
Abstract
Purpose
Age at primary dislocation, recurrence, and glenoid bone loss are associated with development of osteoarthritis (OA). However, an overview of OA following traumatic anterior shoulder instability is lacking and it is unclear to what degree type of surgery is associated with development of OA in comparison to non-operative treatment. The aim of this study was to determine the degree of OA at long-term follow-up after non-operative and operative treatments for patients with anterior shoulder instability. Surgery is indicated when patients experience recurrence and this is associated with OA; therefore, it was hypothesized that shoulders show a higher proportion or degree of OA following operative treatment compared to non-operative treatment.
Methods
A literature search was performed in the PubMed/Medline, EMBASE, and Cochrane databases. Articles reporting the degree of OA that was assessed with the Samilson–Prieto or Buscayret OA classification method after non-operative and operative treatment for anterior shoulder instability with a minimum of 5 years follow-up were included.
Results
Thirty-six articles met the eligibility criteria of which 1 reported the degree of OA for non-operative treatment and 35 reported the degree of OA for 9 different operative procedures. A total of 1832 patients (1854 shoulders) were included. OA proportions of non-operative and operative treatments are similar at any point of follow-up. The Latarjet procedure showed a lower degree of OA compared to non-operative treatment and the other operative procedures, except for the Bristow procedure and Rockwood capsular shift. The meta-analyses showed comparable development of OA over time among the treatment options. An increase in OA proportion was observed when comparing the injured to the contralateral shoulder. However, a difference between the operative subgroups was observed in neither analysis.
Conclusion
Non-operative and operative treatments show similar OA proportions at any point of follow-up. The hypothesis that shoulders showed a higher proportion or degree of OA following operative treatment compared to non-operative treatment is not supported by the data. Operative treatment according to the Latarjet procedure results in a lower degree of OA compared to other treatments, including non-operative treatment.
Level of evidence
IV.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
General risk factors for development of osteoarthritis (OA) include genetic predisposition, female gender, old age, and trauma [5, 32, 49, 50, 60]. OA of the shoulder can be painful, and lead to a decrease in range of motion, limiting shoulder function, which may lead to shoulder arthroplasty as an intervention to treat the pain and reduce the limitations [3, 52]. Studies have shown a higher degree of OA following anterior shoulder dislocation and stabilization surgery compared to the contralateral healthy shoulder [9, 30, 54]. A shoulder dislocation is a commonly established diagnosis at the emergency department, with a reported incidence of 23.9 per 100,000 person-years [30, 67]. The incidence of an anterior shoulder dislocation decreases with age, is higher in males than in females, and is higher when participating in contact and overhead sports in comparison to other types of sports [16]. When the patient experiences (recurrent) instability that affects activities of daily living, work, or sports participation, an operative stabilization procedure is indicated. Several stabilization procedures have been proposed, ranging from soft-tissue procedures to bony augmentation procedures [6]. A soft-tissue procedure, such as the Bankart repair, is usually indicated when little glenoid bone loss is present [15]. A bony augmentation procedure, for example a Latarjet procedure or an Iliac crest bone graft procedure, is usually indicated in case of extensive damage to the glenohumeral joint or excessive glenoid bone loss [51]. Both soft-tissue and bone augmentation procedures can be performed arthroscopically or with an open procedure. Plath et al. showed that an arthroscopic Bankart procedure resulted in similar long-term OA rates compared to an open procedure and non-operative treatment [48]. Age at primary dislocation, recurrence, and glenoid bone loss are associated with development of OA. However, it is unclear to what degree type of surgery is associated with development of OA in comparison to non-operative treatment [23, 25, 26, 28]. In addition, a patient will gain relatively more stability following a bone augmentation procedure in comparison to a soft-tissue procedure. To what degree this is associated with development of OA is unclear as well [7, 36].
To assess the severity of OA following a shoulder dislocation, multiple classification methods have been proposed. Using plain radiography, these methods generally consist of four or five grades of OA severity ranging from “no OA” to “severe OA” [11, 55, 56]. Severity is determined by joint space narrowing and the presence of osteophytes [11, 55, 56]. Long-term degrees of OA for other orthopedic pathologies, such as knee osteoarthritis following an anterior cruciate ligament defect, have been well described [38]. However, it remains unclear if the treatment type for anterior shoulder instability influences degree of OA [46]. If the degree of OA is influenced by treatment type in any way, it can assist both clinicians and patients in the decision-making process.
The aim of this study was to determine the degree of OA at long-term follow-up after non-operative and operative treatment for patients with anterior shoulder instability. Surgery is indicated when patients experience recurrence and this is associated with OA; therefore, it was hypothesized that shoulders show a higher proportion or degree of OA following operative treatment compared to non-operative treatment.
