
Abstract
Purpose
There is a lack of robust evidence for the magnitude of the effects of posterior capsular release (PCR) on intraoperative component gaps during total knee arthroplasty (TKA). The purpose of the present study was to quantify and compare the effects of partial versus full PCR on the intraoperative component gaps at various degrees of flexion during posterior-stabilized TKA.
Methods
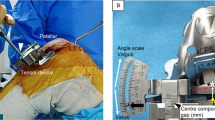
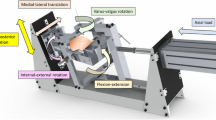
Full PCR was performed on 39 consecutive cases (full PCR group), and partial PCR (the medial side up to and including the intercondylar notch) was performed on the subsequent 39 consecutive cases (partial PCR group) during posterior-stabilized TKA using the measured resection technique for varus knee osteoarthritis. Medial component gaps and varus angles at 0°, 10°, 45°, 90°, and a maximum of flexion were measured with a tensor device before and after the PCR. Differences between the two groups in post-release medial component gap increase and post-release joint varus angle increase were assessed using a t test. Pre- to post-release medial component gaps and joint varus angles in each group were compared using a paired samples t test.
Results
In both groups at 0° and 10° of flexion, post-release medial compartment gaps were significantly greater than pre-release gaps (all P < 0.001). At 45°, 90° and maximum flexion, the medial compartment gap increase did not exceed the minimal detectable change in either group. At 0° and 10° of flexion, there was no significant difference in post-release medial compartment gap change between the two groups. In the full PCR group, post-release joint varus angles at 0° of flexion were significantly greater than pre-release angles (P < 0.001), while there was no significant pre- and post-release difference in the partial PCR group. The change in post-release joint varus angles at 0° of flexion was significantly greater in the full PCR group than in the partial PCR group.
Conclusion
Both full and partial PCR show similar clinical usefulness for increasing the medial component gap at extension and reducing component gap mismatch. A partial PCR can be used to avoid increasing joint varus angles at 0° of flexion.
Level of evidence
Level 2 (prospective comparative study).







Similar content being viewed by others

Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Al-Jabri T, Brivio A, Maffulli N, Barrett D (2021) Management of instability after primary total knee arthroplasty: an evidence-based review. J Orthop Surg Res 16:729
Athwal KK, Milner PE, Bellier G, Amis AA (2019) Posterior capsular release is a biomechanically safe procedure to perform in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 27:1587–1594
Hasegawa M, Naito Y, Yamaguchi T, Wakabayashi H, Sudo A (2018) Factors contributing to patient satisfaction and expectations following computer-assisted total knee arthroplasty. J Knee Surg 31:448–452
Jakobsen TL, Christensen M, Christensen SS, Olsen M, Bandholm T (2010) Reliability of knee joint range of motion and circumference measurements after total knee arthroplasty: does tester experience matter? Physiother Res Int 15:126–134
Jennings LM, Bell CI, Ingham E, Komistek RD, Stone MH, Fisher J (2007) The influence of femoral condylar lift-off on the wear of artificial knee joints. Proc Inst Mech Eng H 221:305–314
Katagiri H, Saito R, Shioda M, Jinno T, Watanabe T (2022) Medial osteophyte resection width correlates with correction of the medio-lateral component gap imbalance during posterior-stabilized total knee arthroplasty. Clin Biomech (Bristol, Avon) 100:105803
Kinoshita T, Hino K, Kutsuna T, Watamori K, Tsuda T, Miura H (2021) Efficacy of posterior capsular release for flexion contracture in posterior-stabilized total knee arthroplasty. J Exp Orthop 8:102
Longo UG, Candela V, Pirato F, Hirschmann MT, Becker R, Denaro V (2021) Midflexion instability in total knee arthroplasty: a systematic review. Knee Surg Sports Traumatol Arthrosc 29:370–380
Mochizuki T, Tanifuji O, Sato T, Hijikata H, Koga H, Watanabe S et al (2017) Association between anteroposterior laxity in mid-range flexion and subjective healing of instability after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 25:3543–3548
