
Abstract
Purpose
The aim of this study was to describe the epidemiology of Achilles tendon rupture (ATR) and its relationship with socioeconomic deprivation status (SEDS). The hypothesis was that ATR occurs more frequently in socioeconomically deprived patients. Secondary aims were to determine variations in circumstances of injury between more and less deprived patients.
Methods
A 6-year retrospective review of consecutive patients presenting with ATR was undertaken. The health-board population was defined using governmental population data and SEDS was defined using the Scottish Index of Multiple Deprivation. The primary outcome was an epidemiological description and comparison of incidence in more and less deprived cohorts. Secondary outcomes included reporting of the relationship between SEDS and patient and injury characteristics with univariate and binary logistic regression analyses.
Results
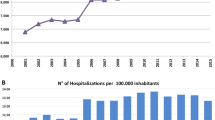
There were 783 patients (567 male; 216 female) with ATR. Mean incidence for adults (≥ 18 years) was 18.75/100,000 per year (range 16.56–23.57) and for all ages was 15.26/100,000 per year (range 13.51 to 19.07). Incidence in the least deprived population quintiles (4th and 5th quintiles; 18.07 per 100,000/year) was higher than that in the most deprived quintiles (1st and 2nd; 11.32/100,000 per year; OR 1.60, 95%CI 1.35–1.89; p < 0.001).
When adjusting for confounding factors, least deprived patients were more likely to be > 50 years old (OR 1.97; 95%CI 1.24–3.12; p = 0.004), to sustain ATR playing sports (OR 1.72, 95%CI 1.11–2.67; p = 0.02) and in the spring (OR 1.65, 95%CI 1.01–2.70; p = 0.045) and to give a history of preceding tendinitis (OR 4.04, 95%CI 1.49–10.95; p = 0.006). They were less likely to sustain low-energy injuries (OR 0.44, 95%CI 0.23–0.87; p = 0.02) and to be obese (OR 0.25–0.41, 95%CI 0.07–0.90; p ≤ 0.03).
Conclusions
The incidence of ATR was higher in less socioeconomically deprived populations and the hypothesis was therefore rejected. Significant variations in patient and predisposing factors, mechanisms of injury and seasonality were demonstrated between most and least deprived groups, suggesting that circumstances and nature of ATR may vary with SEDS and these are not a homogenous group of injuries.
Level of Evidence
Prognostic Study Level III.





Similar content being viewed by others

Abbreviations
- ATR:
-
Achilles tendon rupture
- SEDS:
-
Socioeconomic deprivation status
- LD:
-
Least deprived
- MD:
-
Most deprived
- NHS:
-
National health service
- REC:
-
Regional ethics committee
- NRS:
-
National records of Scotland
- SIMD:
-
Scottish index of multiple deprivation
- IQR:
-
Inter-quartile range
- FET:
-
Fisher’s exact test
References
Aujla RS, Patel S, Jones A, Bhatia M (2019) Non-operative functional treatment for acute Achilles tendon ruptures: The Leicester Achilles Management Protocol (LAMP). Injury 50(4):995–999
Bedrick BS, Eskew AM, Chavarro JE, Jungheim ES (2020) Dietary patterns, physical activity, and socioeconomic associations in a midwestern cohort of healthy reproductive-age women. Matern Child Health J 24(10):1299–1307
Bengtsson C, Nordmark B, Klareskog L, Lundberg I, Alfredsson L (2005) Socioeconomic status and the risk of developing rheumatoid arthritis: results from the Swedish EIRA study. Ann Rheum Dis 64(11):1588–1594
Beynon C, Bailey L (2020) Prevalence of severe childhood obesity in Wales UK. J Public Health 42(4):e435–e439
Bostman OM (1995) Body-weight related to loss of reduction of fractures of the distal tibia and ankle. J Bone Joint Surg Br 77(1):101–103
Brodersen NH, Steptoe A, Boniface DR, Wardle J (2007) Trends in physical activity and sedentary behaviour in adolescence: ethnic and socioeconomic differences. Br J Sports Med 41(3):140–144