Materials and methods
This systematic review focused on glenohumeral OA after non-operative and operative treatment for anterior shoulder instability. The guideline and algorithm of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) were used [40]. The review was registered in PROSPERO (https://www.crd.york.ac.uk/prospero/; registration number CRD42020141008).
Literature search and study selection
A literature search was performed in the PubMed/Medline, EMBASE, and Cochrane databases on the 22nd of July 2019. The search was performed with the assistance of a clinical librarian and was not limited to year of publication. The search terms are listed in the appendix. Articles written in the English, Dutch, German, or French language were included. Titles and abstracts were screened by two authors (LV and EP). Studies that met the inclusion criteria underwent full-text screening by the same authors. Any disagreement was resolved by discussion and consensus.
Inclusion and exclusion criteria
Articles that reported degree of OA after non-operative or operative treatments for anterior shoulder instability with a minimum of 5 years follow-up were included. Controlled trials and prospective or retrospective cohort studies were included. Studies that used classification systems other than Samilson–Prieto or its modified version by Buscayret were excluded. Furthermore, studies that did not use plain radiograph to assess OA with these classifications were excluded. Studies that did not report original data, animal studies, and cadaveric studies were excluded. When the same patient group was used, the article with the longest follow-up was included for analysis.
Methodological quality assessment
The quality of the studies was assessed by the methodological index for non-randomized studies (MINORS) [59]. By scoring 0 (not reported), 1 (reported but inadequate), or 2 (reported and adequate) at each item, studies could get a total score of 16 for non-comparative studies and 24 for comparative studies. Any disagreement was resolved by discussion and consensus.
Data extraction
The extracted primary outcome measure was degree of OA according to both the Samilson-Prieto and Buscayret OA classification after non-operative or operative treatment for anterior shoulder instability. If the authors had assessed classification of OA on multiple radiographic views, a weighted average score of the different views was calculated. Furthermore, secondary outcome measures were extracted including type of surgery, gender, functional outcome (Rowe score), recurrent dislocation, age at surgery, and length of follow-up. The data were extracted by the lead author (LV). A random sample of ten articles was independently assessed by the second author (EP) and checked for accuracy.
OA classification
The Samilson–Prieto classification is a radiographical classification system which categorizes OA in 4 categories comprising (0) no OA, (I) osteophytes measuring < 3 mm in greatest distance diameter, (II) osteophytes measuring between 3 and 7 mm in greatest distance diameter and slight glenohumeral joint irregularity, and (III) osteophytes measuring > 7 mm in greatest distance diameter, narrowing of the glenohumeral joint and sclerosis (Fig. 1). For the modified version, Buscayret added one extra category by splitting the category III of the original version into the categories (III) osteophytes measuring > 7 mm in greatest distance diameter, narrowing of the glenohumeral joint and sclerosis, and (IV) complete obliteration of the glenohumeral joint with or without osteophytes. For the purpose of pooling, these two categories were merged again [11, 56]. Furthermore, if authors reported that some of their patients received arthroplasty treatment of the shoulder or that the shoulder showed complete glenoid erosion, they were considered to be grade III.

Osteoarthritis (OA) following a Bankart repair with > 10 years follow-up. This figure demonstrates an example of OA in the shoulder. The shoulder has been classified as Samilson–Prieto grade II
Statistical analysis
To perform meta-analyses, data of the primary outcome were pooled. For calculation of pooled proportions and Relative Risks (RR) of OA, the Samilson–Prieto classification was dichotomized by merging all categories describing signs of OA (categories I, II, and III) as OA. Category 0 was considered as no OA. Patient characteristics and follow-up were pooled by calculation of weighted means and pooled standard deviations (SD). If the standard deviation was not reported, it was estimated with the range and the sample size according to Walter et al. [64]. Furthermore, if the mean was not reported, it was estimated using the median, range, and sample size according to Hozo et al. [31]. Comparisons of the degree of OA were performed by the use of Mann–Whitney U tests; proportions were compared by the use of Chi squared tests. Review Manager version 5.3 (the Nordic Cochrane Center, Copenhagen, Denmark) was used to calculate RR with 95% CI. Heterogeneity between studies was assessed by the use of X2 and I2 statistic. I2 > 50% was considered as substantial heterogeneity [24]. IBM SPSS Statistics 25 (IBM Corp., Armonk, NY) was used to perform other statistical analyses.
