
Abstract
Introduction and Hypothesis
The gold standard for quantifying pelvic organ prolapse is the pelvic organ prolapse quantification (POP-Q) system; however, upright magnetic resonance imaging (MRI) is a promising new method. The objective of this study was to determine the correlation between POP-Q and MRI measurements of the bladder and cervix.
Methods
This prospective study included patients with prolapse in whom POP-Q points Aa or Ba and C were measured as standard care. MRI scans were performed in an upright position, and the distances of the lowest points of the bladder and cervix to the Pelvic Inclination Correction System (PICS) were calculated. Correlations between POP-Q and MRI-PICS measurements were determined using the Pearson correlation coefficient for normally distributed data and the Spearman’s rank correlation coefficient for non-normally distributed data.
Results
A total of 63 patients were suitable for analysis. There was a moderate positive correlation between the POP-Q and MRI-PICS measurements for bladder (r(61) = 0.480, r < 0.001) and uterus (r(61) = 0.527, p < 0.001). Measurement differences between POP-Q and MRI-PICS of the bladder and uterus vary from −3.2 cm to 7.1 cm, and from −2.1 cm to 8.5 cm respectively. In 71.4% of patients more descent was seen on upright MRI than with POP-Q measurement for both bladder and uterus. For patients with similar POP-Q measurements, a high variation in MRI measurements of the bladder and uterus was found.
Conclusion
Despite a moderate positive correlation, upright MRI shows a larger POP extent in 71.4% of the patients than POP-Q. A high variation in MRI measurements for patients with the same POP-Q measurement was seen.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pelvic organ prolapse (POP) is a common condition in women, with a reported prevalence of symptomatic POP of 11.4% [1]. POP is defined as a downward displacement of the anterior vaginal wall, the uterus or vaginal vault, the posterior vaginal wall, or a combination of any of them [2]. Correct diagnosis of POP is important as it influences treatment decisions, such as pelvic floor physiotherapy, pessary treatment, and surgical treatment [3].
The Pelvic Organ Prolapse Quantification (POP-Q) system is the gold standard for quantifying POP [4], and is the recommended system by among others the International Continence Society, American College of Obstetricians and Gynecologists, and the Royal College of Obstetricians and Gynaecologists [5,6,7]. However, this method has several limitations. First, POP-Q examination is usually performed with the patient in a dorsal lithotomy position, whereas symptoms are mostly experienced in an upright position. Previous research confirmed that intraoperative POP assessment with cervical traction revealed a larger extent of POP than was established at preoperative evaluation [8,9,10]. Second, the measurements are performed using the hymen as a reference point. The hymen is not a fixed point and will move downward with Valsalva along with the prolapsed organs [11]. Finally, the Valsalva maneuver itself, which is used for POP-Q assessment, is sometimes difficult to perform for patients. All three limitations of the POP-Q assessment can lead to underestimation of the extent of POP and can explain the poor association between POP-Q stage and severity of symptoms [12, 13]. We therefore hypothesize that POP-Q examination might not be the most reliable method of quantifying POP.
Imaging techniques, such as ultrasound and magnetic resonance imaging (MRI), have been investigated for quantifying POP. Because MRI has a good spatial resolution, large field of view, and good soft-tissue contrast, it is especially suitable for providing information about pelvic organs and supportive structures [14]. Assessment of the extent of POP based on dynamic MRI shows an outstanding inter- and intra-observer reliability, but POP quantification on supine MRI had a poor-to-moderate correlation with physical examination and POP symptoms [15,16,17]. In addition, Grob et al. concluded that MRI scanning of patients with POP stage ≥ 2 shows a significantly larger extent of the prolapse in upright rest than during a supine straining position. This indicates the need to investigate POP quantification with upright MRI and its correlation with POP-Q assessment [18]. We hypothesize that upright MRI measurements can provide a more reliable POP quantification than the POP-Q system in a dorsal lithotomy position. Therefore, in the future, upright MRI may provide a better understanding of patients’ symptoms and a better preparation for surgical treatment.
The aim of this prospective research is to establish the correlation between the distance measurements of the bladder and uterus to the pelvic inclination correction system (PICS) plane in upright MRI, and the POP-Q measurements of the anterior vaginal wall and cervix in patients with POP.