Burrus MT, Werner BC, Park JS, Perumal V, Cooper MT (2016) Achilles tendon repair in obese patients is associated with increased complication rates. Foot Ankle Spec 9(3):208–214
Caldwell JE, Lightsey HM, Trofa DP, Swindell HW, Greisberg JK, Vosseller JT (2018) Seasonal Variation of Achilles Tendon Injury. J Am Acad Orthop Surg Glob Res Rev 2(8):e043
Cassell A, Edwards D, Harshfield A, Rhodes K, Brimicombe J, Payne R et al (2018) The epidemiology of multimorbidity in primary care: a retrospective cohort study. Br J Gen Pract 68(669):e245–e251
Chen C, Hunt KJ (2019) Open reconstructive strategies for chronic Achilles tendon ruptures. Foot Ankle Clin 24(3):425–437
Clement ND, McQueen MM, Court-Brown CM (2014) Social deprivation influences the epidemiology and outcome of proximal humeral fractures in adults for a defined urban population of Scotland. Eur J Orthop Surg Traumatol 24(7):1039–1046
Concato J, Hartigan JA (2016) P values: from suggestion to superstition. J Investig Med 64(7):1166–1171
Corfield AR, MacKay DF, Pell JP (2016) Association between trauma and socioeconomic deprivation: a registry-based, Scotland-wide retrospective cohort study of 9,238 patients. Scand J Trauma Resusc Emer Med. https://doi.org/10.1186/s13049-016-0275-7
Cottom JM, Sisovsky CA (2021) Neglected Achilles tendon ruptures. Clin Podiatr Med Surg 38(2):261–277
Court-Brown CM, Aitken SA, Duckworth AD, Clement ND, McQueen MM (2013) The relationship between social deprivation and the incidence of adult fractures. J Bone Joint Surg Am 95(6):e321–e327
Ganestam A, Kallemose T, Troelsen A, Barfod KW (2015) Increasing incidence of acute Achilles tendon rupture and a noticeable decline in surgical treatment from 1994 to 2013 a nationwide registry study of 33,160 patients. Knee Surg Sports Traumatol Arthrosc 24(12):3730–3737
Hodgkins CW, Wessling NA (2021) Epidemiology of sports-specific foot and ankle injuries. Foot Ankle Clin 26(1):173–185
Hrotko J, Rueda-Sabater E, Lang N, Chin V (2019) Measure Well-Being to Improve It. The 2019 Sustainable Economic Development Assessment. Boston Consulting Group, Boston
Huttunen TT, Kannus P, Rolf C, Fellander-Tsai L, Mattila VM (2014) Acute achilles tendon ruptures: incidence of injury and surgery in Sweden between 2001 and 2012. Am J Sports Med 42(10):2419–2423
Jayanthi NA, Holt DB Jr, LaBella CR, Dugas LR (2018) Socioeconomic factors for sports specialization and injury in youth athletes sports. Health 10(4):303–310
Jenkins PJ, Watts AC, Duckworth AD, McEachan JE (2012) Socioeconomic deprivation and the epidemiology of carpal tunnel syndrome. J Hand Surg Eur 37(2):123–129
Kamphuis CB, van Lenthe FJ, Giskes K, Huisman M, Brug J, Mackenbach JP (2008) Socioeconomic status, environmental and individual factors, and sports participation. Med Sci Sports Exerc 40(1):71–81
Lemme NJ, Li NY, DeFroda SF, Kleiner J, Owens BD (2018) Epidemiology of Achilles tendon ruptures in the united states: athletic and nonathletic injuries from 2012 to 2016. Orthop J Sports Med 6(11):2325967118808238
Maempel JF, Clement ND, Wickramasinghe NR, Duckworth AD, Keating JF (2020) Operative repair of acute Achilles tendon rupture does not give superior patient-reported outcomes to nonoperative management. Bone Joint J 102-B(7):933–940
Maempel JF, White TO, MacKenzie SP, McCann C, Clement ND (2022) The epidemiology of Achilles tendon re-rupture and associated risk factors: male gender, younger age and traditional immobilising rehabilitation are risk factors Knee Surg Sports. Traumatol Arthrosc 30(7):2457–2469
Maffulli N, Waterston SW, Squair J, Reaper J, Douglas AS (1999) Changing incidence of Achilles tendon rupture in Scotland: a 15-year study. Clin J Sport Med 9(3):157–160
National Records of Scotland (NRS) (2021) Mid-Year Population Estimates for Scotland. https://www.nrscotland.gov.uk/statistics-and-data/statistics/statistics-by-theme/population/population-estimates/mid-year-population-estimates.
