
Abstract
Introduction and hypothesis
We aimed to compare differences between laparoscopic lateral suspension with mesh (LLS) performed with supracervical hysterectomy (LLSHE) and without hysterectomy (LLSUP).
Methods
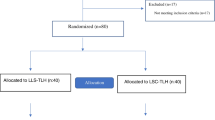
We retrospectively collected data from women operated by a single surgeon between 2003 and 2011. From a total of 339 women with symptomatic anterior and/or apical pelvic organ prolapse (POP) and an intact uterus, 224 had LLSUP (70.4%) and 94 had LLSHE (29.6%). Three hundred and sixteen patients were examined at 1 year. Primary outcomes were objective and subjective success at 1 year during clinical evaluation. Secondary outcomes were complications (Clavien-Dindo scale) and mesh exposure. Patient satisfaction was evaluated by telephone interview using a 10-point scale and the Patient Global Impression of Improvement Scale (PGI-I).
Results
LLSUP and LLSHE did not differ for age (mean 57 and 55 years, respectively), preoperative status, complications, and participation at the interview (52 vs 53%). LLSHE is associated with higher mesh exposure (6.5 vs 1.3%, p = 0.014) and more frequent use of Mersilene. Titanium-coated and noncoated polypropylene was more frequently used in LLSUP. At 1 year, both anatomic success rate for the anterior compartment (98.7 vs 94.6%, p = 0.021) and subjective success rate (83.5 vs 72.8%, p = 0.035) were higher for LLSUP. Without hysterectomy, patients more often improved (90.5 vs 76.5%, p = 0.013) and would more frequently recommend the procedure (94.5 vs 80.4%, p = 0.004).
Conclusions
LLS with or without hysterectomy is a safe technique with high patient satisfaction. The uterus-preserving approach appears to result in better anatomic outcome for the anterior compartment, better subjective outcome, and higher patient satisfaction.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The high prevalence of pelvic organ prolapse (POP) is closely associated with the high risk for woman to undergo surgery for such a condition [1,2,3,4]. There is an ongoing debate about the ideal surgical approach for POP in general and the apical compartment in particular [5]. Traditionally, in the presence of a uterus, surgical correction of apical prolapse has included hysterectomy, whereas now, it is believed that the uterus plays more of a passive role in the condition’s development [6]. Although POP has a significant impact on a woman’s quality of life (QoL), a radical surgical approach sacrificing an otherwise healthy organ is frequently questioned [1, 7]. For some women, the uterus is part of their sense of identity, and they would opt for uterine preservation for additional reasons, such as the desire to maintain fertility and the belief it affects sexual function [6]. This change in psychological value has led to an increase in uterine-sparing prolapse surgery [7,8,9]. Laparoscopic sacrocolpopexy and sacrohysteropexy are now considered the gold standards for correcting apical POP [5]. These techniques require dissection at the level of the promontory, which can be challenging, particularly in obese women and when anatomic variations exist. Sacral area lesions can lead to serious neurological, ureteral, or vascular injuries. In up to 50% of patients, lumbar pain has been described following mesh fixation at the sacrum [10]. In our previous publications, we demonstrated that laparoscopic lateral suspension (LLS) with mesh is a safe and feasible alternative. It avoids dissection at the promontory and can be performed with uterine preservation [11, 12]. We also previously identified uterus-preserving LLS as a factor improving patient satisfaction [13]. In the cross-sectional study reported here, we compared outcomes, complications, and prolapse-associated symptoms in women from the same cohort operated with LLS performed with and without hysterectomy.
Materials and methods
The local Ethics Committee on Clinical Studies of the Geneva University Hospitals approved the study protocol (no. 14-197). This observational cross-sectional study represents a prospective series of consecutive patients treated by LLS for symptomatic POP between January 2004 and October 2011 by a single surgeon (JBD) at the Geneva University Hospital and who completed a standardized clinical follow-up assessment of patients at 1 year postsurgery. We followed recommendations of the International Urogynecology Association (IUGA) for reporting outcome of surgical procedures for POP [14].