Materials and Methods
Population
Magnetic resonance imaging scans and POP-Q measurements of patients with POP recruited for two different POP studies were included in this study. Consecutive patients were recruited between 2021 and 2023 from the gynecology department of the Ziekenhuisgroep Twente hospital in Almelo and Hengelo, the Netherlands. Both studies were approved by the medical ethics committee (NL74061.091.20 and NL79717.091.21) and all patients gave written informed consent. Patients were not involved in the designing or conducting of the research. All women were 18 years or older and had a minimum stage 2 prolapse of the anterior vaginal wall or uterus, and had not undergone previous POP surgery. As prolapse of the posterior compartment is difficult to visualize on MRI without using rectal contrast, patients with primarily a posterior vaginal wall prolapse were not included in the study. Patients were excluded if they were not able to stand for 20 min without assistance, were not eligible to undergo an MRI scan in response to an MRI safety checklist, or had a jeans size ≥ 52 (EU) or 22 (US), because of the limited coil circumference.
MRI Examination
Magnetic resonance scans of the women in an upright position and the pelvis at rest were acquired. The participants were not allowed to drink for 1 h before the scan and had to empty their bladder within 15 min before the scan. A tiltable 0.25 T MR scanner (G-Scan Brio; Esaote S.p.A., Genoa, Italy) was used for MRI acquisition, with a dedicated multichannel spine coil. A 3D balanced steady-state free precession sequence was acquired in an upright patient position (TE/TR: 4/8 ms, flip angle: 60°, reconstructed resolution: 0.49 × 0.49 × 0.49 mm3, FOV: 250 × 250 × 122 mm3 or 250 × 250 × 160 mm3, acquisition matrix 124 × 124 × 100, number signal averages 3, scan time: ± 5 min).
POP Measurements
In all women a POP-Q measurement in a dorsal lithotomy position, and under maximum Valsalva had been performed as part of standard care by one of the urogynecologists. Points “Aa” or “Ba” (whichever showed the highest value) were used for the quantification of the anterior vaginal wall (from now on called “bladder”) prolapse, and “C” was used for the uterus prolapse.
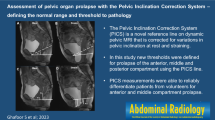
To measure the extent of POP with MRI several reference lines have been proposed over time [19]. In 2017 Reiner et al. introduced the Pelvic Inclination Correction System, which has several advantages over the other reference lines, including the possibility of evaluating POP in three dimensions (3D) [20]. The method was validated for upright MRI, using a 29° PICS angle, by Morsinkhof et al. [21]. The MRI-PICS plane was determined by manually selecting the right ischial spine, the left ischial spine, the inferior pubic point, and the sacrococcygeal joint, as described by Reiner et al. [20]. Following the selection of the PICS plane the lowest points of the bladder and uterus were annotated manually on sagittal MRI slices using a 3D slicer (v.5.0.2) [22]. The rectum was not taken into account in these measurements as it was not possible to visualize the lowest point without the use of rectal contrast. After annotation, the coordinates of the points were exported to MATLAB (R2022a; MathWorks Inc., Natick, MA, USA). In MATLAB the perpendicular distances of the bladder and uterus to the PICS plane were calculated, where the negative values represent a position cranial from the PICS plane and the positive values a point caudal from the PICS plane. All MRI measurements were performed by one of the researchers (KJ) and when in doubt double checked by a second researcher (AS). The researchers were blinded to the POP-Q measurements during the performance of the MRI measurements.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics (version 28.0.1.0, SPSS Inc., Chicago, IL, USA). Normality of the data was assessed by means of the Shapiro–Wilk test. The correlation between the POP-Q measurements and the MRI-PICS measurements were determined by the Pearson correlation coefficient for the normally distributed data and by the Spearman’s rank correlation coefficient for the non-normally distributed data. A statistical significance level of 5% was used for both correlations.
