
Abstract
Purpose
To investigate the prevalence of cam morphology in (1) a group of young elite Mogul and Alpine skiers compared with non-athletes and (2) between the sexes.
Method
The hip joints of 87 subjects [n = 61 young elite skiers (29 females and 32 males) and n = 26 non-athletes (17 females and 9 males)] were examined using MRI, for measurements of the presence of cam morphology (α-angle ≥ 55).
Results
The skiers had a significantly higher prevalence of cam morphology compared with the non-athletes (49% vs 19%, p = 0.009). A significant difference (p < 0.001) was also found between females and males, where 22% of the females and 61% of the males had cam morphology. Among the skiers, there was also a significant difference (p < 0.001) between the sexes, where 28% of the females and 68% of the males had cam morphology. This difference between the sexes was not found in the non-athletic group. No significant differences were found between Mogul and Alpine skiers.
Conclusion
Young male elite skiers have a higher prevalence of cam morphology of the hips compared with non-athletes.
Level of evidence
II.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Femoro-acetabular impingement syndrome (FAIS) is defined as a combination of symptoms, clinical signs and imaging findings of the hip [15, 26, 44]. The abnormal imaging findings can be either femoral based (cam) or acetabular based (pincer) [8, 12, 19, 28]. These two pathologies may occur isolated or in combination [8]. Cam-type FAIS is a condition where the abnormally formed femoral head–neck junction collides with the acetabular margin during flexion and internal rotation of the hip joint (Figs. 1, 2). A measure that quantifies cam morphology is the α-angle; the larger the α-angle, the larger is the cam morphology, and in previous studies a threshold of > 55° has been considered clinically relevant [6, 29, 38, 39] (Fig. 3). The collision in the hip joint may lead to pain, cartilage injuries of the acetabulum and less frequently to tears of the acetabular labrum [8, 10, 12, 19, 27]. Cam-type FAIS is considered to increase the risk for early osteoarthritis (OA) in the hip joint, while pincer-type FAIS is considered to cause a higher prevalence of labral injuries rather than hip OA [2, 4, 5, 25, 34, 43].

Hip joint with normal morphology of the head–neck junction

MRI examination of a male skier showing cam morphology with an α-angle above > 55° (arrow)

The α-angle is used to define the presence of cam morphology and, in this study, a threshold of > 55° has been considered relevant
Several studies have shown a higher prevalence of cam morphology to occur in young athletes, in different sports such as soccer, track and field, ice hockey and basketball, and therefore it is hypothesized that the morphology of cam is acquired in relation to vigorous sporting activity during growth [1, 3, 9, 23, 37,38,39, 42]. Tak et al. [42] found a significant dose–response relationship between the frequency of football practice during skeletal growth and the development of a cam morphology, fortifying the relationship between high-load sporting activity during growth and the development of cam. Agricola et al. [3] showed that young male soccer players gradually develop cam morphology during growth, but after growth plate closure there is no significant increase in the prevalence of cam. Genetics may also play a role in the development of cam, where siblings to patients with cam morphology are at a higher risk of developing the same hip morphology [30]. Furthermore, previous studies have shown that cam morphology is more prevalent among males than females [11].
Skiing, both Mogul and Alpine, is a sport that exposes the hip to great forces (high speed and G-forces) in a vulnerable position [18, 22, 41]. There is a constant shift in hip (and knee) flexion from extended to almost maximally flexed during a ski run, which is often on hard and uneven snow. In the Mogul run, there are two acrobatic jumps included, both with high impact on landing.
The hypothesis of this study was that young elite skiers have a higher prevalence of cam morphology compared with a control group of non-athletes, and that cam morphology is more prevalent among male skiers compared to female skiers.
Materials and methods
Study population
Seventy-six elite Alpine and Mogul skiers, between 16 and 20 years of age, attending Åre Ski Academy were invited to participate in this prospective study.
To recruit non-athletes, two of the authors visited several high schools and presented the project orally in class. Written information was also distributed. The invited non-athletes were all first-year high school pupils and lived in the same area as the skiers. The criteria defining the non-athletes was that they did not currently nor in the recent past participate in training activities more than two times per week.
Seventy-five skiers and 27 non-athletes agreed to participate in the study.
The exclusion criteria for both groups were previously diagnosed hip, spine or pelvic diseases, anomalies and previous surgery to the hips, spine or pelvis (Fig. 4).