Preoperative assessment and inclusion criteria
Patients were included for surgical treatment with LLS when they presented with prolapse-related symptoms, such as a sensation of a bulge or a lump in the vagina. Patients were offered a supracervical hysterectomy if they desired removal of the uterus in the presence of uterine abnormalities, such as enlarged leiomyomas, adenomyosis, endometrial hyperplasia, or abnormal uterine bleeding. All other women had a uterus-preserving approach. Clinical evaluation of pelvic organ support was assessed by the simplified Pelvic Organ Prolapse Quantification grading system (POP-Q) [15]. When patients presented with clinically reported stress urinary incontinence (SUI), they were offered concomitant surgical treatment by laparoscopic Burch colposuspension or transobturator suburethral tape or expectative management.
Surgical technique
LLS aims to treat anterior and apical compartment POP. It is performed under general anesthesia with the patient in the Trendelenburg position. We use a central 10-mm umbilical trocar for the camera and three working trocars (all 5 mm or one 10 mm and one 2 5 mm) in the inguinal regions and suprapubically. In a first step, the vesicovaginal space is dissected until the endopelvic fascia is reached. This deep dissection adequately enables the treatment of concomitant cystocele. In a second step, the rectovaginal space is dissected toward the perineal and anorectal junction. For both steps, the dissection plane is exposed with the help of a flat-blade retractor placed in the vagina and manipulated by the assistant. Third, the mesh is introduced in the peritoneal cavity through a 10-mm trocar. The mesh is T-shaped and has a central rectangular part (~4 × 6 cm) and two long lateral side arms. The central part is flattened over the vesicovaginal dissection plane and fixed to the vaginal fascia with absorbable tackers and four to six separated nonabsorbable sutures. In a fourth step, the skin is incised 2 cm above the iliac crest and 4 cm posterior to the anterior superior iliac spine on both sides over 3 mm, and a laparoscopic grasping forceps is introduced through this new incision (Fig. 1). The latter perforates the aponeurosis perpendicularly and stops behind the peritoneum without perforating it. The forceps is pushed toward the round ligament at the level of its lateral peritoneal insertion through retroperitoneal tunnelization under transperitoneal visualization. The side arms of the mesh previously fixed at the vesicovaginal space can now be grasped and pulled backward through the previously formed tunnel with the tension symmetrically adjusted. Retroperitoneal fibrosis provides adequate attachment of the mesh, with lateral tension-free suspension of the central mesh part attached to the vagina. Hysterocele and cystocele are hereby treated. The peritoneum is closed to completely cover the graft and the side arms cut at the level of the skin (Fig. 2). The posterior compartment was treated separately when there was a prolapse beyond the hymen or preoperative constipation. We either placed a posterior polypropylene mesh laparoscopically in the rectovaginal space after deep dissection, or we performed a posterior colporrhaphy though the vaginal route.
The first patients operated in our series had placement of polyethylene meshes (Mersilene®; Ethicon Inc., Somerville, NJ, USA); recently, only macroporous lightweight polypropylene meshes (Gynemesh®; Ethicon) or titanium-coated polypropylene meshes (TiLOOP®; pfm medical ag, Köln, Germany) have been used. Polyethylene was withdrawn from the market during our study because of an increasing number of reports by other surgeons of mesh erosion.
Postoperative assessment
Systematic postoperative clinical examination and assessment of lower urinary tract symptoms (LUTS), satisfaction, and prolapse-related symptoms was performed at 12 months. Additionally, we searched hospital files for mesh-related complications.
Outcome measures
The main outcome measures were subjective and objective cure at 1 year and patient satisfaction at a certain point in time since the operation. Anatomic cure was the first primary outcome and defined as POP-Q sites Ba, C, and Bp less than −1 cm [16]. Subjective cure was the second primary outcome and was considered when the patient did not report any prolapse-related symptoms. Patient satisfaction was the third primary outcome and was assessed using the Patient Global Impression of Improvement (PGI-I) and a 10-point visual analog scale (VAS) for global satisfaction during a telephone interview. Highest possible satisfaction was rated 10 and lowest 0. The interview was conducted between 4 and 10 years after surgery [17]. Patients were considered satisfied when they rated satisfaction with at least 8 and when the PGI-I was answered as “improved” or “very improved.” Secondary outcomes were mesh-related complications. We also reported complication rates using the Clavien-Dindo scale [18].