Results
Out of a total of 76 eligible patients, 13 patients were excluded because no POP-Q was available (n = 4), no upright MRI scan was available because of the patients fainting in an upright position (n = 2), because the field of view (FOV) of the MRI scan was too small (n = 5), or because the MRI scan had insufficient image quality (n = 2), leaving 63 patients for analysis (Fig. 1).

Flowchart of the patient inclusion and exclusion process. POP-Q Pelvic Organ Prolapse Quantification, MRI magnetic resonance imaging, FOV field of view
Table 1 shows the baseline characteristics of the study population with the POP-Q stage of the bladder and uterus.
The Shapiro–Wilk test showed that the POP-Q (W = 0.966, p = 0.077) and MRI-PICS (W = 0.965, p = 0.074) measurements for the bladder can be assumed to be normally distributed. For the uterus the POP-Q (W = 0.962, p = 0.049) and MRI-PICS (W = 0.934, p = 0.002) measurements were significantly different from normally distributed data.
The Pearson correlation coefficient indicated a moderate positive correlation between the POP-Q bladder measurements and the MRI-PICS bladder measurements (r(61) = 0.480, p < 0.001). The Spearman’s rank correlation coefficient indicated a moderate positive correlation between the POP-Q uterus measurements and the MRI-PICS uterus measurements (r(61) = 0.527, p < 0.001).
Bladder
Figure 2 shows a scatterplot of the POP-Q and MRI-PICS measurements of the bladder, indicating the variety of MRI-PICS measurements per POP-Q outcome. For instance, when considering the bladder at POP-Q measurement + 1, a large variation in MRI-PICS measurements was found, with differences up to 7.1 cm between patients. Figure 3 illustrates the discrepancy between POP-Q and MRI-PICS measurements per patient, identifying three groups: patients in whom the MRI-PICS measurement is smaller (difference < −0.5 cm) than the POP-Q measurement (n = 9 [14.3%]); patients in whom the measurements were almost identical (absolute difference < 0.5 cm; n = 9 [14.3%]); and patients in whom the MRI-PICS measurement was larger (difference > 0.5 cm) than the POP-Q measurement (n = 45 [71.4%]). The measurement differences between the POP-Q and the MRI-PICS of the bladder vary from −3.2 cm to 7.1 cm.

Scatterplot of the Pelvic Organ Prolapse Quantification (POP-Q) and magnetic resonance imaging-Pelvic Inclination Correction system (MRI-PICS) measurements of the bladder. POP-Q (x-axis) and MRI-PICS (y-axis) measurements of the bladder showing that MRI-PICS measurements are often larger. Data points are color labeled by POP-Q stage. The green line represents the reference line at which POP-Q and MRI-PICS values are equal

Scatterplot of the Pelvic Organ Prolapse Quantification (POP-Q) and magnetic resonance imaging-Pelvic Inclination Correction system (MRI-PICS) measurements of the bladder plotted individually per patient. The red datapoints show the MRI-PICS measurements per patient and are connected by the dotted line to the corresponding blue datapoints representing the POP-Q measurements. All patients are sorted by measurement difference
Uterus
Figure 4 shows a scatterplot of the POP-Q and MRI-PICS measurements of the uterus, indicating the variety of MRI-PICS measures per POP-Q outcome. For instance, when considering the uterus at POP-Q measurement −4, a large variation in MRI-PICS measurements was found, with differences up to 5.5 cm between patients. Figure 5 illustrates the discrepancy between POP-Q and MRI-PICS measurements per patient, identifying three groups: patients in whom the MRI-PICS measurement is smaller (difference < −0.5 cm) than the POP-Q measurement (n = 6 [9.5%]); patients in whom the measurements were almost identical (absolute difference < 0.5 cm (n = 12 [19.0%]); and patients in whom the MRI-PICS measurement was larger (difference > 0.5 cm) than the POP-Q measurement (n = 45 [71.4%]). Of the patients with a stage 1 uterus prolapse specifically, 92% show greater descent of the uterus of 3.6 ± 2.2 cm on MRI-PICS compared with POP-Q. The measurement differences between the POP-Q and the MRI-PICS of the uterus vary from −2.1 cm to 8.5 cm.

