
Abstract
Identifying critical success factors (CSFs) of continuous improvement projects is crucial for management control and operations management domains. Despite the availability of manufacturing-related literature, studies on CSFs in more dynamic and complex healthcare-related operations are scarce. This study, based at a large public tertiary healthcare organization, identifies CSFs in implementing Lean Six Sigma (LSS). 62 LSS projects completed by Green Belts in consultation with Black Belts were analyzed for project success by a review team of practitioners (Black Belters) and academics. Using a grounded theory approach, numerous success factors were initially identified. A series of brainstorming sessions and workshops helped to narrow down and revise all the CSFs present in each of the 62 LSS projects to eight CSFs. The success of the 62 completed projects was assessed against each of the eight CSFs on a five-point Likert scale. Success was measured against whether the project met its stated aim and achieved the Key Performance Indicators that had initially been identified. Finally, the correlations of each factor rating against project success were analyzed to validate the relationship between each success factor and project success. The findings confirm that all eight CSFs identified are significantly correlated to project success. This study contributes to the management control, operations management, and healthcare literature by identifying CSFs of continuous improvement projects and introducing a relatively unique, rigorous, and practically proven evaluation method applied via an industry and academic partnership. Specified CSFs and the method used to identify these will benefit managers of continuous improvement projects.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Many healthcare organizations are challenged by the demands of an increasingly ageing population, rising rates of obesity, and the intensification of lifestyle diseases such as diabetes, heart disease, osteoarthritis, and certain cancers, coupled with inadequate government funding on already strained healthcare organizations (Al-Balushi et al., 2014; Sohal et al., 2021). In a context of resource restraints amid rising demand for services, private and public healthcare systems pursue various methods for continuous improvement. Such methods include process redesigning, which aims to provide care to patients and achieve higher service quality (Chartier et al., 2019). Among the improvement methods successfully deployed in the manufacturing sector, Lean and Six Sigma have gained the most prominence in healthcare. There is, in fact, a tendency to combine the two approaches into Lean Six Sigma (LSS) (Henrique and Godinho Filho 2018). Numerous healthcare organizations have attempted process improvements using LSS to increase efficiency and effectiveness (Stanton et al., 2014; Laureani, Brady, and Antony 2013; de Koning et al., 2006).
Healthcare organizations are in an ecosystem that necessitates a system of management control due to its complexity and the dynamic nature caused by differing objectives (e.g., quality of patient care, efficiency, and cost containment) fulfilled by a multitude of actors (e.g., clinicians and administrators) who work together (Morelli and Lecci 2013). Management control systems play an essential role in organizing and monitoring organizations’ resources and processes. They do this by providing information for planning, control, performance measurement, and decision-making process (Wanderley 2019; Alsharari, 2019). Present-day management accountants integrate flexible, non-financial control systems with traditional financial management control mechanisms to achieve challenging organizational goals (Alsharari, 2019). Conversely, Lean is recognized as a complementary management control philosophy consisting of interdependent practices and is found to be fitting with an organization’s management control mechanisms (Nielsen et al., 2018; Fullerton, Kennedy, and Widener 2014). LSSs apply statistical process control techniques that use data as evidence of knowledge to improve operational processes. Similar techniques are affiliated with management control mechanisms (Dahlgaard et al., 2019). Prior studies suggest that management control mechanisms can either hinder or facilitate the outcomes of Lean implementations (Fullerton, Kennedy, and Widener 2014).
One school of thought argues that, to fully realize the benefits of Lean transformation, traditional control systems should be modified to suit Lean practices (Tillema and van der Steen 2015). Evidence suggests that Lean should be implemented as an integrated management control system (Nielsen et al., 2018; Fullerton, Kennedy, and Widener 2014). Co-existing with concepts of management control, Lean implementation has various implications for management accounting systems. These include (1) changes in the performance measures which are used, such as the introduction of various non-financial/non-traditional information systems (i.e., quality and problem-solving information) and operating performance measures; (2) an increased frequency and dissemination of management accounting data, as Lean practices stimulate a continuous flow of information; and (3) alterations to management accounting systems, which become much simpler due to the streamlining of transaction processing. This thus repeals the necessity for sophisticated costing systems (Tillema and van der Steen 2015). Given this interrelationship and synergy, Lean implementation projects must incorporate management control mechanisms and collaboration across disciplines in controlling input, process, and output aspects to deliver performance benefits (Netland, Schloetzer, and Ferdows 2015). There is emerging evidence that the combined effect of Lean and management control systems can improve the efficiency and reliability of healthcare systems by streamlining operational processes (Mahmoud, 2020). Thus, the conceptual synergy between the two mechanisms must be appreciated as interconnected and reciprocal.
Literature reviews reveal plentiful publications about Lean, Six Sigma, and the hybrid LSS in healthcare (Henrique and Godinho Filho 2018; Mousavi Isfahani, Tourani, and Seyedin 2019; D’Andreamatteo et al., 2015). However, the primary focus in most past publications has been developing and describing Lean practices, benefits, and methodologies. Most empirical literature focusses on Lean or LSS implementation experience (Laureani, Brady, and Antony 2013; McCann et al., 2015; Centauri et al., 2018), how LSS has been implemented (Stanton et al., 2014) or used (Antony et al., 2019), perceptions of its impact (Leggat et al., 2016), and success stories in healthcare (Bhat, Gijo, and Jnanesh 2014; Toledo et al., 2013). Empirical accounts of LSS project implementation in healthcare are relatively few compared to those detailing the solo Lean approach (Henrique and Godinho Filho 2018). Nevertheless, these few studies of healthcare organizations find that LSS has a significant impact on the quality of services provided to patients from a management control and management accounting perspective (Mousavi Isfahani, Tourani, and Seyedin 2019).
At this stage, it is essential to differentiate between project success (the delivery of benefits flowing from a project) and project management success (the delivery of those benefits against performance measures such as cost, quality, and time) (Cooke-Davies, 2002; Zippel-Schultz and Schultz 2011). However, scant literature exists that examines the evidence of factors that affect such continuous improvement project success in healthcare organizations (Stelson et al., 2017; Henrique and Godinho Filho 2018). Specifically, limited attention is given to the success factors of LSS projects. Of the few studies published on Lean implementation projects, Hung et al., (2017) report contextual factors as most critical to implementing and scaling Lean redesign across primary care clinics. In their study, these authors apply a Consolidated Framework for Implementation Research (CFIR), using data gathered through one-on-one interviews and focus groups. Harrison et al., (2016) also investigate how context affects the implementation of Lean projects aimed at improving clinical care delivery. Their approach includes interviews. Stelson et al., (2017) present findings from a survey-based study of factors that affect continuous improvement project success in a hospital using Sociotechnical Systems Theory (STS). This theory aims to improve the performance of work systems by understanding that the behaviors of human actors interact with the operation of technology (Pasmore et al., 2018). Thus, the knowledge and capabilities of workers can be leveraged to advance technological progression for better operational performance. STS theory that incorporates human (social) and technical aspects into a unified model is effective in investigations of continuous improvement phenomena (Stelson et al., 2017). STS theorists demonstrate that the most successful change endeavors are the ones that address both humanistic and operational needs (Holden, 2011).
As an organization integrates new tools and techniques into existing management accounting and control systems, the change required to align new practices with managerial expectations rarely develops easily (Macchia, 2019; Wanderley 2019). Further, a change achieved may not necessarily be positive. It could be constructive or detrimental to the success or failure of an organization’s purpose (Macchia, 2019). A literature review by Macchia (2019) reveals that, although there is a great desire to understand what drives successful change, literature only provides a limited narrative on the phenomenon. In most cases, several critical factors contribute to successful change. These are often combined, making it difficult to measure what contributes to the final picture. Therefore, it is essential to understand the critical factors that facilitate this change, and, in turn, success, when implementing such a non-financial control mechanism. Indeed, project success factors for this hybrid version of LSS in the explicit context of healthcare are not well researched. There is scope for research that can advance the evidence base for a better understanding of continuous improvement approaches in healthcare. Specifically, more information needs to be generated about the factors that drive the success of LSS continuous improvement projects. While many success stories of LSS implementation are evident in the literature, not all organizations have gained tangible benefits. Some attempts, in fact, have turned out to be ineffective (Antony et al., 2012). Unless the determinants of LSS project success are firmly verified, healthcare organizations may struggle to achieve the best outcomes from LSS implementation. Therefore, this study furthers management control knowledge of the factors influencing LSS implementation project success. This is achieved based on research conducted with one of the largest healthcare organizations in Australia. Using a mixed-methods approach, this study identifies the critical factors for LSS project success, which facilitate the delivery of stakeholder benefits (Cooke-Davies, 2002). The discussion above led to the overarching research question developed for this study:
What critical success factors make some Lean Six Sigma implementations in healthcare organizations more successful than others?