Statistical analyses
Continuous variables were reported by their mean ± standard deviation (SD). We considered a p value of <0.05 to reflect statistical significance. Categorical variables were described by their number and relative proportion. Variables were compared between groups using the chi-square test. We then assessed whether there was a change in prolapse stages pre- and postoperatively in the same patients (POP-Q point Ba, C, and Bp above −1 cm) using McNemar test. Data analysis was performed using SPSS version 24.0.
Results
Between 2003 and 2011, 243 patients had uterus-preserving laparoscopic lateral suspension (LLSUP), and 96 patients had laparoscopic lateral suspension after supracervical hysterectomy (LLSHE), with the uterus being removed after intra-abdominal morcellation. Demographic data, preoperative procedures, and conditions are summarized in Table 1 and postoperative conditions in Table 2. Preoperative characteristics did not differ between groups, except for body mass index (BMI) (LLSUP 26.05 ± 4.04 vs LLSHE 27.05 ± 3.73, p = .036). All patients had significant stage ≥2 POP in at least two of the three compartments (Table 3). Several patients had concomitant surgery for SUI: 144 of 153 SUI patients in the LLSUP group and 46 of 55 in the LLSHE group. There was no difference between groups in regard to technique used for the procedure (Table 3). The postoperative persistent SUI rate was similar between groups, while the de novo SUI rate was significantly higher in the LLSHE group (4.3 vs 1.8%, p = .030) (Table 3).
The operating time was significantly longer in the LLSHE group in whom a hysterectomy was performed compared with the LLSUP group in whom the uterus was preserved (mean operating time in minutes 237.13 (± 57.56) vs 189.26 (± 44.62), p < 0.001). Groups differed significantly in regard to type of mesh material used. More patients in the LLSHE group were treated with a polyethylene mesh than patients in the LLSUP group (64.6% vs 30%).
There was no conversion to laparotomy. Seven patients had major complications rated grade 3 on the Clavien-Dindo scale (Table 3): three in the LLSUP group vs four in the LLSHE group. In the LLSUP group, two patients had a trocar hernia at the level of a 10-mm trocar insertion (usually the left groin area) and one a vaginal hematoma after posterior colporrhaphy, which was surgically drained. In the LLSHE group, two vesical lesions were immediately sutured: one patient had trocar-related subcutaneous granuloma and one required re-implantation of the ureter on day 16 postoperatively after discovery of a ureterovaginal fistula.
POP symptoms were reported by 16.5% of women in the LLSUP and 27.2% in the LLSHE group 1 year after surgery, indicating a significantly different subjective cure rate of 83.5 vs 72.8% (p = 0.030) (Table 3). Overall, there were more sexually active women at 1 year after surgery (LLSUP 82.8%; LLSHE 86.3%) (Table 3) than preoperatively (LLSUP 60.8%; LLSHE 70%) (Table 1). Twenty-three patients were lost to clinical follow-up after 1 year, 20 in the LLSUP group and three in the LLSHE group. There was clinically and statistically significant anatomic improvement for all compartments at 1 year postoperatively in both groups, resulting in an objective cure rate of 98.7 and 94.6% for the anterior, 97.3 and 95.7% for the apical, and 95.1 and 95.7% for the posterior compartments, respectively (Table 2). There was a significantly better improvement rate for the anterior compartment in the LLSUP group (p = 0.035) (Table 2). Women in the LLSHE group had significantly higher persistent (12.0 vs 3.1%, p = .004) and de novo (4.3 vs 2.2%, p = .008) constipation rates compared with women in the LLSUP group (Table 3).
Nine patients had mesh-related complications: three (1.3%) in the LLSUP group compared with a significantly higher number of six (6.5%, p = 0.012) in the LLSHE group. In the LLSUP group, two (0.9%) patients had exposure or extrusion of the anterior and one patient (0.4%) of the posterior mesh. In the LLSHE group, five (0.9%) patients had exposure or extrusion of the anterior and two patients (2.2%) of the posterior mesh. The mesh-related complication rate for the anterior graft was significantly higher in the LLSHE group (p = 0.013) (Table 3).