Scatterplot of the Pelvic Organ Prolapse Quantification (POP-Q) and magnetic resonance imaging-Pelvic Inclination Correction system (MRI-PICS) measurements of the uterus. POP-Q (x-axis) and MRI-PICS (y-axis) measurements of the uterus showing that MRI-PICS measurements are often larger. Data points are color labeled by POP-Q stage. The green line represents the reference line at which POP-Q and MRI-PICS values are equal

Scatterplot of the Pelvic Organ Prolapse Quantification (POP-Q) and magnetic resonance imaging-Pelvic Inclination Correction system (MRI-PICS) measurements of the uterus plotted individually per patient. The red datapoints show the MRI-PICS measurements per patient and are connected by the dotted line to the corresponding blue datapoints representing the POP-Q measurements. All patients are sorted by measurement difference
Discussion
Main Findings
This prospective study showed a significant moderate positive correlation between the POP-Q and MRI-PICS measurements for the bladder and uterus in patients with POP. Furthermore, MRI-PICS measurements varied widely in patients with the same POP-Q values, and in 71.4% of the bladder and uterus measurements, the MRI-PICS measurements showed greater organ descent than the POP-Q measurements.
Strengths and Limitations
The most important strength of this study is the use of upright instead of supine MRI. The upright rest position gives the best reflection of the natural organ position in patients with POP during the day. Another strong point in our study is that all the MRI-PICS measurements were performed in 3D, by one observer, following a dedicated protocol, reducing possible observer variation [20, 21].
Our study has several limitations. The widely varying MRI-PICS measurements for patients with the same POP-Q measurement could be explained by inaccuracies in the POP-Q measurements. As is known from literature, under controlled circumstances POP-Q has a high interobserver correlation [23]. However, in general clinical practice, as in our hospital, there is great variation in the execution of the POP-Q measurements. For example, not all patients are able to perform the Valsalva maneuver properly, specula are not used by all gynecologists, nor are rulers. This variation may have influenced our study results; however this effect, if at all present, would be minor and the variation reflects clinical practice [11, 24, 25]. As was mentioned earlier, we do not suspect the MRI-PICS measurements to be inaccurate, owing to the protocol that was performed.
Second, making a direct comparison between POP-Q and MRI-PICS is difficult because the hymen, which is the reference point for the POP-Q, was not visible on the MRI scans. We hypothesize that the position of the PICS plane might be more cranial than the hymen, which can account for the greater extent of POP measured with MRI-PICS than with POP-Q in the majority of the patients. However, the hymen as a reference point is not as fixed as the PICS plane and therefore comparing absolute values between POP-Q and MRI-PICS is not useful. Besides, this would not have influenced the currently found moderate positive correlation and cannot explain the large variety of measurements for the same POP-Q value.
Interpretation
To the best of our knowledge, our study is the first to quantify the difference in the extent of prolapse between POP-Q and upright MRI measurements. The underestimation of POP by POP-Q compared with MRI-PICS can be explained by several arguments. Most important is the patient position during the examination. The POP-Q measurements are performed in a dorsal lithotomy position during Valsalva maneuver, whereas the MRI-PICS measurements are performed in an upright position with the pelvis at rest. Previous studies already concluded that the supine straining position can lead to an underestimation of POP, as not all patients are able to perform Valsalva correctly [18]. The underestimation of uterus prolapse we determined is in line with earlier research that compared POP-Q measurement with Valsalva with POP-Q measurement under traction intra-operatively. An increase in uterus prolapse in up to 93% of patients was found in these studies [8,9,10].
The implications of this study for the individual patient are of utmost importance because underestimation of the degree of POP can lead to under-treatment. For instance, if a patient suffers from POP symptoms, but no prolapse is seen on physical examination, no treatment is recommended, and the patient continues to suffer the same complaints. Additionally, in planning POP surgery, underestimation of POP can lead to choosing the wrong or incomplete technique for correcting POP. This may lead to early recurrence of POP and the need to perform recurrence surgery. Considering this, ideally, we recommend performing upright MRI-PICS measurements in all patients with POP for whom the symptoms are worse than expected based on the extent of POP seen on physical examination.