The paper is organized as follows: Section 2 reviews management control and LSS literature in general. The section then turns to healthcare specifically, to understand each of its domains and clarify their relationships. Using grounded theory, Section 3 presents the unique research method developed in this study to identify and validate eight CSFs for LSS project success via industry and academic collaboration. Section 4 then presents this study’s findings and Section 5 explains their theoretical and managerial implications. Finally, Section 6 offers the paper’s conclusions, including limitations and future agendas.
2 Literature review
The Literature Review explores the relationship between management control systems and LSS. This section discusses LSS as a continuous improvement methodology for operational processes. It then reviews the healthcare context, to outline the literature on LSS application and potential in the healthcare context.
2.1 Management control systems and Lean Six Sigma (LSS)
Continuous improvement is a key objective of organizations in their pursuit of operational excellence (Antony et al., 2012; Stelson et al., 2017). It is well established that management needs to ensure that their control systems are aligned and configured in order to facilitate continuous improvement initiatives in an organization (Oliver, 2009). Management control systems are formalized procedures that use statistical information to maintain or change patterns in organizational action to improve operational performance (Zarzycka et al., 2019). This is the organization’s control package. It includes components such as management accounting systems (e.g., activity-based cost management, target costing budget systems, and value analysis), planning systems, performance measurement systems, and reward systems, which can be employed to achieve continuous improvement (Oliver, 2009). Consequently, any system that monitors and assists operational procedures, processes, inputs, and outcomes with the objective of sustenance and continuous improvement is a management control system.
As a complementary mechanism, LSS, as a continuous improvement methodology, focuses on reducing cost, improving outcomes of processes, and generating better value for both customers and shareholders (Albliwi et al., 2014). Some scholars extend the scope of management control mechanisms to include Lean thinking, because Lean philosophy relies on non-financial and financial performance measurements (Nielsen et al., 2018). In any case, due to their complementary nature, management control systems need to be suitably modified to suit the transformations of the organization’s operating strategy. They need to embrace operating philosophies (such as LSS) that support continuous improvement (Oliver, 2009; Zarzycka et al., 2019). From a Lean implementation perspective, careful consideration and incorporation of existing management control practices around input, process, and output controls of the Lean program are vital for its success (Netland, Schloetzer, and Ferdows 2015). The literature consistently espouses the notion that continuous improvement philosophies such as Lean thinking or Six Sigma in operations management and management control systems cannot function in silos to optimal performance. Instead, operations and accounting practitioners must collaborate, to ensure that both mechanisms are strategically integrated into a holistic business strategy (Fullerton, Kennedy, and Widener 2014; Scheidt, Thibadoux, and Rosener 2009). Therefore, the success of LSS implementation is as valuable to management accountants as it is operations managers, due to its potential impact and the rapid scaling and spread of the continuous improvement philosophy.
At present, Lean and Six Sigma and the hybrid LSS are the most popular continuous improvement business strategies in manufacturing (Albliwi et al., 2014; Sohal et al., 2021). The two methods have had independent identities since the 1980s, when the terms were first defined. Lean was pioneered in the Michigan plants of Ford and then advanced to the Toyota Production System in Japan, while Six Sigma was established at the Motorola Research Centre in the USA (Laureani, Brady, and Antony 2013). Lean is one of the world’s most influential management concepts. Its origins date back to early US post-war process improvement and later contributions were made by quality specialists such as Edwards Deming and Joseph Juran. The Toyota Motor Corporation successfully adopted these principles as a production philosophy and a quality system (McCann et al., 2015). Lean thinking emphasizes standardization, process improvement, and the elimination of excess inventory (Joosten, Bongers, and Janssen 2009). Originating from Deming’s process improvement theories, Six Sigma aims at a virtually zero-error processes via reduced variability, standardization, and the elimination of activities that do not add value for the customer (De la Lama et al., 2013). Combining the two is an ideal solution. Lean provides a systemic approach but lacks details, organizational structures, and analytic tools for diagnosis. Six Sigma delivers fewer standard solutions but offers an organizational infrastructure and a general analytical framework for problem-solving (de Koning et al., 2006).
The first hybrid of Lean and Six Sigma was introduced in 1986 in the USA by George Group (Salah et al., 2010), but the term Lean Six Sigma was only coined in the literature around 2000 (Antony et al., 2012). LSS is defined in the literature as “a business strategy and methodology that increases process performance resulting in enhanced customer satisfaction and improves bottom-line results” (Snee, 2010, 10). Despite their independent origins, Lean and Six Sigma have proven to be a powerful combination of improvement methods as a hybrid approach (D’Andreamatteo et al., 2015; de Koning et al., 2006; Bhat, Gijo, and Jnanesh 2014; Mousavi Isfahani, Tourani, and Seyedin 2019). By using tools from both toolboxes, LSS’s optimized methodology increases speed while improving accuracy (Laureani and Antony 2012). The hybrid model is proven to improve efficiency and effectiveness more successfully than implementing each approach separately (Albliwi et al., 2014; Antony et al., 2012; Salah et al., 2010). Following the proven positive experience of this hybrid method in leading enterprises, the complementary relationship between Lean and Six Sigma is commonly acknowledged today, with organizations increasingly establishing LSS improvement projects (Salah et al., 2010; Albliwi et al., 2014). The benefits and success stories of LSS in the industrial world are widely emphasized in the literature (Raja & Raju, 2016). LSS seeks to conform to the customer needs, to deliver the right product at the right time, in the right place, at a shortened cycle time, and at a reduced cost, while removing product defects and non-value-adding steps in business processes (Laureani and Antony 2012). The structure of this quality improvement function is formalized for quality implementation roles, borrowing from martial arts hierarchical terminology: Master Black Belt, Black Belt, Green Belt, Yellow Belt, and White Belt (Laureani and Antony 2012; Albliwi et al., 2014; Bhat, Gijo, and Jnanesh 2014).
2.2 Lean six sigma in healthcare
It is evident that LSS is not just confined to manufacturing. It has been adopted by industries such as financial services, call centers, healthcare, IT, textiles, and the chemical industry (Raja & Raju, 2016). The healthcare sector’s growing interest in adopting methods used in the industrial sector for their own continuous improvement of services has caused the prominence of LSS in healthcare (Henrique and Godinho Filho 2018; Raja & Raju 2016). LSS possesses the same potential to contribute to the healthcare sector as is found in its proven contribution to the automotive industry. This may include clinical and operational support, financial administration, waste elimination, increased quality, safety, and efficiency (Laureani, Brady, and Antony 2013; Sohal et al., 2021). Lean and Six Sigma are contrasting methods but work well together reciprocally in healthcare (Henrique and Godinho Filho 2018). Lean in healthcare organizations can focus on improving the value stream and patient flow while eliminating waste and making problems visible (Arthur, 2011). Six Sigma deals with different kinds of problems, focusing on the accuracy and precision of the processes while providing statistical tools to improve quality and reduce variation in performance (Antony and Kumar 2012). Despite these divergent lenses, both methods refer to customer needs, cost reduction, and process improvement (Arthur, 2011). The hybrid LSS method provides a practical framework for continuous improvement practice in healthcare by controlling cost, improving quality, and providing better healthcare services (de Koning et al., 2006). Antony et al., (2019) report the use of LSS in reducing medication errors in the Norwegian public healthcare context. Bhat, Gijo, and Jnanesh (2014) explore the successful deployment of LSS in the Indian healthcare sector, specifically in the Health Information Department of a Medical College hospital in India. Their study found improvements in patient registration cycle time and reductions in average waiting time, queue length, and staff utilization. Laureani, Brady, and Antony (2013) describe a case study in an Irish hospital that demonstrates that LSS projects can deliver sizeable benefits even when implemented by novices.