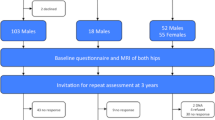
Prisma diagram presenting the participants enrolled in the present study and the MRI results concerning the presence of cam morphology among them
Participation was completely voluntary and the participants could withdraw at any time. Written consent was given by all individuals, and for participants younger than 18 years, written consent was also obtained from their parents.
The present study was approved by the Regional Ethical Review Board at the Sahlgrenska Academy, Gothenburg University, Gothenburg, Sweden (ID number: 692-13).
MRI examination
All subjects underwent MRI of both hips without contrast. The MRI that was used was a GE Optima 450 Wide 1.5T (GE Healthcare Bio-Sciences Corp, Piscataway, NJ, USA), at Östersund Hospital, Sweden. Cor T2 Fat Sat and Ax 3D Cube sequences were obtained, angled to the femoral neck using a coil surface of HD 8 Channel Cardiac Array (GE Healthcare Bio-Sciences Corp).
Evaluation of the MRI images included two parts. First, the status of the growth plate was evaluated as being either closed or open, based on the appearance of the capital femoral growth plate on MRI using the same method as Siebenrock et al. [38]. Second, the α-angle was measured. Seven measurements, from 9 o’clock to 3 o’clock (180°), to determine the morphological features of the femoral head–neck junction were performed [19]. Measurement of the α-angle was performed according to Nötzli et al. [27]. The α-angle was measured between the femoral neck axis and a line from the centre of the femoral head to a point where the contour of the femoral head–neck junction exceeds the radius of the femoral head (Fig. 3). A cam morphology was considered present when the α-angle was above or equal to 55° [6, 29, 38, 39].
The α-angle and the status of the growth plate were evaluated and measured blindly by a resident radiologist, under the guidance of a senior consultant radiologist. The images were evaluated according to a standardized protocol, including standardized assessment of the α-angle and growth plate as previously described. To test the inter-observer reliability, MRI images were selected randomly from ten participants and were re-examined by a senior consultant radiologist.
Statistical analysis
Data were analysed using IBM SPSS Statistics for Windows (Version 24.0. Armonk, NY: IBM Corp). The description of data was expressed in terms of mean and standard deviation (SD). The inter-rater reliability of the measurements was determined with the intraclass correlation coefficient (ICC 2.1) (two-way random model, absolute agreement, single measures). To categorize the level of agreement among ICC values, we used the classification system proposed by Shrout and Fleiss [36]. ICC values less than 0.40 represent poor, values between 0.40 and 0.75 represent fair to good, and values above 0.75 represent excellent reliability. SEM, a reliability statistic which quantifies measurement error in the same units as the original measurement was calculated as SEM = SD \(\surd {\text{E}}1 - {\text{ICC}}\), where SD is the standard deviation of the difference between observations. All tests were two-sided and significance was set at p < 0.05 for each test. A Pearson Chi square test was performed to evaluate the distribution of cam between the sexes.
All pupils of Åre Ski Academy were invited to participate in the present study and comprised the study population; therefore no power analysis was calculated prior to the study. The intention was to match each skier with a control, but it was difficult to recruit accurate age-matched non-athletes. Therefore, the groups were not matched.
Results
Table 1 presents the study population and the distribution of cam morphology between the groups. Seventy-five skiers agreed to participate, 35 females and 40 males (Fig. 4). Twenty-seven non-athletes, 18 females and 9 males, all 16 years old agreed to participate. Three subjects were withdrawn from the study as they did not fulfil all inclusion criteria. Also, failure to attend investigations made only MRI data from 87 participants available for the final analysis.
MRI
The result of the inter-observer test (ICC) analysis for the α-angle [ICC 0.75 (SEM 1.8)] indicated a good level of agreement.
All participants had MRI-verified closed growth plates.
Out of the seven measurements (from 9 o’clock to 3 o’clock), the highest α-angle was generally measured at 1 o’clock in the antero-superior region of the femoral head–neck junction. In 87 participants, 174 hips were analysed, where a total of 53 hips (30%) had cam morphology. The measurements of the α-angle showed equivalent results for the right and left hips, with 26 hips (49%) on the right side and 27 hips (51%) on the left side.
At an individual level, 35 of the subjects (40%) had cam morphology: 10 females (22%) and 25 males (61%) (Table 1). Eighteen subjects of the whole population (21%) and 17 of the skiers (28%) had bilateral cam morphology.