One hundered and twenty-seven patients with LLSUP (52.3%) and 51 with LLSHE (53.1%) participated in the telephone interview. The mean follow-up period was significantly shorter in the LLSHE group (22.61 vs 24.91 months, p < 0.001). One hundred and fifty-one women were not reachable after at least three attempts, and five refused to participate. Five women died during the study period. Significantly more patients in the LLSUP group reported a VAS score of ≥8 (85.8%) compared with those in the LLSHE group (66.7%) (p = 0.004). Improvement (improved or very much improved) in their condition was reported by 90.6% of women in the LLSUP group (on the PGI-I scale, which was significantly more frequent than women in the LLSHE group (76.5%) (p = 0.013). Those in the LLSUP group would recommend the operation more often than those in the LLSHE group (94.5 vs 80.4%, respectively, p = 0.004). Results of the telephone interview are summarized in Table 4.
Discussion
Between 31 and 60% of US women presenting for prolapse care would elect to keep their uterus if surgical outcomes were equally efficacious [19]. One reason might be the knowledge among patients about higher exposure rates after mesh augmented prolapse repair when hysterectomy is performed. However, at the time of our study, debates about mesh surgery were still quite uncommon in the broader public perception.
Uterine preservation is a suitable option in women with POP; however, long-term data are limited, and the need for subsequent hysterectomy is unknown [6, 20]. Our large series demonstrated that the technique of LLS performed with or without hysterectomy is feasible and effective in an overweight population, with low postoperative complications within 1 year. Patients in our study shared comparable characteristics and perioperative outcomes with those in large series on sacrocolpopexy and sacral hysteropexy [21,22,23,24]. Both our techniques for POP surgery—uterine preserving and not preserving—demonstrated overall objective success rates >90% at 1 year. Similar results have been reported for sacrocolpopexy and sacral hysteropexy in previous studies [5, 6]. In addition to previous results from our series, we directly compared hysterectomy and uterine-preservation approaches. We present new findings that add further substantial information for the benefit of patients in the context of a growing demand in uterine-preserving strategies for treating prolapse. We can only speculate about the reason for the surprising finding of a better outcome for the anterior compartment in the LLSUP group. Maybe isthmic fixation of the mesh provides better anterior traction on the vaginal wall. The subjective cure rate at 1 year was high in the LLSHE group and even higher in the LLSUP group. Overall, our results showed a positive outcome by definition of the composite criteria described by Barber et al. [16].
Only 2.2% of patients in the LLSUP group and 4.3% in the LLSHE group developed de novo constipation: this is less than the published rates for sacropexy [21,22,23]. Lesions of the superior hypogastric plexus and spondylodiscitis are known complications of sacral fixation, and numerous cases have been described in the literature [25]. The advantage of our technique is it avoids dissection at the level of the promontory and associated risks, which are commonly described in obese women in particular. The higher de novo constipation rate in the LLSHE group may be explained by potential lesions close to the hypogastric nerves during hysterectomy, with crossing fibers coming from the superior hypogastric plexus and going to the pelvic side wall, which are at risk for damage. LLS resulted in low rates of LUTS and seems to preserve normal sexual function, with higher rates of sexually active patients after the surgery than before in both groups at 1 year postoperatively.
Perioperative complications of Clavien-Dindo grade ≥3 occurred as rarely in both cohorts as in reports that used different techniques [26]. Mesh-related complication rates were comparable with those reported for other laparoscopic prosthetic POP repairs [26]. The current reports indicate that sacral colpopexy associated with hysterectomy has a four times higher risk of mesh exposure (grade B) than sacral colpopexy without hysterectomy [6, 27]. The higher rate in our hysterectomy group is probably due to the more frequent use of polyethylene mesh, which has been withdrawn from the market for this precise reason. The difference in type of mesh material used in both groups represents a significant bias in our study. However, we found no exposure with titanium-coated polypropylene, the benefits of which were demonstrated in hernia repair [28, 29].