The application of LSS in healthcare is at an early stage, relative to its use in the automotive industry (Laureani, Brady, and Antony 2013). Critical success and failure factors for continuous improvement projects in manufacturing are well-identified in the literature (Farris et al., 2009; Albliwi et al., 2014). However, empirical evidence on healthcare success factors is scarce (Al-Balushi et al., 2014). Nevertheless, the literature presents growing evidence of factors affecting Lean implementation project success. Al-Balushi et al., (2014), through a review of literature, reveal the critical readiness factors (foundational mechanisms) for the success of Lean deployment in healthcare organizations. Leadership, organizational culture, communication, training, measurement and reward systems, a decentralized management style, and an end-to-end process view were found to be important in a healthcare context.
Other empirical studies focusing on factors critical to the acceptance of Lean redesign include the following. Hung et al., (2017) identify several Lean implementation success factors: time and intensity of exposure to changes, top-down (as opposed to bottom-up) implementation styles, the degree of employee engagement in developing new workflows, a clinic’s culture and style of leadership, the availability of information about Lean’s effectiveness, individual and team characteristics regarding changed work roles, and related issues of professional identity, authority, and autonomy. Harrison et al., (2016) find that the intra-organizational characteristics shaping Lean project outcomes include CEO commitment and active support for it, prior organizational capacity for quality improvement-based performance improvement, the alignment of the Lean initiative with the organizational mission, the dedication of resources and experts to Lean, staff training before and during projects, the establishment of measurable and relevant project targets, and the planning of project sequences that enhance staff capabilities and commitment. Stelson et al., (2017) identify managerial and employee factors that affect project success, including managerial support, communication, and affective commitment (the extent to which employees perceive the change as being necessary). However, the projects of five Masters students incorporated into a paper by Laureani, Brady, and Antony (2013) provide the only findings so far that touch on the success factors of LSS projects in healthcare. Support from top management and regular communication with stakeholders are the critical project success factors that they identified. The other success factors identified were the involvement of staff, the clear communication of project objectives, the availability of data, the commitment of the process team to the change process, and support for the change of infrastructure.
The knowledge gap in LSS project success factors in general and in healthcare (and linking LSS to management control systems) suggests a need for more research on this specific intersection. Therefore, in contrast to previously published papers, this paper investigates exclusively LSS implementation projects for their project success factors, analyzing empirical data collected during an LSS implementation and evaluation process.
Studies on Lean implementation success have employed traditional methodologies. This study follows a more practice-based, grounded-theory-centered methodological approach developed by industry professionals and academics in partnership. This is a different methodological approach to prior studies on LSS improvement projects. A study where practitioners themselves (in consultation with academics) use grounded theory to analyze LSS project implementation documents to identify and evaluate success factors (grounded in those documents) is scarce in general literature. This is specially the case when it comes to the intersection between management control systems and continuous improvement in the healthcare sector. Given LSS’s association with management control systems, research examining its adaption to the specific healthcare domain can be relevant to healthcare accounting scholarship. The decision contexts of healthcare delivery processes are particularly unique and complex (Morelli and Lecci 2013). Thus, identifying CSFs in LSS implementation in the critical context of healthcare could be pertinent to all sectors.
3 Methodology
This section describes the context for the study and outlines the methodology. First, it discusses the case of LSS Implementation by a tertiary healthcare organization in Melbourne. Then it moves on to the method used by a team of practitioners and academics to identify the CSFs and validate them.
3.1 A case of LSS implementation by a healthcare organization
This study was based on a large public tertiary healthcare organization in Melbourne, Australia. The initiative for LSS redesign first got underway when a new CEO was appointed in 2007. In her previous post, the new CEO had a close professional relationship with a large Australian bank that had pioneered LSS implementation in the financial sector and had established a national training center to train its staff in the implementation of LSS conversion projects. The CEO built on her relationship and tapped into the bank’s LSS initiative. In 2009, five staff from the healthcare organization were trained by the bank as LSS Black Belts. Black Belts possess knowledge and experience of using sophisticated statistical techniques and problem-solving approaches. They are therefore highly competent as on-site consultants and trainers for LSS applications (Voehl et al., 2013; Laureani and Antony 2012). Soon after the training was completed, one of the five Black Belts resigned from the healthcare organization. The remaining four were entrusted with training staff members as Green and White Belts to drive LSS implementation across the healthcare organization. Starting in 2009, the healthcare organization initiated 116 Green Belt projects over a five-year period. Each individual was coached by an LSS Black Belt. The implementations of these projects were predominantly led by the Green Belts. Green Belts were authorized to lead process improvement projects and train other staff on tools and analysis within a single division or location (Voehl et al., 2013; Laureani and Antony 2012). This paper examines the factors that helped achieve success in Green Belt LSS projects across healthcare organizations.
3.2 Steps involved in identifying success factors
The first step in identifying success factors was to inspect documentation for each project conducted during a period of five years (2009–2014). The expert review team consisted of two practitioners with over 20 years of experience in process improvement (who were also LSS Black Belts) and two senior academics who had studied the process improvement domain for over twenty years.
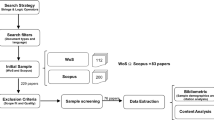
As the first step, the review team’s two LSS Black Belts conducted a very rigorous inspection of all implementation documents for each of the 116 projects. This included examining all change processes, measures, and outcomes. The documents included DMAIC (Define, Measure, Analyze, Improve, and Control) qualitative and quantitative tools that ensure the change management process is monitored and controlled at each stage (Toledo et al., 2013). The DMAIC framework focuses on precise measurement and statistical control of process variability throughout each project (Stanton et al., 2014). The first phase of the review identified that, of the 116 LSS projects commenced during the five-year period, 62 (53%) had been completed and 54 (47%) were yet to be completed or had been abandoned for a range of reasons.
Next, the full review team of two academics and two practitioners assembled for the second phase. The team conducted a workshop to analyze the 62 completed projects for project success. In an LSS project, objectives must be clearly stated from the outset (Laureani, Brady, and Antony 2013). Realization of initial project objectives was compared against project outcomes to categorize whether or not a project had been successful. No bias in the review process was assumed, given that the project objective and outcome were clearly documented in reports in most cases via statistics (See Table 1 for examples). This review process identified 41 projects that had been successful in achieving project objectives and delivering stakeholder benefits. This represented a 66% success rate in completed projects. Examples of successful projects and their outcomes are displayed in Table 1.
The next objective of the review team was to identify what factors enabled project success. The third phase consisted of a series of brainstorming sessions. Workshops were conducted for this purpose. All DMAIC documentation for each project was examined. In this, incomplete or unsuccessful projects served as a counterpoint when looking for project success. Since a number of unknowns were being investigated, a grounded theory approach was deemed better suited to such emerging and complex research situations (Glaser & Strauss, 1967; Charmaz and Belgrave 2007). The grounded theory promotes an open mind in a qualitative investigation to uncover new and unbiased concepts inspired by emerging patterns (Glaser & Strauss, 1967; Charmaz and Belgrave 2007). Numerous success factors were identified in the first round of analysis. The review team revised the list through a series of brainstorming sessions and ultimately narrowed it down to eight CSFs. This grounded-theory-based exercise first helped identify a range of success factors via document review. It then aided the review team to filter this range down to eight critical success factors. Through a series of brainstorming exercises, the team found these eight factors significant when implementing projects in healthcare
The review team then assembled again to conduct another series of brainstorming sessions, in order to refine the eight CSFs. These sessions helped distil sentence clarity, confirm the relevance of the CSFs, and confirm content validity. Finally, the review team were able to develop eight simple statements using a series of meticulous steps. These steps were:
-
1)
There were efficacious governance and strong performance monitoring of the project.
-
2)
There was a well-defined scope, with a clear determination of what was in and out of scope.
-
3)
The project lead was actively involved in all aspects of project management.
-
4)
There was active and effective Executive Sponsor support when required.
-
5)
The process owner was actively involved early on and accepted responsibility for developing sustainable solutions.
-
6)
Staff affected by the project were actively engaged and participated in developing solutions.
-
7)
The deployment of solutions was well planned and executed.
-
8)
A clear and thorough sustainability plan was put in place, which overtly prescribed corrective actions.
A ‘sense making’ workshop between the lead practitioner and the lead academic confirmed that these statements were recognizable constructs that merited investigation.