Results
Screening and study characteristics
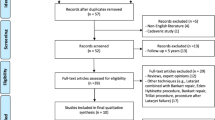
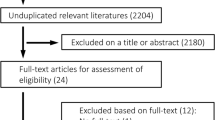
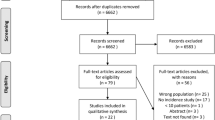
The literature search resulted in 3529 articles for title and abstract screening after deduplication (Fig. 2). The full-text analysis was performed on 200 articles after title and abstract screening, resulting in 36 articles for inclusion in the analysis. Reasons for exclusion are listed in Fig. 2. In the included studies, a total of 1832 patients (1854 shoulders) were included. The sample size ranged from 9 to 161 shoulders. The follow-up ranged from 5 to 57 years. The included studies were published between 1994 and 2019. The included studies reported degree of OA for 1 type of non-operative treatment, which included 161 shoulders for conservative treatment (Tables 1, 2) [28]. Furthermore, the included studies reported degree of OA for 9 types of operative treatment, which included a total sample of 663 shoulders for the Bankart repair [4, 12, 13, 19, 20, 30, 34, 41, 44, 47, 48, 63, 69], 515 shoulders for the Latarjet procedure [8, 14, 22, 29, 30, 37, 39, 45, 58, 65], 220 shoulders for the Eden–Hybinette procedure [9, 35, 53, 54, 66], 112 shoulders for the Putti-Platt procedure [35, 62, 68], 75 shoulders for the Iliac crest bone graft procedure [42, 61], 11 shoulders for the Bristow procedure [57], 45 shoulders for the Du Toit procedure [70], 25 shoulders for Weber’s rotational osteotomy [18], and 27 shoulders for the Rockwood capsular shift (Tables 1, 2) [43]. The MINORS quality assessment ranged from 4 to 11 (median 8; IQR 8–9) of the 16 points for non-comparative studies (Table 1). The comparative studies scored 16 of the 24 points. The mean Rowe score ranged from 80.0 to 95.0 and the percentage of recurrent dislocation ranged from 0 to 41% (Table 1). Because of the small differences in quality scores between the studies, no weighing of the outcomes was applied in the analyses.

Flow diagram
Comparison of OA among non-operative and operative treatment options
OA proportion was calculated by merging all categories describing signs of OA (categories I, II, and III) as OA. Non-operative and operative treatments show similar OA proportions at any point of follow-up (Fig. 3). The Latarjet procedure seems to show a slightly lower proportion of OA compared to other treatment options.

Percentage of osteoarthritis after operative or non-operative treatments. This figure shows the percentage of osteoarthritis for each individual procedure (n = 39) of the included studies (n = 36). Three studies reported long-term follow-up of two procedures; these studies are shown twice in this figure. The color of the circle matches a procedure that can be found in the legend. The size of the circle is dependent on sample size and increases in size with a larger sample size. OA proportion was calculated by merging all categories describing signs of OA (categories I, II, and III) as OA. OA = Osteoarthritis
Comparison of the degree of OA according to the Samilson–Prieto scale among treatment modalities revealed that the Latarjet procedure shows a significantly lower degree of OA compared to the Bankart repair (P < 0.001), the Eden–Hybinette procedure (P < 0.001), the Putti–Platt procedure (P < 0.001), the Iliac crest procedure (P < 0.001), the Du Toit procedure (P = 0.001), the Weber’s rotational osteotomy (P < 0.001), and conservative treatment (P < 0.001; Table 2). There was no statistically significant difference between the Latarjet procedure and the Bristow (n.s.) and the Latarjet procedure and the Rockwood capsular shift procedure (n.s.; Table 2). Degree of OA following arthroscopic surgery was only reported for the Bankart repair. Seven studies reported degree of OA following arthroscopic surgery, six studies following open surgery, and one study compared both surgery techniques. A significant difference in degree of OA between an open or arthroscopic Bankart repair was not observed (n.s., Table 1).
Proportion of OA preoperatively and at follow-up
Eight studies reported consistent data for degree of OA preoperatively and at follow-up following treatment. Overall, a higher proportion of OA post-operative compared to pre-operative was observed for the Bankart repair and the Latarjet groups, but not for the iliac crest group (Fig. 4). The likelihood of developing OA was not statistically significantly different between the treatment groups Bankart, Latarjet, and Iliac crest (n.s.; Fig. 4).

Meta-analysis of preoperative vs follow-up for proportion of osteoarthritis (OA). This meta-analysis shows the ratio of the studies (n = 8) that reported degree of OA preoperatively and at follow-up. The proportion of OA was calculated to perform the meta-analysis. Furthermore, the difference between the subgroups is determined. OA proportion was calculated by merging all categories describing signs of OA (categories I, II, and III)
Proportion of OA of the injured versus contralateral shoulder
Seven studies reported consistent data for degree of OA for both the injured and contralateral (healthy) shoulder. Overall, a higher proportion of OA for the injured shoulder compared to the contralateral shoulder was observed for the Bankart repair, the Latarjet, Eden–Hybinette, and iliac crest groups, but not for the Rockwood capsular shift (Fig. 5). There was no statistically significant difference in proportion of OA between the subgroups Eden–Hybinette, Bankart, Latarjet, Rockwood capsular shift, and Iliac crest (n.s.; Fig. 5).