Nagai K, Muratsu H, Kanda Y, Tsubosaka M, Kamenaga T, Miya H et al (2018) Intraoperative soft tissue balance using novel medial preserving gap technique in posterior-stabilized total knee arthroplasty: comparison to measured resection technique. Knee Surg Sports Traumatol Arthrosc 26:3474–3481
Nagle M, Glynn A (2020) Midflexion instability in primary total knee arthroplasty. J Knee Surg 33:459–465
Nakahara H, Okazaki K, Hamai S, Okamoto S, Kuwashima U, Higaki H et al (2015) Does knee stability in the coronal plane in extension affect function and outcome after total knee arthroplasty? Knee Surg Sports Traumatol Arthrosc 23:1693–1698
Oh CS, Song EK, Seon JK, Ahn YS (2015) The effect of flexion balance on functional outcomes in cruciate-retaining total knee arthroplasty. Arch Orthop Trauma Surg 135:401–406
Pinter Z, Staggers R, Lee S, Bergstresser S, Shah A, Naranje S (2019) Open posterior capsular release with an osteotome in total knee arthroplasty does not place important neurovascular structures at risk. Knee Surg Sports Traumatol Arthrosc 27:2120–2123
Roth JD, Howell SM, Hull ML (2015) Native knee laxities at 0°, 45°, and 90° of flexion and their relationship to the goal of the gap-balancing alignment method of total knee arthroplasty. J Bone Joint Surg Am 97:1678–1684
Santos C, Ferreira G, Malacco P, Sabino G, Moraes G, Felício D (2012) Intra and inter examiner reliability and measurement error of goniometer and digital inclinometer use. Revista Brasileira de Medicina do Esporte 18:38–41
Seki Y, Katagiri H, Otabe K, Nakagawa Y, Miyatake K, Sekiya I et al (2020) Investigation of association between the preoperative intra-articular anesthetic test and persistent pain after total knee arthroplasty. J Orthop Sci 25:1055–1060
Shalhoub S, Moschetti WE, Dabuzhsky L, Jevsevar DS, Keggi JM, Plaskos C (2018) Laxity profiles in the native and replaced knee-application to robotic-assisted gap-balancing total knee arthroplasty. J Arthroplasty 33:3043–3048
Song SJ, Lee HW, Bae DK, Park CH (2022) Mid-flexion laxity could be identified with continuous flexion-arc gap assessment in patients with a large preoperative convergence angle. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-021-06846-8
Tomaszewski KA, Popieluszko P, Graves MJ, Pękala PA, Henry BM, Roy J et al (2017) The evidence-based surgical anatomy of the popliteal artery and the variations in its branching patterns. J Vasc Surg 65:521-529.e526
Watanabe T, Koga H, Katagiri H, Otabe K, Nakagawa Y, Muneta T et al (2020) Coronal and sagittal laxity affects clinical outcomes in posterior-stabilized total knee arthroplasty: assessment of well-functioning knees. Knee Surg Sports Traumatol Arthrosc 28:1400–1409
Watanabe T, Muneta T, Sekiya I, Banks SA (2013) Intraoperative joint gaps affect postoperative range of motion in TKAs with posterior-stabilized prostheses. Clin Orthop Relat Res 471:1326–1333
Acknowledgements
Midori Tanabe for data registration; Vern Fischer for English language editing.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
HK designed the initial plan, conducted the study, and completed the final manuscript. RS and TJ analyzed the data and drafted the manuscript. MS collected the data. TW designed the initial plan, conducted the study, and edited the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This study was approved by the Institutional Review Board in Dokkyo Medical University Saitama Medical Center (research protocol identification number: 21071).
Informed consent
All the study participants provided their full written informed consent for participation in this clinical research prior to the operative procedure.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Katagiri, H., Saito, R., Shioda, M. et al. Limited medial posterior capsular release increases the intraoperative medial component gap while maintaining the joint varus angle at extension in posterior-stabilized total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 31, 4187–4194 (2023). https://doi.org/10.1007/s00167-023-07425-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-023-07425-9