Apart from the correlation between MRI-PICS measurements and POP-Q measurements, future research should focus on the correlation between MRI-PICS measurements and symptoms. Previous research showed that symptoms correlate poorly with POP-Q stage, which might now be explained by the underestimation of POP. In that case MRI-PICS measurements could show a better correlation with complaints.
Conclusion
In this prospective study we showed that despite a moderate positive correlation between the POP-Q measurements and the upright MRI-PICS measurements in patients with POP, an underestimation of POP when assessed using POP-Q is found. The great variation in MRI-PICS measurement in patients with similar POP-Q values supports our hypothesis that upright MRI might give a more reliable estimation of the extent of prolapse of the bladder and uterus. We recommend further research to consider the correlation between POP symptoms and MRI-PICS measurements, to conclude whether upright MRI is of value for patients in whom symptoms are worse than expected based on POP-Q.
References
Slieker-ten Hove MCP, Pool-Goudzwaard AL, Eijkemans MJC, et al. Symptomatic pelvic organ prolapse and possible risk factors in a general population. Am J Obstet Gynecol. 2009;200:184.e1–7. https://doi.org/10.1016/j.ajog.2008.08.070.
Haylen BT, De Ridder D, Freeman RM, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Int Urogynecol J. 2010;21:5–26. https://doi.org/10.1007/s00192-009-0976-9.
Bø K, Anglès-Acedo S, Batra A, et al. International urogynecology consultation chapter 3 committee 2; conservative treatment of patient with pelvic organ prolapse: pelvic floor muscle training. Int Urogynecol J. 2022;33:2633–67. https://doi.org/10.1007/S00192-022-05324-0.
Bump RC, Mattiasson A, Brubaker LP, et al. The standardization of terminology of female pelvic organ prolapse and pelvic floor dysfunction. Am J Obstet Gynecol. 1996;175:10–7.
Haylen BT, Maher CF, Barber MD, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic organ prolapse (POP). Int Urogynecol J. 2016;27:165–94. https://doi.org/10.1007/s00192-015-2932-1.
Pelvic Organ Prolapse: ACOG Practice Bulletin, Number 214. Obstet Gynecol 2019;134:e126–42. https://doi.org/10.1097/AOG.0000000000003519
Urinary incontinence and pelvic organ prolapse in women: management. NICE guideline. 2019.
Chao FL, Rosamilia A, Dwyer PL, et al. Does pre-operative traction on the cervix approximate intra-operative uterine prolapse? A randomised controlled trial. Int Urogynecol J. 2012;23:417–22. https://doi.org/10.1007/S00192-011-1656-0.
Krissi H, Eitan R, Ram E, Peled Y. How accurate is preoperative evaluation of pelvic organ prolapse in women undergoing vaginal reconstruction surgery? PLoS One 2012;7:e47027. https://doi.org/10.1371/JOURNAL.PONE.0047027
Chaudhuri S, Vaitheeswari J. Correlation of preoperative and intraoperative assessment of pelvic organ prolapse by pelvic organ prolapse quantification system. Int J Gynecol Obstet. 2022;157:466–70. https://doi.org/10.1002/IJGO.13894.
Visco AG, Wei JT, McClure LA, et al. Effects of examination technique modifications on pelvic organ prolapse quantification (POP-Q) results. Int Urogynecol J. 2003;14:136–40. https://doi.org/10.1007/s00192-002-1030-3.
Manonai J, Wattanayingcharoenchai R. Relationship between pelvic floor symptoms and POP-Q measurements. Neurourol Urodyn. 2016;35:724–7. https://doi.org/10.1002/nau.22786.
Ellerkmann RM, Cundiff GW, Melick CF, et al. Correlation of symptoms with location and severity of pelvic organ prolapse. Am J Obstet Gynecol. 2001;185:1332–8. https://doi.org/10.1067/MOB.2001.119078.
Law YM, Fielding JR. MRI of pelvic floor dysfunction: review. Am J Roentgenol 2008;191:S45–53.
Fauconnier A, Zareski E, Abichedid J, et al. Dynamic magnetic resonance imaging for grading pelvic organ prolapse according to the International Continence Society classification: which line should be used? Neurourol Urodyn. 2008;27:191–7. https://doi.org/10.1002/nau.20491.