As the fourth step, the review team subsequently rated each of the 62 completed projects against each of the eight CSFs. Project documentation for all completed projects was again examined thoroughly for this exercise. The strength of the impact of each factor was rated on a Likert scale of one to five. Strongly Disagree, Disagree, Undecided, Agree, and Strongly Agree were the five options. The rating process involved a series of project documents, which were reviewed independently by each practitioner for each of the 62 projects. The practitioners independently rated each CSF. There was then a workshop in which they compared notes and agreed on a rating of each CSF for each project. Thereafter, the ratings were independently verified in a workshop format with academics. It was a rigorous and time-consuming collaborative process. What started with document reviewing led to identifying eight CSFs, and then to rating each of the 62 projects under each of the eight CSFs. As described above, the strength of each factor’s impact was rated on a Likert scale of one to five (Strongly Disagree, Disagree, Undecided, Agree, and Strongly Agree) by the review team for each of the 62 completed projects against each of the eight CSFs. This means that the maximum presence of each CFS for a single LSS project was rated as five.
Each of the eight CSF ratings (1–5) was aligned against the project success or failure (1–0) for all 62 projects for analysis purposes. Project success was measured against the following criteria: (i) whether the project met its stated aim and (ii) whether the project met the Key Performance Indicator that had initially been identified.
The correlations of each factor rating against project success were analyzed to test the relationship between each success factor and project success. A given relationship validated whether or not the identified CSFs were related to project success. In the broadest sense, correlation is a simple statistical method to calculate and interpret. It refers to the degree to which a linear association exists between two continuous variables (Mukaka, 2012). Pearson’s Correlation Technique is one of the most popular for quantitative variables, whereas Pearson’s Correlation Coefficient measures the strength of the linear relationship between two such variables (Hauke and Kossowski 2011). The Pearson correlation coefficient (p) evaluates how far each observation deviates from the best-fit line (a measure of precision) (Lawrence & Lin, 1989). Cohen, (2013) provides perhaps the most broadly accepted guidelines or operational definitions. These are more realistic than other typically found standards for interpreting the scale of correlation coefficients (Hemphill, 2003). In terms of the magnitude of effect sizes, Cohen (2013) stipulates that correlation coefficients below 0.10 are “small”, those between 0.10 and 0.30 are “medium”, and those of 0.50 are “large”. Cohen’s guidelines are primarily based on extensive experience with effect sizes and correlation coefficients (Hemphill, 2003).
Thereafter, the academic team conducted a comprehensive literature review on identified CSFs. They undertook this review to check reliability and validity as a means of substantiation by the literature, so as to better understand each construct.
4 Findings and discussion
This section discusses findings in terms of the validity of each CSF for project success. The eight CSFs are then discussed in detail and their relationship with the existing literature identified.
4.1 Findings
This study’s analysis of correlations between each success factor rating and project success/failure suggests that each factor is significantly correlated (at 0.01 level) to success. The findings demonstrate that project success increases in the more significant presence of factors that the LSS Black Belts and academics found to be favorable to project success via their document review exercise. Project failure is more likely to be an issue when these factors are weak in LSS implementation projects in healthcare (Fig. 1).

Depicts the Pearson correlation coefficient of each relationship. Examination of the magnitude of coefficient effect sizes reveals that all correlation coefficients are above 0.50 except for the second factor, which is close to 0.50 (Cohen, 2013)
Figure 1 depicts correlation coefficients of the LSS success factors identified by the LSS experts. It also reveals the success and failure of the 62 projects implemented in the Melbourne healthcare organization. Therefore, this chart shows the relationship between LSS success factors and project success in the LSS implementation in healthcare organizations.
“Deployment of solutions was well planned and executed” is the most correlated factor in project success, indicating the importance of planning and precisely following up with the plan. Closely correlated is “a clear and thorough sustainability plan was put in place, which overtly prescribed corrective actions”, again stipulating the importance of meticulous planning. Overall, meticulous planning and precise execution are demonstrated to be highly important for LSS implementation project success in healthcare. It can also be observed that governance and performance monitoring, sponsorship, and stakeholder engagement are three factors equivalently correlated to project success.
4.2 Discussion of Critical Success Factors
This section of this study discusses each of the eight CSFs for LSS implementation projects in the healthcare sector. These factors had been earlier identified and validated via a unique and rigorous methodology. This section’s discussion relates the CSFs to the literature on LSS in healthcare specifically, as well as to generic continuous improvement project literature. The correlation coefficient indicates the strength of the relationship of each CSF present in each of the 62 projects against the success of each project, as reported in Fig. 1.
4.2.1 CSF 1: governance and performance monitoring
“There were efficacious governance and strong performance monitoring of the project” as a CSF had a strong relationship (the fifth strongest) to project success, with a correlation coefficient of 0.719. Project governance provides the structure through which a project’s objectives are set. The means of attaining them and monitoring performance are determined through a set of relationships among stakeholders (Joslin and Müller 2016). Project success correlates with stakeholder-oriented forms of governance, such as those prevalent in participative and cohesive organizations with strong shared values due to stewardship relationships (Joslin and Müller 2016). Nevertheless, forms of governance that emphasize control mechanisms can be detrimental to projects and hinder people’s ability to deliver benefits through projects (Joslin and Müller 2016). Governance is crucial to sustain and optimize operational performance in methods such as Lean or LSS (Spanyi, 2010).
Furthermore, project success is more likely when such stakeholder orientations are reflected in performance monitoring processes that go beyond control measures associated with costs and schedules (de Carvalho, Patah, and de Souza Bido 2015). LSS implementation projects require measuring the baseline performance of each process and the potential difficulties encountered due to lack of performance monitoring (Antony et al., 2019). De Carvalho, Patah, and de Souza Bido (2015) emphasize that there is no simple way to define appropriate performance measures against which to monitor success, which is necessarily defined differently in different projects, contexts, and stages from different stakeholder perspectives.
4.2.2 CSF 2: well defined scope
“There was a well-defined scope with a clear determination of what was in and out of scope” had the weakest relationship out of the eight CSFs. However, it was closer to having a strong relationship (0.5) to project success, with a correlation coefficient of 0.498. In the context of LSS improvement projects in healthcare, De la Lama et al., (2013) argue for the importance of project scoping to ensure problems are adequately defined early on. This helps team members understand potential impacts on the quality of their care, patient satisfaction, and the team and its broader context. In a more general sense, Aubry, Richer, and Lavoie-Tremblay (2014) argue that understanding scope allows for effective organizational design to facilitate change. Furthermore, in the UK context, Antonacci et al., (2018) find detailed project scoping to help align individual project tasks with the overall organizational picture and frame the project within its context. This is important for guiding improvement project teams. Similarly, Gorrell (2012) finds that failure to effectively scope improvement project boundaries can constrain the potential for quality improvement. Finally, Greenhalgh (2018) argues that controlling scope creep is a key factor in improving the success of technology projects in health and social care settings.
Nevertheless, as with other themes in the literature, a tension between rigid and emergent scoping is evident. Several scholars argue that while well-defined project scopes may be appropriate for incremental innovations and straightforward problems exploratory projects especially may benefit from less rigid scoping and an emergent flexibility that ensures creativity, new learning, and adaptation (Zippel-Schultz and Schultz 2011; Brown and Eisenhardt 1995).
4.2.3 CSF 3: project lead involvement in project management
“The project lead was actively involved in all aspects of project management” had the second weakest (yet still strong) relationship to project success, with a correlation coefficient of 0.659. The involvement of project leads in the project management process emerges from the healthcare project management literature as an important factor for project success; again the importance of support and facilitation are emphasized alongside the ability to flexibly transition between ‘enabling’ frontline facilitation and ‘managing’ the project (Kislov, Humphreys, and Harvey 2016). Project leaders in such LSS implementation projects are Black Belts or Green Belts with expertise in tools and are trained in a curriculum that resembles that of Six Sigma with additional Lean components (de Koning et al., 2006; Al-Balushi et al., 2014). They are trained in project management, problem-solving methodology, and statistical methods (De la Lama et al., 2013). An essential characteristic of the project leader is vision setting, which involves the cognitive ability to interlace various factors in order to create a holistic view and communicate it to the team (Brown and Eisenhardt 1995). Leadership’s strategic actions aid in the sustainable operation of the clinical, operational, and administrative departments, changing the hierarchical culture of the healthcare setting (Al-Balushi et al., 2014). Arumugam, Antony, and Kumar (2013) find that, in Six Sigma projects, a project leader influences knowledge creation via facilitation, coordination, and a synthesis of individual knowledge into team-level improvement solutions. However, one of the most important tasks of a quality improvement (QI) project leader is transitioning from the active project phase to the longer-term sustainability phase (Chartier et al., 2019). The involvement of supportive leads clearly reinforces participants’ commitment to the improvement process and brings about workable solutions to problems that would be identified and implemented (Harrison et al., 2016).