Meta-analysis of injured vs contralateral shoulder for proportion of osteoarthritis (OA). This meta-analysis shows the ratio of the studies (n = 7) that reported the degree of OA for the injured and contralateral shoulder for a procedure. The proportion of OA was calculated to perform the meta-analysis. Furthermore, the difference between the subgroups is determined. OA proportion was calculated by merging all categories describing signs of OA (categories I, II, and III)
Discussion
The most important finding of the present study was that proportion of OA seems comparable between the various treatments and may be unrelated to treatment type with a follow-up ranging from 5 to 35 years. However, the analyses of the data revealed a statistically significant lower degree of OA after the Latarjet procedure compared to other treatment types at follow-up, except the Bristow procedure and Rockwood capsular shift. A difference in degree of OA between an open or arthroscopic Bankart repair was also not observed. In addition, the meta-analyses showed that the likelihood of developing OA after a Bankart and Latarjet was similar and an overall increase in proportion of OA was observed for the injured shoulder compared to the contralateral shoulder for the Bankart repair, the Latarjet, Eden–Hybinette, and iliac crest groups, but not for the Rockwood capsular shift. However, a difference between the operative subgroups was not observed for both analyses.
Giving a prospect regarding development of OA after a shoulder dislocation might be challenging for professionals at the outpatient clinic. Besides from the general risk factors for development of OA, professionals are confronted with the multiple treatment options. Bony augmentation procedures, such as the Latarjet or Iliac crest bone graft procedure, are usually indicated when more glenoid bone loss is present [51]. Excessive glenoid bone loss is often the result of multiple dislocations and this is associated with development of OA [25, 26, 28]. One of the factors that might explain the association between multiple dislocations and development of OA is changes in morphology of the glenoid as a result of multiple dislocations [23]. However, based on the data of this systematic review, these types of surgeries, which are used to treat excessive glenoid bone loss, do not seem to contribute to a higher proportion of OA. The Latarjet procedure even showed a lower proportion and degree of OA compared to the other treatment types. As the development of OA is associated with multiple dislocations, recurrent dislocation after operation may contribute to a higher degree of OA at follow-up. Both the Latarjet procedure and the Iliac crest bone graft procedure have low recurrence rates, showing a weighted recurrence rate of 2% and 3% respectively. The bony augmentation procedures may offer more stability compared to other procedures, which could prevent micro instability and development of OA in the long term [7, 36]. However, the Bankart repair, showing a wide range of 14% to 86% OA, may have a wider indication range compared to the bony augmentation procedures.
The difference in pooled proportion of OA between the Latarjet procedure and the Iliac crest bone graft procedure is remarkable with values of 34% and 61%, respectively. Since both procedures use a bone graft to stabilize the shoulder, this difference could be based on coincidence [21, 42, 61]. The sample sizes of the iliac crest studies are smaller, and two of the ten studies showed proportions of 65% and 71% for the Latarjet procedure, as well. Furthermore, the meta-analyses did not show a difference between proportions OA of preoperative and follow-up data or proportions of OA for the injured compared to the contralateral shoulder for the Latarjet procedure compared to other procedures. However, at follow-up, the degree of OA seems lower following the Latarjet procedure. An explanation might be that the Latarjet studies started with lower degrees of pre-operative OA.
OA can be classified through multiple classification methods of which the Samilson–Prieto method is most commonly used [11, 55, 56]. These methods determine severity, which is generally based on the presence of osteophytes, joint space irregularity, and joint space narrowing. The reliability of the Samilson–Prieto classification, which is the most commonly used method, is generally good [10, 17]. As the Samilson–Prieto classification is based on the presence and size of osteophytes on the inferior glenoid, Ilg et al. question if damage to the inferior part of the glenoid, such as glenoid bone loss, may lead to a higher classification [33]. Both Ilg et al. and Hovelius et al. stated that the Samilson–Prieto classification alone might not be enough to reliably determine OA [27, 33]. Furthermore, it is unclear whether the type of surgical procedure influences the Samilson–Prieto classification. A bone augmentation procedure adds a bone block to the inferior part of the glenoid, which may result in a different classification as well. For example, the Iliac crest bone graft procedure had many patients classified as grade I with the Samilson–Prieto classification. The difference between grade 0 and grade I may illustrate that it can be difficult to assess OA with a bone graft that is attached to the inferior part of the glenoid [2].