Broekhuis SR, Kluivers KB, Hendriks JCM, et al. POP-Q, dynamic MR imaging, and perineal ultrasonography: do they agree in the quantification of female pelvic organ prolapse?. 2009;20:541-9. https://doi.org/10.1007/s00192-009-0821-1
Lakeman MME, Zijta FM, Peringa J, et al. Dynamic magnetic resonance imaging to quantify pelvic organ prolapse: reliability of assessment and correlation with clinical findings and pelvic floor symptoms. Int Urogynecol J. 2012;23:1547–54. https://doi.org/10.1007/S00192-012-1772-5.
Grob ATM, Olde Heuvel J, Futterer JJ, et al. Underestimation of pelvic organ prolapse in the supine straining position, based on magnetic resonance imaging findings. Int Urogynecol J. 2019;30:1939–44. https://doi.org/10.1007/s00192-018-03862-0.
Betschart C, Chen L, Ashton-Miller JA, DeLancey JOL. On pelvic reference lines and the MR evaluation of genital prolapse: a proposal for standardization using the pelvic inclination correction system. Int Urogynecol J. 2013;24:1421–8. https://doi.org/10.1007/S00192-013-2100-4.
Reiner CS, Williamson T, Winklehner T, et al. The 3D Pelvic Inclination Correction System (PICS): a universally applicable coordinate system for isovolumetric imaging measurements, tested in women with pelvic organ prolapse (POP). Comput Med Imaging Graph. 2017;59:28–37. https://doi.org/10.1016/j.compmedimag.2017.05.005.
Morsinkhof LM, Schulten MK, DeLancey JOL, et al. Pelvic inclination correction system for magnetic resonance imaging analysis of pelvic organ prolapse in upright position. Int Urogynecol J. 2022;33:2801–7. https://doi.org/10.1007/s00192-022-05289-0.
Virzì A, Muller CO, Marret JB, et al. Comprehensive review of 3D segmentation software tools for MRI usable for pelvic surgery planning. J Digit Imaging. 2020;33:99–110. https://doi.org/10.1007/S10278-019-00239-7.
Hall AF, Theofrastous JP, Cundiff GW, et al. Interobserver and intraobserver reliability of the proposed International Continence Society, Society of Gynecologic Surgeons, and American Urogynecologic Society pelvic organ prolapse classification system. Am J Obstet Gynecol. 1996;175:1467–71. https://doi.org/10.1016/S0002-9378(96)70091-1.
Pham T, Burgart A, Kenton K, et al. Current use of pelvic organ prolapse quantification by AUGS and ICS members. Female Pelvic Med Reconstr Surg. 2011;17:67–9. https://doi.org/10.1097/SPV.0B013E318207C904.
Madhu C, Swift S, Moloney-Geany S, Drake MJ. How to use the Pelvic Organ Prolapse Quantification (POP-Q) system? Neurourol Urodyn. 2018;37:S39–43. https://doi.org/10.1002/NAU.23740.
Acknowledgements
This study was partly funded by a research grant from the Ziekenhuisgroep Twente Hospital. The Ziekenhuisgroep Twente was not involved in the designing and conducting of the research, or in the writing of the manuscript.
Author information
Authors and Affiliations
Contributions
A.v.d.S.: data analysis, manuscript writing; K.Y.J.: data analysis, manuscript editing; E.C.J.C.: project development, manuscript editing; F.F.J.S.: project development, data analysis, manuscript editing; A.T.M.G.: project development, data collection, data analysis, manuscript editing.
Corresponding author
Ethics declarations
Ethical Approval
Both studies were approved by the medical ethics committee CMO region Arnhem-Nijmegen and registered as NL74061.091.20 and NL79717.091.21.
Conflicts of Interest
None.
Additional information
Handling Editor: Jaromir Masata
Editor in Chief: Maria A. Bortolini
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
van der Steen, A., Jochem, K.Y., Consten, E.C.J. et al. POP-Q Versus Upright MRI Distance Measurements: A Prospective Study in Patients with POP. Int Urogynecol J 35, 1255–1261 (2024). https://doi.org/10.1007/s00192-024-05802-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-024-05802-7