4.2.4 CSF 4: active and effective executive sponsorship
“There was active and effective Executive Sponsor support when required” had the third strongest relationship to project success, with a correlation coefficient of 0.753. Like governance and performance monitoring, project sponsorship has multiple configurations, only some of which seem to enhance project outcomes (Bryde, 2008; Sense, 2013). Sponsorship activities that are internally-focused (such as supporting the project manager, the team members, and project management processes) help facilitate positive project outcomes (Bryde, 2008; Cooke-Davies, 2002). Sense, (2013) also finds that the project sponsor role has important implications for project success through its stewardship of learning on projects through dynamic interaction with project team members. Thus, to ensure project success, organizations should ensure that the project sponsor role is well-defined and communicated to sponsors in a way that fulfils relations with both external stakeholders and internal supporting activities (Bryde, 2008).
Sponsorship is addressed in the generic project management literature. However, executive sponsorship seems to be particularly emphasized within the healthcare literature on improvement projects. In the context of projects arising from organization-wide improvement efforts, executive leadership is uniquely positioned to understand how services are integrated across the organization to promote and support the importance of improvement projects (Holden, 2011). Therefore, it is key that individuals at this level of the organization demonstrate a fundamental belief in the need for improvement and are actively involved and willing to demonstrate their support of projects when issues arise (Al-Balushi et al., 2014). Further, executive sponsorship is imperative to secure material and non-material resources such as time, education, and information (Al-Balushi et al., 2014; Holden, 2011). Executive sponsorship also provides critical support for flexibility and individual initiative within projects (Ben-Tovim et al., 2007; Grove et al., 2010) show how, without it, the extent to which goals can be achieved and sustained is limited.
4.2.5 CSF 5: process owner involvement and responsibility
“The process owner was actively involved early on and accepted responsibility for developing sustainable solutions” had a strong relationship to project success, with a correlation coefficient of 0.66. Six Sigma provides an organizational structure of project leaders and project owners, where members of upper and middle management generally play the role of project owners or champions (de Koning et al., 2006). They are the immediate supervisors of the business area related to the project and those responsible for the day-to-day operations of the business process (Ramabadron, Dean, and Evans 1997). The role of the process owner is to design a control plan, implement corrective actions, design an audit plan, and monitor continuously (Salah et al., 2010). Process owners are considered one of the pillars of Six Sigma and are responsible for the performance of their designated processes (Torok, 2004). It is the Executive Steering committee that identifies the owner of the selected process (Sharon et al., 1997). The success of projects can be directly influenced by the process owner’s involvement. In contrast, in a healthcare environment, process owners are usually clinicians (e.g., doctors and surgeons, nurse managers, lab supervisors, dietitians, physical therapy department leaders, and emergency room directors). Without their involvement and support, success at the clinical level is, in fact, difficult (Creasy, 2017).
4.2.6 CSF 6: stakeholder engagement and participation
“Staff affected by the project were actively engaged and participated in developing solutions” had the third strongest relationship to project success, with a correlation coefficient of 0.774. Early in projects, appropriate and systematic stakeholder engagement is important in aligning stakeholders and reducing socio-political complexities related to people, power, politics, agendas, and conflicts (Maylor & Turner, 2017). As Winch (2014) suggests, considering projects as temporary configurations and coalitions of people within permanent organizations dedicated to delivering particular outputs may be a useful way of conceptualizing projects in a way that brings stakeholder engagement to the fore. In Lechler’s (1998) words, “When it comes to project management, it’s the people that matter”.
In the complex professionalized context of healthcare, stakeholder engagement is particularly challenging, due to the wide range of stakeholders (e.g., government, organizations, professions, and healthcare consumers). As a starting point for projects, there must be some recognition of the need for improvement among those who carry out the work that will be affected by the change. Without this, improvement projects risk being perceived as cost-cutting efforts at odds with the values of healthcare. They therefore risk the withdrawal of staff and potential resistance (Holden, 2011). Ideally, new projects are generated by professionals themselves in response to work challenges (De la Lama et al., 2013). Furthermore, the professionals who own and live the process must also have the opportunity to share their interpretations of the issues to be addressed (van Offenbeek and Vos 2016), participate in the design of solutions, and be given responsibility for their implementation and ongoing refinement (Grove et al., 2010; Centauri et al., 2018). More recently, there has been increasing recognition of the importance of engaging relevant consumer groups in designing and implementing healthcare projects (Al-Balushi et al., 2014; Sohal et al., 2021).
4.2.7 CSF 7: deployment of solutions
“Deployment of solutions was well planned and executed” had the strongest relationship to project success out of the eight CSFs, with a correlation coefficient of 0.896. A number of researchers have highlighted that planning is a key factor for project success. However, as with governance and performance monitoring, variations among streams of literature emphasize the tensions between control and flexibility in project planning and execution. For example, Koppenjan et al., (2011) highlight the need for a focus on planning and control and the simultaneous necessity for project managers to remain flexible enough to respond to the emerging challenges in complex projects. Along these lines, Kapsali (2013) points out that the field of project management has tended to be dominated by a prescriptive paradigm that artificially separates planning from execution. The author notes that a shift away from rigid planning and control is needed. This promotes a view that values flexibility arising from systems thinking in projects.
4.2.8 CSF 8: sustainability planning
“A clear and thorough sustainability plan was put in place, which overtly prescribed corrective actions” possessed the second strongest relationship to project success, with a correlation coefficient of 0.887. The healthcare improvement literature emphasizes the importance of sustainability planning throughout the lifespan of projects, from their conception. This could be enacted, for example, through (1) the alignment of project goals with long-term organizational objectives (de Koning et al., 2006), (2) the establishment of the architecture for sustainability (e.g., training, budget, and executive support) and, continuously, (3) ongoing evaluation, adjustment, and planning for further changes in an evolutionary process (e.g., in Plan, Do, Check, and Act cycles) (Holden, 2011). Kislov, Humphreys, and Harvey (2016) also highlight the importance of ongoing adaptation. They caution the damaging potential of ‘sustainability objectives in the form of target-related improvement goals that align with compliance-focused institutional imperatives but constrain the ability of actors in this context to make their way toward genuine long-term sustainability iteratively’.
4.3 Key drivers for LSS project success
We can identify three key drivers of success from the data (Fig. 1 scores the overall presence for each CSF in all 62 projects). The first driver that was essential in project success is active and visible leadership. The whole Lean initiative at the hospital was established by its CEO. Through her Executive sponsorship, she provided leadership, support, and the necessary resources, including the training of the quality improvement team in LSS methods and tools. This support and endorsement were clearly reflected in the next four CSFs (Fig. 1). The initiative was taken seriously. The project leads were involved in project management, the projects contained a well-defined scope, the overall governance and performance monitoring was of a high quality, and active and effective Executive sponsorship was recognized.
The second driver of success is a recognition of the complexity of health services projects. This was reflected in projects with process owner involvement and responsibility and where the deployment of solutions was well planned (Fig. 1). In healthcare, process owners are usually clinicians. Getting these clinicians on board with management-focused projects is about flexible, rather than rigid, processes. However, this challenge helps explain why the next key driver of success, ‘winning hearts and minds,’ was more problematic.
Third, both stakeholder engagement and sustainable projects are rated as CSFs (Fig. 1). Clinicians are often skeptical and cynical about management ‘fads’. To engage them in workplace change means that they must view the project as relevant and valuable. A project management mindset that focuses on measures such as time limits and budget capacities can devalue important contributions from key actors who often have a different set of values.