Our telephone interview revealed a higher satisfaction in patients who had LLS with uterine preservation. These results may be biased by the difference in mean follow-up period between groups, although overall mean follow-up exceeded 6.5 years in both groups. The higher subjective cure rate and satisfaction in LLSHE patients may illustrate the trend of a positive association women tend to have between their self-image and their uterus.
The strengths of this study are its prospective design with regard to the clinical follow-up as a consecutive series of patients operated with a standardized technique by a single surgeon and the satisfying turnout of >50% in telephone interviews, providing a long-term follow-up about patient satisfaction. However, loss to follow-up rates close to 50% may represent a source for bias. Loss to follow-up was partially due to a highly migratory patient population. Limitations were results based on the experience a single surgeon working in single university center and the substantial differences in mesh materials used over the years. Patient satisfaction was assessed on a long-term basis using objective factors measured at standardized time-points following surgery, but there were significant variations in postoperative follow-up times when this information was obtained. Another shortcoming is the heterogeneity in follow-up intervals for objective and subjective outcome (1 year) and patient satisfaction (4–10 years).
Conclusion
In conclusion, both LLSUP and LLSHE are feasible and safe approaches for POP in sexually active and obese women and may represent a safe alternative to sacrohysteropexy and sacrocolpopexy, respectively. Uterine preservation is associated with higher satisfaction rates, better short-term subjective outcome, and lower rates of postoperative constipation and de novo SUI. However, there were differences in mesh materials used, and only a prospective controlled randomized study may confirm our results. Overall, patient goals and preferences about preservation of the uterus should be carefully considered during surgical planning and when obtaining informed consent. There is a need for further studies evaluating the safety and efficacy of hysteropexy, since there are limited data regarding risks associated with subsequent pregnancy and delivery.
Abbreviations
- POP:
-
Pelvic organ prolapse
- LLS:
-
Laparoscopic lateral suspension
- LLSUP:
-
Uterus-preserving laparoscopic lateral suspension
- LLSHE:
-
Laparoscopic lateral suspension with hysterectomy
- POP-Q:
-
Pelvic Organ Prolapse Quantification system
- PGI-I:
-
Patient Global Impression of Improvement
- VAS:
-
Visual analog scale
- LUTS:
-
Lower urinary tract symptoms
References
Barber MD, Maher C. Epidemiology and outcome assessment of pelvic organ prolapse. Int Urogynecol J. 2013;24(11):1783–90. https://doi.org/10.1007/s00192-013-2169-9.
Nygaard I, Barber MD, Burgio KL, Kenton K, Meikle S, Schaffer J, et al. Prevalence of symptomatic pelvic floor disorders in US women. JAMA. 2008;300(11):1311–6. https://doi.org/10.1001/jama.300.11.1311.
Handa VL, Garrett E, Hendrix S, Gold E, Robbins J. Progression and remission of pelvic organ prolapse: a longitudinal study of menopausal women. Am J Obstet Gynecol. 2004;190(1):27–32. https://doi.org/10.1016/j.ajog.2003.07.017.
Smith FJ, Holman CD, Moorin RE, Tsokos N. Lifetime risk of undergoing surgery for pelvic organ prolapse. Obstet Gynecol. 2010;116(5):1096–100. https://doi.org/10.1097/AOG.0b013e3181f73729.
Barber MD, Maher C. Apical prolapse. Int Urogynecol J. 2013;24(11):1815–33. https://doi.org/10.1007/s00192-013-2172-1.
Gutman R, Maher C. Uterine-preserving POP surgery. Int Urogynecol J. 2013;24(11):1803–13. https://doi.org/10.1007/s00192-013-2171-2.
Rosen DM, Shukla A, Cario GM, Carlton MA, Chou D. Is hysterectomy necessary for laparoscopic pelvic floor repair? A prospective study. J Minim Invasive Gynecol. 2008;15(6):729–34. https://doi.org/10.1016/j.jmig.2008.08.010.
Frick AC, Barber MD, Paraiso MF, Ridgeway B, Jelovsek JE, Walters MD. Attitudes toward hysterectomy in women undergoing evaluation for uterovaginal prolapse. Female Pelvic Med Reconstr Surg. 2013;19(2):103–9. https://doi.org/10.1097/SPV.0b013e31827d8667.