There were some limitations to this systematic review. The included studies are primarily of low level of evidence with mediocre scores in the MINORS quality assessment. Most of these studies were performed with a retrospective design. The length of follow-up varies widely, posing a challenge with regard to drawing firm conclusions. However, a strength of this systematic review includes a systematic search and selection process according to the PRISMA guidelines. Furthermore, a large amount of data and sufficient studies made a quantitative meta-analysis feasible.
Many uncertainties remain regarding degree of OA following an anterior shoulder dislocation. The presented data show that the type of operative procedure may have little effect on the development of OA and that a Latarjet procedure may even show a lower degree of OA compared to other treatment options. Future studies should focus on shoulder stability as a factor in developing OA [36]. There appear to be little changes in proportion of OA between 5 and 35 years of follow-up. Studies with short- to mid-term follow-up of 10 years might be valuable in identifying patients that are prone to developing OA in an early stage. Finally, few studies exist that consider surgical options that reduce instability by treating a Hill–Sachs lesion, such as a remplissage in addition to the Bankart repair [1]. The only study that was found in this systematic review that treated a Hill–Sachs lesion was Weber’s rotational osteotomy. These treatment options are underexposed and they require long-term studies to determine the proportion and degree of OA, as well.
Conclusions
Non-operative and operative treatments show similar OA proportions at any point of follow-up. The hypothesis that shoulders showed a higher proportion or degree of OA following operative treatment compared to non-operative treatment is not supported by the data. Operative treatment according to the Latarjet procedure results in a lower degree of OA compared to other treatments, including non-operative treatment.
Abbreviations
- OA:
-
Osteoarthritis
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- MINORS:
-
Methodological index for non-randomized studies
References
Alkaduhimi H, Verweij LPE, Willigenburg NW, van Deurzen DFP, van den Bekerom MPJ (2019) Remplissage with bankart repair in anterior shoulder instability: a systematic review of the clinical and cadaveric literature. Arthroscopy 35:1257–1266
Allain J, Goutallier D, Glorion C (1998) Long-term results of the Latarjet procedure for the treatment of anterior instability of the shoulder. J Bone Joint Surg Am 80:841–852
Baumgarten KM, Chang PS, Dannenbring TM, Foley EK (2018) Does total shoulder arthroplasty improve patients’ activity levels? J Shoulder Elbow Surg 27:1987–1995
Berendes T, Mathijssen N, Verburg H, Kraan G (2018) The open-modified Bankart procedure: long-term follow-up ‘a 16-26-year follow-up study’. Arch Orthop Trauma Surg 138:597–603
Blagojevic M, Jinks C, Jeffery A, Jordan KP (2010) Risk factors for onset of osteoarthritis of the knee in older adults: a systematic review and meta-analysis. Osteoarthritis Cartilage 18:24–33
Blonna D, Bellato E, Caranzano F, Assom M, Rossi R, Castoldi F (2016) Arthroscopic bankart repair versus open bristow-latarjet for shoulder instability: a matched-pair multicenter study focused on return to sport. Am J Sports Med 44:3198–3205
Bolia I, Chahla J, Locks R, Briggs K, Philippon MJ (2016) Microinstability of the hip: a previously unrecognized pathology. Muscles Ligaments Tendons J 6:354–360
Bouju Y, Gadea F, Stanovici J, Moubarak H, Favard L (2014) Shoulder stabilization by modified Latarjet-Patte procedure: results at a minimum 10 years’ follow-up, and role in the prevention of osteoarthritis. Orthop Traumatol Surg Res 100:S213–218
Brox JI, Finnanger AM, Merckoll E, Lereim P (2003) Satisfactory long-term results after Eden-Hybbinette-Alvik operation for recurrent anterior dislocation of the shoulder: 6-20 years’ follow-up of 52 patients. Acta Orthop Scand 74:180–185
Brox JI, Lereim P, Merckoll E, Finnanger AM (2003) Radiographic classification of glenohumeral arthrosis. Acta Orthop Scand 74:186–189
Buscayret F, Edwards TB, Szabo I, Adeleine P, Coudane H, Walch G (2004) Glenohumeral arthrosis in anterior instability before and after surgical treatment - Incidence and contributing factors. Am J Sports Med 32:1165–1172