5 Implications
Evidence is scarce in the literature about factors that affect such continuous improvement project success in healthcare organizations (Stelson et al., 2017; Henrique and Godinho Filho 2018). CSFs in continuous improvement projects have been explored before. However, to the authors’ knowledge, no study to date has attempted to identify CSFs of LSS implementation in the healthcare sector. Importantly, this study identified not just the factors. Their relationship to overall project success was also verified to reinforce their validity. In contrast to previously published papers on this theme which have employed traditional methodologies this paper’s reports capture empirical evidence and the methodology used throughout the LSS implementation and subsequent evaluation process. In particular, the study reports a rare, practice-based, grounded-theory-centered methodological approach, used in a collaborative exercise as an industry-academic partnership. This constitutes a unique approach when compared to prior academic studies reporting improvement initiatives. It is a rare feat for practitioners themselves (in consultation with academics) to conduct a hospital-wide practical exercise using a grounded-theory approach in order to analyze LSS project documents and thus identify and evaluate success factors grounded in those documents. The study also takes a mixed-method approach, reporting both qualitative and quantitative analysis processes followed during the evaluation process. These findings are externally validated via the literature to reinforce trust in these identified success factors. The uniqueness of this paper is further highlighted by the interdisciplinary approach that intersects the disciplines of management control, operations management, and healthcare.
5.1 Practical implications
The success factors of LSS implementation in healthcare operations are not only important as a quality control methodology that seeks continuous improvement in healthcare processes. They are also critical for management control systems that seek complementary methodologies. Therefore, the finding that provides actionable guidelines for LSS success is valuable to management accountants, operations managers, medical administrators, and clinicians who endeavor to implement LSS. It is fair to state that the reported rigorous evaluation approach followed by highly qualified LSS Black Belts in consultation with leading academics who have specialized in this domain for decades covers more bases in general. This approach thus may gain more acceptance in the practical domain (Scheidt, Thibadoux, and Rosener 2009; Tillema and van der Steen 2015).
The implications for practice emerging from these findings include the importance of continuous review and feedback loops to key stakeholders, identifying champions (especially clinicians), focusing on what is working and what is not, and celebrating success. The ability to identify barriers and constraints and engage end-users in solutions are critical capabilities of project management practitioners.
The eight success factors of LSS implementation that this study has identified can form sound initial essentials for practitioners to explore. This will help them make informed decisions when managing LSS implementation projects in healthcare systems. It can be argued that, if these success factors are applicable within the demanding and dynamic nature of healthcare, the same can be applied to other industries which are generally more modular and flow-oriented. Practitioners must foster these success factors within their ecosystem while LSS implementation ensures that the LSS project becomes a success.
The mixed-method approach that was applied first to identify the success factors qualitatively and quantitatively and then to apply quantitative techniques to validate them is an applicable and tested method. This is the case not just in healthcare operations but also in other industries. As a successfully tested and validated approach in a very complex and dynamic healthcare setting, practitioners of all domains can adopt this method or modify it to suit their own operation, given that Lean philosophy itself is universally adaptable and general processes in most industries are more linear and flow-based than healthcare contexts.
5.2 Contribution to knowledge
This study contributes to knowledge by identifying CSFs of LSS implementation in healthcare and verifying their validity.
This practitioner-led exercise started with a clean canvas with no prior literature as a foundation in a grounded-theory-based approach, to identify CSFs from project documentation.
LSS interventions can make tasks faster, more productive, and more efficient. They involve operational technicalities and those who execute these processes. This transformation thus requires interaction between social (human behavioral) and technical elements (technologies), to achieve better operational performance (Pasmore et al., 2018). STS theory explores the interaction between these two elements. Prior studies (e.g. Stelson et al., 2017) have used STS theory to empirically identify continuous improvement project success. This project’s findings represent the notion that technological advances and human aspirations could be achieved jointly. The validated eight CSFs of this study incorporate both human (social) and technical aspects, aligning with STS theory. Therefore, this paper’s findings extend the STS approach because they identify relatively discrete CSFs grounded in LSS implementation projects through a relatively new method. As the STS approach intends, these eight CSFs may facilitate the implementation of change. Therefore, these findings further demonstrate that successful change endeavors address both humanistic and operational needs, substantiating the STS theory (Holden, 2011). The principles of STS will be more relevant than ever in facilitating envisioned pervasive improvement initiatives that unify the evolution of social systems with cutting-edge technologies and increasing digitization.
The knowledge contribution of this paper occurs primarily at the intersection of management control, operations management, and healthcare domains, by shedding light on the success factors for continuous improvement projects. Given LSS’s complementary association with management control systems, the findings of this research can be particularly interesting for management control scholars to evaluate the feasibility of implementing complementary control mechanisms on top of traditional systems (Dahlgaard et al., 2019; Nielsen et al., 2018). More specifically, this study’s findings are relevant for the knowledge area of management accounting change.
The mixed-method approach that this project applied using grounded theory is methodologically relatively unique compared to the methods previous authors have applied. In fact, this method has been tried and proven in the practical domain after being developed through a collaborative exercise by practitioners and academics in a very complex healthcare domain. Scholars can therefore now replicate the study method to test the success of continuous improvement projects in different industries. The method should prompt researchers to think further about applying even more innovative and practically focused methods.
6 Conclusions
The overall aim of this paper was to examine the success factors of LSS implementation projects in a large public tertiary healthcare organization in Australia. The key research question was: What are the critical success factors that make some proposed LSS innovations in healthcare organizations more successful than others? A unique and rigorous grounded-theory-based, mixed-method approach was applied for this study. The grounded approach helped the review team retain an open mind during the evaluation process. This, in turn, produced CSFs that were built into the 62 projects with minimum biases. The eight key success factors were not just identified via a thorough analysis of project documents of 62 LSS implementation projects. They were also verified for their relationship with project success through the project data. The top success factors (“deployment of solutions was well planned and executed” and “a clear and thorough sustainability plan was put in place, which overtly prescribed corrective actions”) demonstrate the importance of planning and execution. Governance and performance monitoring, sponsorship, and stakeholder engagement are also vital for project success.
The findings of this paper are significant for both practitioners and academics alike. Provided the eight CSFs are found in the healthcare context in which processes are very complex and dynamic it can be argued that the findings and method used in this study can be applicable for most industry domains (which are arguably more linear and flow-based) with a slight modification or customization to suit their own operation. This study’s method was derived and implemented successfully by practitioners. This may give project managers and management control professionals the confidence they need to accept the method. Scholars from management control systems, operations management, and healthcare disciplines may benefit from the study’s findings and the practice-based methodology used when exploring the success of continuous improvement projects.
This paper contains some limitations, which provide directions for future studies. Its research uses a quantitative-based method. A qualitative enquiry may provide in-depth findings. Thus, a qualitative enquiry based on identified CSFs in the healthcare sector or another industry could be of value. Likewise, the method applied to identify and verify the CSFs should be tested in other sectors for future replicative study. Since the objective was to determine what factor makes an LSS project successful, factors that may have a negative impact on project outcomes are beyond the scope of this paper. They should be included, however, in a future research agenda.