Noback PC, Jang ES, Cuellar DO, Seetharaman M, Malagoli E, Greisberg JK et al (2017) Risk factors for achilles tendon rupture: a matched case control study. Injury 48(10):2342–2347
Oliver WM, Mackenzie SA, Lenart L, McCann CJ, MacKenzie SP, Duckworth AD et al (2022) Age, personal and family history are independently associated with venous thromboembolism following acute Achilles tendon rupture. Injury 53(2):762–770
Park HG, Youn D, Baik JM, Hwang JH (2021) Epidemiology of Achilles Tendon Rupture in South Korea: Claims Data of the National Health Insurance Service from 2009 to 2017. Clin Orthop Surg 13(4):539–548
Reyes C, Garcia-Gil M, Elorza JM, Mendez-Boo L, Hermosilla E, Javaid MK et al (2015) Socio-economic status and the risk of developing hand, hip or knee osteoarthritis: a region-wide ecological study. Osteoarthritis Cartilage 23(8):1323–1329
Saarensilta IA, Edman G, Ackermann PW (2020) Achilles tendon ruptures during summer show the lowest incidence, but exhibit an increased risk of re-rupture. Knee Surg Sports Traumatol Arthrosc 28(12):3978–3986
Salonen MK, Kajantie E, Osmond C, Forsen T, Yliharsila H, Paile-Hyvarinen M et al (2009) Role of socioeconomic indicators on development of obesity from a life course perspective J Environ. Public Health 2009:625168
Scottish Government (2020) Scottish Index of Multiple Deprivation 16 https://www.webarchive.org.uk/wayback/archive/20200117165925/https://www2.gov.scot/SIMD.
Seeger JD, West WA, Fife D, Noel GJ, Johnson LN, Walker AM (2006) Achilles tendon rupture and its association with fluoroquinolone antibiotics and other potential risk factors in a managed care population. Pharmacoepidemiol Drug Saf 15(11):784–792
Sheth U, Wasserstein D, Jenkinson R, Moineddin R, Kreder H, Jaglal SB (2017) The epidemiology and trends in management of acute achilles tendon ruptures in Ontario, Canada: a population-based study of patients. Bone Joint J 99-B(1):78–86
Steginsky BD, Van DB, Berlet GC (2017) The missed Achilles tear: now what? Foot Ankle Clin 22(4):715–734
Suchak AA, Bostick G, Reid D, Blitz S, Jomha N (2005) The incidence of Achilles tendon ruptures in edmonton. Canada Foot Ankle Int 26(11):932–936
Svedman S, Edman G, Ackermann PW (2020) Deep venous thrombosis after Achilles tendon rupture is associated with poor patient-reported outcome. Knee Surg Sports Traumatol Arthrosc 28(10):3309–3317
Tarantino D, Palermi S, Sirico F, Corrado B (2020) Achilles tendon rupture: mechanisms of injury principles of rehabilitation and return to play. J Funct Morphol Kinesiol 5(4):95
Urwin M, Symmons D, Allison T, Brammah T, Busby H, Roxby M et al (1998) Estimating the burden of musculoskeletal disorders in the community: the comparative prevalence of symptoms at different anatomical sites, and the relation to social deprivation. Ann Rheum Dis 57(11):649–655
Valentin G, Ravn MB, Jensen EK, Friis K, Bhimjiyani A, Ben-Shlomo Y et al (2021) Socio-economic inequalities in fragility fracture incidence: a systematic review and meta-analysis of 61 observational studies. Osteoporos Int 32(12):2433–2448
Varo JJ, Martinez-Gonzalez MA, De Irala-Estevez J, Kearney J, Gibney M, Martinez JA (2003) Distribution and determinants of sedentary lifestyles in the European Union. Int J Epidemiol 32(1):138–146
Westin O, Nilsson HK, Gravare SK, Samuelsson K, Brorsson A, Karlsson J (2018) Patients with an Achilles tendon re-rupture have long-term functional deficits and worse patient-reported outcome than primary ruptures. Knee Surg Sports Traumatol Arthrosc 26(10):3063–3072
Westin O, Sjogren T, Svedman S, Horvath A, Hamrin SE, Samuelsson K et al (2020) Treatment of acute Achilles tendon rupture - a multicentre, non-inferiority analysis BMC. Musculoskelet Disord. https://doi.org/10.1186/s12891-020-03320-3
Funding
None received.
Author information
Authors and Affiliations
Contributions
JM: concept/idea for study, data collection, review and analysis, drafting of manuscript, and editing of manuscript; NDC: guidance with study design, assistance with statistical analysis, and editing of manuscript; SPM: data collection and manuscript editing; CMcC data collection and manuscript editing; TOW: guidance with study design and manuscript editing.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare.
Ethical approval
This study was part of a departmentally approved service review of ATR which was reviewed by the scientific officer for the regional ethics committee (REC) who advised that REC review was not necessary.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix

Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Maempel, J.F., Clement, N.D., Mackenzie, S.P. et al. Socioeconomic deprivation status predicts both the incidence and nature of Achilles tendon rupture. Knee Surg Sports Traumatol Arthrosc 31, 691–700 (2023). https://doi.org/10.1007/s00167-022-07103-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-022-07103-2