Korbly NB, Kassis NC, Good MM, Richardson ML, Book NM, Yip S, et al. Patient preferences for uterine preservation and hysterectomy in women with pelvic organ prolapse. Am J Obstet Gynecol. 2013;209(5):470.e471–6. https://doi.org/10.1016/j.ajog.2013.08.003.
Vieillefosse S, Thubert T, Dache A, Hermieu JF, Deffieux X. Satisfaction, quality of life and lumbar pain following laparoscopic sacrocolpopexy: suture vs. tackers. Eur J Obstet Gynecol Reprod Biol. 2015;187:51–6. https://doi.org/10.1016/j.ejogrb.2015.02.014.
Dubuisson JB, Yaron M, Wenger JM, Jacob S. Treatment of genital prolapse by laparoscopic lateral suspension using mesh: a series of 73 patients. J Minim Invasive Gynecol. 2008;15(1):49–55. https://doi.org/10.1016/j.jmig.2007.11.003.
Veit-Rubin N, Dubuisson JB, Lange S, Eperon I, Dubuisson J. Uterus-preserving laparoscopic lateral suspension with mesh for pelvic organ prolapse: a patient-centred outcome report and video of a continuous series of 245 patients. Int Urogynecol J. 2016;27(3):491–3. https://doi.org/10.1007/s00192-015-2859-6.
Veit-Rubin N, Dubuisson JB, Gayet-Ageron A, Lange S, Eperon I, Dubuisson J. Patient satisfaction after laparoscopic lateral suspension with mesh for pelvic organ prolapse: outcome report of a continuous series of 417 patients. Int Urogynecol J. 2017;28(11):1685–93. https://doi.org/10.1007/s00192-017-3327-2.
Toozs-Hobson P, Freeman R, Barber M, Maher C, Haylen B, Athanasiou S, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for reporting outcomes of surgical procedures for pelvic organ prolapse. Int Urogynecol J. 2012;23(5):527–35. https://doi.org/10.1007/s00192-012-1726-y.
Swift S, Morris S, McKinnie V, Freeman R, Petri E, Scotti RJ, et al. Validation of a simplified technique for using the POPQ pelvic organ prolapse classification system. Int Urogynecol J Pelvic Floor Dysfunct. 2006;17(6):615–20. https://doi.org/10.1007/s00192-006-0076-z.
Barber MD, Brubaker L, Nygaard I, Wheeler TL 2nd, Schaffer J, Chen Z, et al. Defining success after surgery for pelvic organ prolapse. Obstet Gynecol. 2009;114(3):600–9. https://doi.org/10.1097/AOG.0b013e3181b2b1ae.
Srikrishna S, Robinson D, Cardozo L. Validation of the patient global impression of improvement (PGI-I) for urogenital prolapse. Int Urogynecol J. 2010;21(5):523–8. https://doi.org/10.1007/s00192-009-1069-5.
Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250(2):187–96. https://doi.org/10.1097/SLA.0b013e3181b13ca2.
Gutman RE. Does the uterus need to be removed to correct uterovaginal prolapse? Curr Opin Obstet Gynecol. 2016;28(5):435–40. https://doi.org/10.1097/GCO.0000000000000307.
Medina C, Takacs P. Laparoscopic uterosacral uterine suspension: a minimally invasive technique for treating pelvic organ prolapse. J Minim Invasive Gynecol. 2006;13(5):472–5. https://doi.org/10.1016/j.jmig.2006.04.009.
Rozet F, Mandron E, Arroyo C, Andrews H, Cathelineau X, Mombet A, et al. Laparoscopic sacral colpopexy approach for genito-urinary prolapse: experience with 363 cases. Eur Urol. 2005;47(2):230–6. https://doi.org/10.1016/j.eururo.2004.08.014.
Rivoire C, Botchorishvili R, Canis M, Jardon K, Rabischong B, Wattiez A, et al. Complete laparoscopic treatment of genital prolapse with meshes including vaginal promontofixation and anterior repair: a series of 138 patients. J Minim Invasive Gynecol. 2007;14(6):712–8. https://doi.org/10.1016/j.jmig.2007.06.017.