References
Al-Balushi, S., Sohal, A. S., Singh, P. J., Al Hajri, A., Al Farsi, Y. M., & Al Abri, R. (2014). Readiness factors for lean implementation in healthcare settings--a literature review. Journal of Health Organisation and Managagement, 28(2), 135–153. https://doi.org/10.1108/JHOM-04-2013-0083. https://www.ncbi.nlm.nih.gov/pubmed/25065107
Albliwi, S., Antony, J., Lim, S. A. H., Ton van der, & Wiele (2014). Critical failure factors of Lean Six Sigma: a systematic literature review. International Journal of Quality & Reliability Management, 31(9), 1012–1030. https://doi.org/10.1108/ijqrm-09-2013-0147
Alsharari, N. M. (2019). Management accounting and organizational change: alternative perspectives. International Journal of Organizational Analysis, 27(4), 1124–1147. https://doi.org/10.1108/ijoa-03-2018-1394
Antonacci, G., Reed, J. E., Lennox, L., & Barlow, J. (2018). “The use of process mapping in healthcare quality improvement projects.“. Health Service Management Research, 31(2), 74–84. https://doi.org/10.1177/0951484818770411. https://www.ncbi.nlm.nih.gov/pubmed/29707978
Antony, J., Forthun, S. C., Trakulsunti, Y., Farrington, T., McFarlane, J., Brennan, A., & Dempsey, M. (2019). An exploratory study into the use of Lean Six Sigma to reduce medication errors in the Norwegian public healthcare context. Leadership in Health Service, 32(4), 509–524. https://doi.org/10.1108/LHS-12-2018-0065. https://www.ncbi.nlm.nih.gov/pubmed/31612783
Antony, J., Krishan, N., Cullen, D., & Kumar, M. (2012). Lean Six Sigma for higher education institutions (HEIs) Challenges, barriers, success factors, tools/techniques. International Journal of Productivity and Performance Management, 61(8), 940–948
Antony, J., & Kumar, M. (2012). Lean and Six Sigma methodologies in NHS Scotland: an empirical study and directions for future research. Quality Innovation Prosperity, 16(2), 19–34
Arthur, J. (2011). Lean Six Sigma for hospitals: Simple steps to fast, affordable, and flawless Healthcare. McGraw-Hill Education
Arumugam, V., Antony, J., & Kumar, M. (2013). Linking learning and knowledge creation to project success in Six Sigma projects: An empirical investigation. International Journal of Production Economics, 141(1), 388–402. https://doi.org/10.1016/j.ijpe.2012.09.003
Aubry, M., Richer, M. C., & Lavoie-Tremblay, M. (2014). Governance performance in complex environment: The case of a major transformation in a university hospital. International Journal of Project Management, 32(8), 1333–1345
Ben-Tovim, D. I., Bassham, J. E., Bolch, D., Martin, M. A., Dougherty, M., & Szwarcbord, M. (2007). “Lean thinking across a hospital: redesigning care at the Flinders Medical Centre.“. Australian Health Review, 31(1), 10–15
Bhat, S., Gijo, E. V., & Jnanesh, N. A. (2014). Application of Lean Six Sigma methodology in the registration process of a hospital. International Journal of Productivity and Performance Management, 63(5), 613–643. https://doi.org/10.1108/ijppm-11-2013-0191
Brown, S. L., & Eisenhardt, K. M. (1995). Product development: Past research, present findings, and future directions. Academy of Management Review, 20(2), 343–378
Bryde, D. (2008). Perceptions of the impact of project sponsorship practices on project success. International Journal of Project Management, 26(8), 800–809. https://doi.org/10.1016/j.ijproman.2007.12.001
Centauri, F., Mazzocato, P., Villa, S., & Marsilio, M. (2018). “System-wide lean implementation in health care: A multiple case study.“. Health Service Management Research, 31(2), 60–73. https://doi.org/10.1177/0951484818768226. https://www.ncbi.nlm.nih.gov/pubmed/29681169
Charmaz, K. & Belgrave, L. L. (2007).Grounded theory: The Blackwell Encyclopedia of Sociology. London
Chartier, L. B., Vaillancourt, S., Cheng, A. H. Y., & Stang, A. S. (2019). “Quality improvement primer part 3: Evaluating and sustaining a quality improvement project in the emergency department.“ CJEM 21 (2): 261-268. https://doi.org/10.1017/cem.2018.380. https://www.ncbi.nlm.nih.gov/pubmed/29925452
Cohen, J. (2013). Statistical power analysis for the behavioral sciences. Routledge
Cooke-Davies, T. (2002). The “real” success factors on projects. International Journal of Project Management, 20(3), 185–190
Creasy, T. (2017). Factors that lead to success or failure in healthcare projects. Quality Progress, 50(2), 24
D’Andreamatteo, A., Ianni, L., Lega, F., & Sargiacomo, M. (2015). Lean in healthcare: A comprehensive review. Health Policy, 119(9), 1197–1209. https://doi.org/10.1016/j.healthpol.2015.02.002. https://www.ncbi.nlm.nih.gov/pubmed/25737260
Dahlgaard, J. J., Reyes, L., Chen, C. K., & Dahlgaard-Park, S. M. (2019). “Evolution and future of total quality management: management control and organisational learning.“. Total Quality Management & Business Excellence, 30(sup1), S1–S16. https://doi.org/10.1080/14783363.2019.1665776
de Carvalho, M. M., Patah, L. A., & de Souza Bido, D. (2015). Project management and its effects on project success: Cross-country and cross-industry comparisons. International Journal of Project Management, 33(7), 1509–1522
de Koning, H., Verver, J. P. S., Jaap, van den Heuvel, S., Bisgaard, Ronald, J. M. M., & Does (2006). “Lean Six Sigma in Healthcare.“ Journal For Healthcare Quality 28 (2): 4-11. https://doi.org/10.1111/j.1945-1474.2006.tb00596.x
De la Lama, J., Fernandez, J., Punzano, J. A., Nicolas, M., Nin, S., Mengual, R. … Ramos, G. (2013). Using Six Sigma tools to improve internal processes in a hospital center through three pilot projects. International Journal of Healthcare Management, 6(3), 158–167. https://doi.org/10.1179/2047971913y.0000000044
Farris, J. A., Van Aken, E. M., Doolen, T. L., & Worley, J. (2009). Critical success factors for human resource outcomes in Kaizen events: An empirical study. International Journal of Production Economics, 117(1), 42–65. https://doi.org/10.1016/j.ijpe.2008.08.051
Fullerton, R. R., Kennedy, F. A., & Widener, S. K. (2014). Lean manufacturing and firm performance: The incremental contribution of lean management accounting practices. Journal of Operations Management, 32(7-8), 414–428. https://doi.org/10.1016/j.jom.2014.09.002
Glaser, B., & Strauss, A. (1967). “The discovery of grounded theory: Strategiesfor qualitative research.“. Sociology The Journal of The British Sociological Association, 12, 27–49
Gorrell, M. (2012). Clinical systems improvement: it’s all about the project boundaries. Journal of Infection Prevention, 13(2), 48–54
Greenhalgh, T. (2018). “How to improve success of technology projects in health and social care.“. Public Health Res Pract, 28(3), https://doi.org/10.17061/phrp2831815. https://www.ncbi.nlm.nih.gov/pubmed/30406256
Grove, A. L., Meredith, J. O., MacIntyre, M., Angelis, J., & Neailey, K. (2010). UK health visiting: challenges faced during lean implementation. Leadership in Health Services, 23(3), 204–218. https://doi.org/10.1108/17511871011061037
Harrison, M. I., Paez, K., Carman, K. L., Stephens, J., Smeeding, L., Devers, K. J., & Garfinkel, S. (2016). “Effects of organizational context on Lean implementation in five hospital systems.“. Health Care Management Review, 41(2), 127–144. https://doi.org/10.1097/HMR.0000000000000049. https://www.ncbi.nlm.nih.gov/pubmed/25539057
Hauke, J., & Kossowski, T. (2011). Comparison of values of Pearson’s and Spearman’s correlation coefficients on the same sets of data. Quaestiones geographicae, 30(2), 87–93
Hemphill, J. F. (2003). Interpreting the magnitudes of correlation coefficients. American Psychologist, 58(1), 78–79
Henrique, D. B., & Godinho Filho, M. (2018). “A systematic literature review of empirical research in Lean and Six Sigma in healthcare.“. Total Quality Management & Business Excellence, 1–21. https://doi.org/10.1080/14783363.2018.1429259
Holden, R. J. (2011). “Lean Thinking in emergency departments: a critical review.“. Annals of Emergency Medicine, 57(3), 265–278. https://doi.org/10.1016/j.annemergmed.2010.08.001. https://www.ncbi.nlm.nih.gov/pubmed/21035904
Hung, D., Gray, C., Martinez, M., Schmittdiel, J., & Harrison, M. I. (2017). “Acceptance of lean redesigns in primary care: A contextual analysis.“. Health Care Management Review, 42(3), 203–212. https://doi.org/10.1097/HMR.0000000000000106. https://www.ncbi.nlm.nih.gov/pubmed/26939032
Joosten, T., Bongers, I., & Janssen, R. (2009). Application of lean thinking to health care: issues and observations. International Journal for Quality in Health Care, 21(5), 341–347
Joslin, R., & Müller, R. (2016). The relationship between project governance and project success. International Journal of Project Management, 34(4), 613–626