Castagna A, Markopoulos N, Conti M, Delle Rose G, Papadakou E, Garofalo R (2010) Arthroscopic bankart suture-anchor repair: radiological and clinical outcome at minimum 10 years of follow-up. Am J Sports Med 38:2012–2016
Chapus V, Rochcongar G, Pineau V, Salle de Chou E, Hulet C (2015) Ten-year follow-up of acute arthroscopic Bankart repair for initial anterior shoulder dislocation in young patients. Orthop Traumatol Surg Res 101:889–893
de l’Escalopier N, Barbier O, Demoures T, Ollat D, Versier G (2018) Long-term results of a monocentric series of soldiers after latarjet procedure for anterior shoulder instability. implications for the assessment of soldiers’ medical ability. Mil Med 183:e134–e137
DeFroda S, Bokshan S, Stern E, Sullivan K, Owens BD (2017) Arthroscopic bankart repair for the management of anterior shoulder instability: indications and outcomes. Curr Rev Musculoskelet Med 10:442–451
DeFroda SF, Donnelly JC, Mulcahey MK, Perez L, Owens BD (2019) Shoulder instability in women compared with men: epidemiology, pathophysiology, and special considerations. JBJS Rev 7:e10
Elsharkawi M, Cakir B, Reichel H, Kappe T (2013) Reliability of radiologic glenohumeral osteoarthritis classifications. J Shoulder Elbow Surg 22:1063–1067
Flury MP, Goldhahn J, Holzmann P, Simmen BR (2007) Does Weber’s rotation osteotomy induce degenerative joint disease at the shoulder in the long term? J Shoulder Elbow Surg 16:735–741
Franceschi F, Papalia R, Del Buono A, Vasta S, Maffulli N, Denaro V (2011) Glenohumeral osteoarthritis after arthroscopic Bankart repair for anterior instability. Am J Sports Med 39:1653–1659
Gamulin A, Dayer R, Lubbeke A, Miozzari H, Hoffmeyer P (2014) Primary open anterior shoulder stabilization: a long-term, retrospective cohort study on the impact of subscapularis muscle alterations on recurrence. BMC Musculoskelet Disord 15:45
Giles JW, Degen RM, Johnson JA, Athwal GS (2014) The Bristow and Latarjet procedures: why these techniques should not be considered synonymous. J Bone Joint Surg Am 96:1340–1348
Gordins V, Hovelius L, Sandstrom B, Rahme H, Bergstrom U (2015) Risk of arthropathy after the Bristow-Latarjet repair: a radiologic and clinical thirty-three to thirty-five years of follow-up of thirty-one shoulders. J Shoulder Elbow Surg 24:691–699
Haas M, Plachel F, Wierer G, Heuberer P, Hoffelner T, Schulz E et al (2019) Glenoid morphology is associated with the development of instability arthropathy. J Shoulder Elbow Surg 28:893–899
Higgins JP, Thompson SG (2002) Quantifying heterogeneity in a meta-analysis. Stat Med 21:1539–1558
Hovelius L, Augustini BG, Fredin H, Johansson O, Norlin R, Thorling J (1996) Primary anterior dislocation of the shoulder in young patients. A ten-year prospective study. J Bone Joint Surg Am 78:1677–1684
Hovelius L, Rahme H (2016) Primary anterior dislocation of the shoulder: long-term prognosis at the age of 40 years or younger. Knee Surg Sports Traumatol Arthrosc 24:330–342
Hovelius L, Saeboe M (2008) Documentation of dislocation arthropathy of the shoulder “area index”: a better method to objectify the humeral osteophyte? J Shoulder Elbow Surg 17:197–201
Hovelius L, Saeboe M (2009) Neer Award 2008: arthropathy after primary anterior shoulder dislocation–223 shoulders prospectively followed up for twenty-five years. J Shoulder Elbow Surg 18:339–347
Hovelius L, Sandstrom B, Saebo M (2006) One hundred eighteen Bristow-Latarjet repairs for recurrent anterior dislocation of the shoulder prospectively followed for fifteen years: study II-the evolution of dislocation arthropathy. J Shoulder Elbow Surg 15:279–289
Hovelius LK, Sandstrom BC, Rosmark DL, Saebo M, Sundgren KH, Malmqvist BG (2001) Long-term results with the Bankart and Bristow-Latarjet procedures: recurrent shoulder instability and arthropathy. J Shoulder Elbow Surg 10:445–452
Hozo SP, Djulbegovic B, Hozo I (2005) Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol 5:13
Iidaka T, Muraki S, Oka H, Horii C, Kawaguchi H, Nakamura K et al (2020) Incidence rate and risk factors for radiographic hip osteoarthritis in Japanese men and women: a 10-year follow-up of the ROAD study. Osteoarthr Cartil 28:182–188
Ilg A, Bankes MJ, Emery RJ (2001) The intra- and inter-observer reliability of the Samilson and Prieto grading system of glenohumeral arthropathy. Knee Surg Sports Traumatol Arthrosc 9:187–190
