kanis JA, Johnell O, Oden A, Borgstrom F, Johansson H, De Laet C et al (2004) Intervention thresholds for osteoporosis in men and women. A study based on data from Sweden. Osteoporos Int 16:6–14
National Osteoporosis Foundation (NOF) (2003) Physician’s guide to prevention and treatment of osteoporosis. National Osteoporosis Foundation, Washington, DC
Kanis JA, Johnell O, Committee of Scientific Advisors of the International Osteoporosis Foundation (2005) Requirements for DXA for the management of osteoporosis in Europe. Osteoporos Int 16:229–238
Johansson H, Oden A, Johnell O, Jonsson B, De Laet C, Oglesby A, McCloskey EV, Kayan K, Jalava T, Kanis JA (2004) Optimisation of BMD measurements to identify high risk groups for treatment—a test analysis. J Bone Miner Res 19:906–913
Tosteson AN, Melton LJ 3rd, Dawson-Hughes B, Baim S, Favus MJ, Khosla S, Lindsay RL, National Osteoporosis Foundation Guide Committee (2008) Cost-effective osteoporosis treatment thresholds: the United States perspective. Osteoporos Int 19:437–447
Dawson-Hughes B, Tosteson AN, Melton LJ 3rd, Baim S, Favus MJ, Khosla S, Lindsay RL, National Osteoporosis Foundation Guide Committee (2008) Implications of absolute fracture risk assessment for osteoporosis practice guidelines in the USA. Osteoporos Int 19:449–458
Borgström F, Ström O, Kanis JA (2008) What proportion of patients can be treated with second line at a maintained incremental cost utility ratio. Osteoporos Int 19(Suppl 1):S65
Cummings SR, Black DM, Thompson D et al (1998) Effect of alendronate on risk of fracture in women with low bone density but without vertebral fractures: results from the Fracture Intervention Trial. JAMA 280:2077–2082
Food and Drug Administration (1994) Guidelines for preclinical and clinical evaluation of agents used in the prevention or treatment of postmenopausal osteoporosis. Division of Metabolism and Endocrine Drug Products, Rockville
Saag KG, Emkey R, Schnitzer TJ et al (1998) Alendronate for the prevention and treatment of glucocorticoid-induced osteoporosis. Glucocorticoid-induced Osteoporosis Intervention Study Group. N Engl J Med 339:292–299
Adachi JD, Saag KG, Delmas PD et al (2001) Two year effects of alendronate on bone mineral density and vertebral fracture in patients receiving glucocorticoids: a randomised, double-blind, placebo-controlled extension trial. Arthritis Rheum 44:202–211
Reginster JY, Minne HW, Sorensen OH et al (2000) Randomized trial of the effects of risedronate on vertebral fractures in women with established postmenopausal osteoporosis. Vertebral efficacy with risedronate therapy (VERT) study group. Osteoporos Int 11:83–91
Roussow JE, Anderson GL, Prentice RL, LaCroix AZ, Kooperberg C, Stefanick ML et al (2002) Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women’s Health Initiative randomized controlled trial. JAMA 288:321–333
McCloskey EV, Beneton M, Charlesworth D, Kayan K, deTakats D, Dey A et al (2007) Clodronate reduces the incidence of fractures in community dwelling elderly women unselected for osteoporosis: results of a double-blind, placebo-controlled randomized study. J Bone Miner Res 22:135–141
Chapuy MC, Arlot ME, Delmas PD, Meunier PJ (1994) Effect of calcium and cholecalciferol treatment for three years on hip fractures in elderly women. BMJ 308:1081–1082
Kanis JA, Barton I, Johnell O (2005) Risedronate decreases fracture risk in patients selected solely on the basis of prior vertebral fracture. Osteoporos Int 16:475–482
McCloskey EV, Selby P, Davies M et al (2004) Clodronate reduces vertebral fracture risk in women with post-menopausal or secondary osteoporosis: results of a double blind placebo-controlled 3 year study. J Bone Miner Res 19:728–736
Roux C, Reginster JY, Fechtenbaum J et al (2006) Vertebral fracture risk reduction with strontium ranelate in women with post-menopausal osteoporosis is independent of baseline risk factors. J Bone Miner Res 21:536–542
Marcus R, Wang O, Satterwhite J et al (2003) The skeletal response to teriparatide is largely independent of age, initial bone mineral density and prevalent vertebral fractures in postmenopausal women with osteoporosis. J Bone Miner Res 18:18–23
Johnell O, Kanis JA, Black DM et al (2004) Association between baseline risk factors and vertebral fracture risk in the Multiple Outcomes of Raloxifene Evaluation (MORE) study. J Bone Miner Res 19:764–772
McCloskey EV, Johansson H, Oden A, Aropuu S, Jalava T, Kanis JA (2007) Efficacy of clodronate on fracture risk in women selected by 10-year fracture probability. J Bone Miner Res 22(Suppl 1):S46
McClung MR, Geusens P, Miller PD, Zippel H, Bensen WG, Roux C et al (2001) Effect of risedronate on the risk of hip fracture in elderly women. Hip Intervention Program Study Group. N Engl J Med 344:333–340
Johansson H, Kanis JA, Oden A, Johnell O, McCloskey EV (2008) BMD, clinical risk factors and their combination for hip fracture prevention. Unpublished
Acknowledgements
The National Osteoporosis Guideline Group thanks the WHO Collaborating Centre for Metabolic Bone Diseases, University of Sheffield and the International Osteoporosis Foundation for supporting the meetings of NOGG.
Conflicts of interest
None.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
The National Osteoporosis Guideline Group members are Prof JE Compston (Chair), Dr AL Cooper, Prof C Cooper, Prof R Francis, Prof D Marsh, Dr EV McCloskey, Prof JA Kanis, Prof D Reid, Dr P Selby, Mrs M Wilkins.
An erratum to this article can be found at http://dx.doi.org/10.1007/s00198-008-0783-z
Rights and permissions
About this article
Cite this article
Kanis, J.A., McCloskey, E.V., Johansson, H. et al. Case finding for the management of osteoporosis with FRAX®—assessment and intervention thresholds for the UK. Osteoporos Int 19, 1395–1408 (2008). https://doi.org/10.1007/s00198-008-0712-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-008-0712-1