Claerhout F, De Ridder D, Roovers JP, Rommens H, Spelzini F, Vandenbroucke V, et al. Medium-term anatomic and functional results of laparoscopic sacrocolpopexy beyond the learning curve. Eur Urol. 2009;55(6):1459–67. https://doi.org/10.1016/j.eururo.2008.12.008.
Krause HG, Goh JT, Sloane K, Higgs P, Carey MP. Laparoscopic sacral suture hysteropexy for uterine prolapse. Int Urogynecol J Pelvic Floor Dysfunct. 2006;17(4):378–81. https://doi.org/10.1007/s00192-005-0019-0.
Propst K, Tunitsky-Bitton E, Schimpf MO, Ridgeway B. Pyogenic spondylodiscitis associated with sacral colpopexy and rectopexy: report of two cases and evaluation of the literature. Int Urogynecol J. 2014;25(1):21–31. https://doi.org/10.1007/s00192-013-2138-3.
Maher C, Feiner B, Baessler K, Schmid C. Surgical management of pelvic organ prolapse in women. Cochrane Database Syst Rev. 2013;4:CD004014. https://doi.org/10.1002/14651858.CD004014.pub5.
Stepanian AA, Miklos JR, Moore RD, Mattox TF. Risk of mesh extrusion and other mesh-related complications after laparoscopic sacral colpopexy with or without concurrent laparoscopic-assisted vaginal hysterectomy: experience of 402 patients. J Minim Invasive Gynecol. 2008;15(2):188–96. https://doi.org/10.1016/j.jmig.2007.11.006.
Le TH, Kon L, Bhatia NN, Ostergard DR. Update on the utilization of grafts in pelvic reconstruction surgeries. Curr Opin Obstet Gynecol. 2007;19(5):480–9. https://doi.org/10.1097/GCO.0b013e3282efdecd.
Kockerling F, Schug-Pass C. What do we know about titanized polypropylene meshes? An evidence-based review of the literature. Hernia. 2014;18(4):445–57. https://doi.org/10.1007/s10029-013-1187-3.
Acknowledgements
Open access funding provided by Medical University of Vienna.
Funding
Pfm medical ag, Köln, Germany, contributed to the costs for statistical analysis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
Jean-Bernard Dubuisson is a medical advisor for pfm medical ag, Köln, Germany.
All other authors declare that they have no conflict of interest.
Additional information
Prior presentations
• The results of this study were presented as an oral poster communication at the 10th Annual Meeting of the European Urogynaecological Association (EUGA) held in Barcelona, Spain, from 19 to 21 October 2017.
• A previous publication presented the factors associated with patient satisfaction after laparoscopic lateral suspension with mesh: “Patient satisfaction after laparoscopic lateral suspension with mesh for pelvic organ prolapse: outcome report of a continuous series of 417 patients.” Veit-Rubin N, Dubuisson JB, Gayet-Ageron A, Lange S, Eperon I, Dubuisson J. Int Urogynecol J. 2017 Nov;28(11):1685-1693. https://doi.org/10.1007/s00192-017-3327-2. Epub 2017 Apr 17. PMID: 28417156.
• A previously published video article demonstrated the technique of uterine-preserving lateral suspension with mesh: “Uterus-preserving laparoscopic lateral suspension with mesh for pelvic organ prolapse: a patient-centred outcome report and video of a continuous series of 245 patients.” Veit-Rubin N, Dubuisson JB, Lange S, Eperon I, Dubuisson J. Int Urogynecol J. 2016 Mar;27(3):491-3. https://doi.org/10.1007/s00192-015-2859-6. Epub 2015 Oct 17. PMID: 26476819.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Veit-Rubin, N., Dubuisson, J., Constantin, F. et al. Uterus preservation is superior to hysterectomy when performing laparoscopic lateral suspension with mesh. Int Urogynecol J 30, 557–564 (2019). https://doi.org/10.1007/s00192-018-3678-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-018-3678-3