Kavaja L, Pajarinen J, Sinisaari I, Savolainen V, Bjorkenheim JM, Haapamaki V et al (2012) Arthrosis of glenohumeral joint after arthroscopic Bankart repair: a long-term follow-up of 13 years. J Shoulder Elbow Surg 21:350–355
Konig DP, Rutt J, Treml O, Hackenbroch MH (1997) Osteoarthritis and recurrences after Putti-Platt and Eden-Hybbinette operations for recurrent dislocation of the shoulder. Int Orthop 21:72–76
Ladermann A, Denard PJ, Tirefort J, Kolo FC, Chague S, Cunningham G et al (2016) Does surgery for instability of the shoulder truly stabilize the glenohumeral joint?: a prospective comparative cohort study. Medicine (Baltimore) 95:e4369
Ladermann A, Lubbeke A, Stern R, Cunningham G, Bellotti V, Gazielly DF (2013) Risk factors for dislocation arthropathy after Latarjet procedure: a long-term study. Int Orthop 37:1093–1098
Lie MM, Risberg MA, Storheim K, Engebretsen L, Oiestad BE (2019) What’s the rate of knee osteoarthritis 10 years after anterior cruciate ligament injury? An updated systematic review. Br J Sports Med 53:1162–1167
Mizuno N, Denard PJ, Raiss P, Melis B, Walch G (2014) Long-term results of the Latarjet procedure for anterior instability of the shoulder. J Shoulder Elbow Surg 23:1691–1699
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6:e1000097
Moroder P, Odorizzi M, Pizzinini S, Demetz E, Resch H, Moroder P (2015) Open bankart repair for the treatment of anterior shoulder instability without substantial osseous glenoid defects: results after a minimum follow-up of twenty years. J Bone Joint Surg Am 97:1398–1405
Moroder P, Plachel F, Becker J, Schulz E, Abdic S, Haas M et al (2018) Clinical and radiological long-term results after implant-free, autologous, iliac crest bone graft procedure for the treatment of anterior shoulder instability. Am J Sports Med 46:2975–2980
Murena L, Guindani N, Turino S, Grassi FA, Cherubino P (2016) Long-term outcome of Rockwood capsular shift for recurrent shoulder dislocation. J Orthop Surg (Hong Kong) 24:392–397
Neviaser RJ, Benke MT, Neviaser AS (2017) Mid-term to long-term outcome of the open Bankart repair for recurrent traumatic anterior dislocation of the shoulder. J Shoulder Elbow Surg 26:1943–1947
Neyton L, Young A, Dawidziak B, Visona E, Hager JP, Fournier Y et al (2012) Surgical treatment of anterior instability in rugby union players: clinical and radiographic results of the Latarjet-Patte procedure with minimum 5-year follow-up. J Shoulder Elbow Surg 21:1721–1727
Papalia R, Osti L, Del Buono A, Denaro V, Maffulli N (2010) Glenohumeral arthropathy following stabilization for recurrent instability. Br Med Bull 96:75–92
Pelet S, Jolles BM, Farron A (2006) Bankart repair for recurrent anterior glenohumeral instability: results at twenty-nine years’ follow-up. J Shoulder Elbow Surg 15:203–207
Plath JE, Aboalata M, Seppel G, Juretzko J, Waldt S, Vogt S et al (2015) Prevalence of and risk factors for dislocation arthropathy: radiological long-term outcome of arthroscopic bankart repair in 100 shoulders at an average 13-year follow-up. Am J Sports Med 43:1084–1090
Poulsen E, Goncalves GH, Bricca A, Roos EM, Thorlund JB, Juhl CB (2019) Knee osteoarthritis risk is increased 4-6 fold after knee injury - a systematic review and meta-analysis. Br J Sports Med 53:1454–1463
Prieto-Alhambra D, Judge A, Javaid MK, Cooper C, Diez-Perez A, Arden NK (2014) Incidence and risk factors for clinically diagnosed knee, hip and hand osteoarthritis: influences of age, gender and osteoarthritis affecting other joints. Ann Rheum Dis 73:1659–1664
Provencher MT, Bhatia S, Ghodadra NS, Grumet RC, Bach BR Jr, Dewing CB et al (2010) Recurrent shoulder instability: current concepts for evaluation and management of glenoid bone loss. J Bone Joint Surg Am 92(Suppl 2):133–151
Puskas B, Harreld K, Clark R, Downes K, Virani NA, Frankle M (2013) Isometric strength, range of motion, and impairment before and after total and reverse shoulder arthroplasty. J Shoulder Elbow Surg 22:869–876
Rachbauer F, Ogon M, Wimmer C, Sterzinger W, Huter B (2000) Glenohumeral osteoarthrosis after the Eden-Hybbinette procedure. Clin Orthop Relat Res 373:135–140
Rahme H, Wikblad L, Nowak J, Larsson S (2003) Long-term clinical and radiologic results after Eden-Hybbinette operation for anterior instability of the shoulder. J Shoulder Elbow Surg 12:15–19