Kapsali, M. (2013). Equifinality in Project Management Exploring Causal Complexity in Projects. Systems Research and Behavioral Science, 30(1), 2–14. https://doi.org/10.1002/sres.2128
Kislov, R., Humphreys, J., & Harvey, G. (2016). “How do managerial techniques evolve over time? The distortion of “facilitation” in healthcare service improvement.“. Public Management Review, 19(8), 1165–1183. https://doi.org/10.1080/14719037.2016.1266022
Koppenjan, J., Veeneman, W., van der Voort, H., & Martijn Leijten. (2011). Ernst ten Heuvelhof, and. “Competing management approaches in large engineering projects: The Dutch RandstadRail project.“ International Journal of Project Management 29 (6): 740-750. https://doi.org/10.1016/j.ijproman.2010.07.003
Laureani, A., & Antony, J. (2012). Standards for lean six sigma certification. International Journal of Productivity and Performance Management, 61(1), 110–120
Laureani, A., Brady, M., & Antony, J. (2013). Applications of Lean Six Sigma in an Irish hospital. Leadership in Health Services, 26(4), 322–337. https://doi.org/10.1108/lhs-01-2012-0002
Lawrence, I., & Lin, K. (1989). “A concordance correlation coefficient to evaluate reproducibility.“ Biometrics: 255-268
Lechler, T. (1998). “When it comes to project management, it’s the people that matter: an empirical analysis of project management in Germany.“. IRNOP III. The nature and role of projects in the next, 20, 205–215
Leggat, S. G., Gough, R., Bartram, T., Stanton, P., Bamber, G. J., Ballardie, R., & Sohal, A. (2016). Process redesign for time-based emergency admission targets. Journal of Health Organisation and Management, 30(6), 939–949. https://doi.org/10.1108/JHOM-08-2015-0114. https://www.ncbi.nlm.nih.gov/pubmed/27681026
Macchia, S. (2019). “A review on Management Accounting Change. What’s next?“. Economia Aziendale Online-, 10(1), 107–134
Mahmoud, Z. (2020). “Hospital Management in the Anthropocene: an international examination of Lean-based management control systems and alienation of nurses in operating theatres.“ Macquarie University (Sydney). https://hal.archives-ouvertes.fr/tel-03168940
Maylor, H., & Turner, N. (2017). Understand, reduce, respond: project complexity management theory and practice. International Journal of Operations & Production Management, 37(8), 1076–1093. https://doi.org/10.1108/ijopm-05-2016-0263
McCann, L., Hassard, J. S., Granter, E., & Hyde, P. J. (2015). Casting the lean spell: The promotion, dilution and erosion of lean management in the NHS. Human Relations, 68(10), 1557–1577. https://doi.org/10.1177/0018726714561697
Morelli, M., & Lecci, F. (2013). Management control systems (MCS) change and the impact of top management characteristics: the case of healthcare organisations. Journal of Management Control, 24(3), 267–298. https://doi.org/10.1007/s00187-013-0182-2
Mousavi Isfahani, H., Tourani, S., & Seyedin, H. (2019). Lean management approach in hospitals: a systematic review. International Journal of Lean Six Sigma, 10(1), 161–188. https://doi.org/10.1108/ijlss-05-2017-0051
Mukaka, M. M. (2012). A guide to appropriate use of correlation coefficient in medical research. Malawi Medical Journal, 24(3), 69–71
Netland, T. H., Schloetzer, J. D., & Ferdows, K. (2015). Implementing corporate lean programs: The effect of management control practices. Journal of Operations Management, 36(1), 90–102. https://doi.org/10.1016/j.jom.2015.03.005
Nielsen, H., Kristensen, T. B., & Grasso, L. P. (2018). The performance effects of complementary management control mechanisms. International Journal of Operations & Production Management, 38(11), 2124–2148. https://doi.org/10.1108/ijopm-09-2016-0577
Oliver, J. (2009). Continuous improvement: role of organisational learning mechanisms. International Journal of Quality & Reliability Management, 26(6), 546–563. https://doi.org/10.1108/02656710910966129
Pasmore, W., Winby, S., Mohrman, S. A., & Vanasse, R. (2018). Reflections: Sociotechnical Systems Design and Organization Change. Journal of Change Management, 19(2), 67–85. https://doi.org/10.1080/14697017.2018.1553761
Raja, S. V., & Raju, R. (2016). A systematic literature review of Lean Six Sigma in different industries. International Journal of Lean Six Sigma, 7(4), 430–466. https://doi.org/10.1108/ijlss-12-2015-0050
Ramabadron, R., Dean, J. W., & James, R. E. (1997). Benchmarking and project management: a review and organizational model. Benchmarking for Quality Management & Technology, 4(91), 47–58
Salah, S., Rahim, A., & Carretero, J. A. (2010). The integration of Six Sigma and lean management. International Journal of Lean Six Sigma, 1(3), 249–274. https://doi.org/10.1108/20401461011075035
Scheidt, M., Thibadoux, G., & Rosener, W. S. (2009). How management accountants can become key members of the Six Sigma team. Management Accounting Quarterly, 10(3), 19
Sense, A. J. (2013). A project sponsor’s impact on practice-based learning within projects. International Journal of Project Management, 31(2), 264–271. https://doi.org/10.1016/j.ijproman.2012.06.007
Sharon, L. T., Bitzer, M., & Kamel, M. N. (1997). “Workflow reengineering: a methodology for business process reengineering using workflow management technology.“ Proceedings of the Thirtieth Hawaii International Conference on System Sciences
Snee, R. D. (2010). Lean Six Sigma–getting better all the time. International Journal of Lean Six Sigma, 1(1), 9–29
Sohal, A., Vass, T., Singh, P., Balushi, S. A., Hajri, A. S. A., Farsi, Y. A., & Rashid Al Arbi (2021). “Assessing readiness for lean thinking in healthcare settings: the case for Oman.“ Industrial Management & Data Systems ahead-of-print (ahead-of-print). https://doi.org/10.1108/imds-02-2021-0120
Spanyi, A. (2010). “Business process management governance.“ In Handbook on Business Process Management 2, 223-238. Springer
Stanton, P., Gough, R., Ballardie, R., Bartram, T., Bamber, G. J., & Amrik Sohal (2014). “Implementing lean management/Six Sigma in hospitals: beyond empowerment or work intensification?“. The International Journal of Human Resource Management, 25(21), 2926–2940. https://doi.org/10.1080/09585192.2014.963138
Stelson, P., Hille, J., Eseonu, C., & Doolen, T. (2017). “What drives continuous improvement project success in healthcare?“. International Journal of Health Care Quality Assurance, 30(1), 43–57. https://doi.org/10.1108/IJHCQA-03-2016-0035. https://www.ncbi.nlm.nih.gov/pubmed/28105876
Tillema, S., & van der Steen, M. (2015). “Co-existing concepts of management control.“. Management Accounting Research, 27, 67–83. https://doi.org/10.1016/j.mar.2015.01.002
Toledo, A. H., Carroll, T., Arnold, E., Tulu, Z., Caffey, T., Kearns, L. E., & Gerber, D. A. (2013). Reducing liver transplant length of stay: a Lean Six Sigma approach. Prog Transplant, 23(4), 350–364. https://doi.org/10.7182/pit2013226. https://www.ncbi.nlm.nih.gov/pubmed/24311399
Torok, J. (2004). The Where and Y: A 1-2-3 Model for Project Success. Quality Progress, 37(4), 46
van Offenbeek, M. A. G., & Vos, J. F. J. (2016). An integrative framework for managing project issues across stakeholder groups. International Journal of Project Management, 34(1), 44–57. https://doi.org/10.1016/j.ijproman.2015.09.006
Voehl, F., Harrington, H. J., Mignosa, C., & Charron, R. (2013). The lean six sigma black belt handbook: tools and methods for process acceleration. Productivity Press
Wanderley, & Cláudio de Araújo (2019). “A Process Model of Management Accounting Change Based on the Instituional Theory Contributions.“. Revista de Educação e Pesquisa em Contabilidade (REPeC), 13(4), https://doi.org/10.17524/repec.v13i4.2397
Winch, G. M. (2014). Three domains of project organising. International Journal of Project Management, 32(5), 721–731. https://doi.org/10.1016/j.ijproman.2013.10.012
Zarzycka, E., Dobroszek, J., Lepistö, L., & Moilanen, S. (2019). Coexistence of innovation and standardization: evidence from the lean environment of business process outsourcing. Journal of Management Control, 30(3), 251–286. https://doi.org/10.1007/s00187-019-00284-x
Zippel-Schultz, B., & Schultz, C. (2011). Mediated and moderated effects of business and project planning on innovation projects in hospitals. Creativity and Innovation Management, 20(4), 296–310
Acknowledgements
We thank the Australian Research Council (Project No. LP110200528) for support. We are grateful to a large healthcare organization in Melbourne, Australia for providing research access.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sohal, A., De Vass, T., Vasquez, T. et al. Success factors for lean six sigma projects in healthcare. J Manag Control 33, 215–240 (2022). https://doi.org/10.1007/s00187-022-00336-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00187-022-00336-9