Rosenberg BN, Richmond JC, Levine WN (1995) Long-term followup of Bankart reconstruction. Incidence of late degenerative glenohumeral arthrosis. Am J Sports Med 23:538–544
Samilson RL, Prieto V (1983) Dislocation arthropathy of the shoulder. J Bone Joint Surg Am 65:456–460
Schroder DI, Provencher MT, Mologne TS, Muldoon MP, Cox JS (2006) The modified Bristow procedure for anterior shoulder instability - 26-year outcomes in naval academy midshipmen. Am J Sports Med 34:778–786
Singer GC, Kirkland PM, Emery RJ (1995) Coracoid transposition for recurrent anterior instability of the shoulder. A 20-year follow-up study. J Bone Joint Surg Br 77:73–76
Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J (2003) Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg 73:712–716
Snoeker B, Turkiewicz A, Magnusson K, Frobell R, Yu D, Peat G et al (2020) Risk of knee osteoarthritis after different types of knee injuries in young adults: a population-based cohort study. Br J Sports Med 54:725–730
Steffen V, Hertel R (2013) Rim reconstruction with autogenous iliac crest for anterior glenoid deficiency: forty-three instability cases followed for 5-19 years. J Shoulder Elbow Surg 22:550–559
van der Zwaag HM, Brand R, Obermann WR, Rozing PM (1999) Glenohumeral osteoarthrosis after Putti-Platt repair. J Shoulder Elbow Surg 8:252–258
van Gastel ML, Willigenburg NW, Dijksman LM, Lindeboom R, van den Bekerom MPJ, van der Hulst VPM et al (2019) Ten percent re-dislocation rate 13 years after the arthroscopic Bankart procedure. Knee Surg Sports Traumatol Arthrosc 27:3929–3936
Walter SD, Yao X (2007) Effect sizes can be calculated for studies reporting ranges for outcome variables in systematic reviews. J Clin Epidemiol 60:849–852
Wei-Yu Shih K-CC, Hung Sheng-Tsai, Lee Hung-Maan, Shih Jui-Tien (2012) Clinical results of shoulder arthroscopy combined with an open modified Latarjet procedure for chronic anterior shoulder instability with glenoid bony loss. Formos J Musculoskelet Disord 3:126–131
Wildner M, Wimmer B, Reichelt A (1994) Osteoarthritis after the Eden-Hybbinette-Lange procedure for anterior dislocation of the shoulder. A 15 year follow up. Int Orthop 18:280–283
Zacchilli MA, Owens BD (2010) Epidemiology of shoulder dislocations presenting to emergency departments in the United States. J Bone Joint Surg Am 92:542–549
Zaffagnini S, Marcacci M, Loreti I, Visani A, Vascellari A (2000) Results of the original Putti-Platt procedure for shoulder instability: review of Putti’s scholar experience. Knee Surg Sports Traumatol Arthrosc 8:314–319
Zaffagnini S, Marcheggiani Muccioli GM, Giordano G, Bonanzinga T, Grassi A, Nitri M et al (2012) Long-term outcomes after repair of recurrent post-traumatic anterior shoulder instability: comparison of arthroscopic transglenoid suture and open Bankart reconstruction. Knee Surg Sports Traumatol Arthrosc 20:816–821
Zaffagnini S, Russo A, Reggiani LM, Iacono F, Filardo G, Delcogliano M et al (2007) Revisiting open capsuloplasty for the treatment of anterior shoulder instability: 35-year follow-up of the Du Toit procedure. Knee Surg Sports Traumatol Arthrosc 15:1055–1061
Acknowledgements
We would like to thank our clinical librarian F.S. van Etten–Jamaludin for helping us with the search.
Funding
There was no funding for this project
Author information
Authors and Affiliations
Contributions
Lukas P.E. Verweij: Lead authordesign, data acquisition, data analysis, data interpretation, and writing. Erik C. Pruijssen: Data acquisition. Gino M.M.J. Kerkhoffs: Designdata interpretation, and writing. Leendert Blankevoort: Design, data analysis, data interpretation, and writing. Inger N. Siervelt: Data analysisdata interpretation, and writing. Derek F.P. van Deurzen: Designdata interpretation, and writing. Michel P.J. van den Bekerom: Designdata interpretation, and writing.
Corresponding author
Ethics declarations
Conflict of interest
The authors report no conflict of interest.
Ethical statement
All authors comply with Springer's ethical policies.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Verweij, L.P.E., Pruijssen, E.C., Kerkhoffs, G.M.M.J. et al. Treatment type may influence degree of post-dislocation shoulder osteoarthritis: a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc 29, 2312–2324 (2021). https://doi.org/10.1007/s00167-020-06263-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-020-06263-3