The skiers had a significantly higher prevalence of cam morphology compared with the non-athletes (p = 0.009), where 30 of the skiers (49%) and only 5 of the non-athletes (19%) had cam (Table 1). No significant difference was found between the Mogul and Alpine skiers.
A significant difference was found between the sexes in this study population, where 10 of the females (22%) and 25 of the males (61%) had cam morphology (p < 0.001). Among the skiers there was also a significant difference between females and males (p < 0.001), where 8 of the females (28%) and 22 of the males (69%) had cam. This difference between the sexes was not found in the non-athletic group.
Across the sample, even the participants with an α-angle less than 55°, a tendency was shown with the skiers having higher α-angle values in all measurements (from 9 o’clock to 3 o’clock) compared with the control group.
Discussion
The most important findings of the present study were that (1) a significantly higher prevalence of cam morphology was shown amongst the young skiers compared with the non-athletes (49% vs. 19%), and (2) there was a significantly lower prevalence of cam amongst the female subjects compared with their male counterparts (22% vs. 61%).
The exact mechanism behind the formation of cam has still not been identified. Siebenrock et al. [37] suggest that cam morphology is a consequence of an alteration of the growth plate (extension of the growth plate) and that this is more common in young athletes. It is possible that the cam morphology is acquired, due to repetitive and heavy load, during the years associated with the adolescent growth spurt, because of a vulnerability of the skeleton and growth plate. Bailey et al. [7] showed that there is a significant time difference in peak bone velocity (bone mineral content accumulation) between girls (12.5 years) and boys (14.1 years). The peak height velocity appeared approximately 1 year earlier than the peak bone velocity (girls 11.8 and boys 13.5 years). Because of the lag time between the peak bone height velocity and the peak bone mineral content alongside higher hormonal levels, the skeleton is especially more responsive to mechanical stimuli during the years accompanying the adolescent growth spurt [7]. Biomechanical studies have shown that the growth plate is the most vulnerable part in the growing hip and is especially sensitive to heavy loading during hip flexion and/or external rotation [20, 33]. The growth disturbance may be due to repetitive micro-fractures, which could disrupt the arterial blood supply to the growth plate and inhibit the normal ossification of the chondrocytes, resulting in a delayed closure of the growth plate [24, 35], and the development of cam morphology.
The prevalence of cam morphology may vary depending on imaging modality, definition of cam morphology, age and sex. In the present study, we chose MRI because it has been used in several previous studies investigating cam, and cam morphology was considered present when the α-angle was above or equal to 55° [6, 19, 27, 29, 38, 39]. All participants in the present study had closed growth plates and were therefore considered skeletally mature [3, 29]. In the elite skiers group, there was an equal distribution between the sexes, but in the control group there was an overrepresentation of females.
Compared with other studies, with regard to asymptomatic controls, the present study showed a slightly higher prevalence of cam in both females and males. Others have reported a prevalence of cam morphology in asymptomatic study populations ranging from 5.2 to 24.7% (females 5.2–5.4% and males 9–24.7%) [1, 14, 16, 32, 38]. In the present study, the prevalence was 19.2% (females 11.7% and males 33.3%). The control group was selected from the same geographical area as the Åre Ski Academy is located, and therefore they might be more active than average high-school pupils, as the population in this region is generally active. Moreover, it was difficult to recruit controls and the smaller cohort size, compared with the skiers, might have affected the results. Especially the male controls are underrepresented in this study and this might have contributed to the relatively high prevalence of cam among the controls.
Moreover, the present results correlate well with those in previous studies involving athletes in different sports such as soccer, track and field, ice hockey and basketball [1, 3, 9, 23, 29, 37,38,39, 42]. Philippon et al. [29] found that the prevalence of MRI-verified cam morphology (α-angle ≥ 55°) was higher among young skiers (40%) than the average non-athletic control (as found in other studies), but lower compared with age-matched ice hockey players (79%). Compared to the present study, they reported a lower prevalence of cam amongst male skiers (61% vs. 40%). Phillipon et al.’s study included a relatively small group of male skiers with closed growth plates and the study does not specify at which level or type of skiing (Mogul, Alpine, cross-country, etc.) the skiers train/compete.
Only few studies on females and cam morphology have been published, and there are no previous investigations on the prevalence of cam in female skiers. In other sports, female athletes have a reported lower prevalence of cam and this was also found in the present study [11]. We found that men had a threefold higher prevalence of cam morphology compared with females (61% vs 22%). Other studies have reported a higher prevalence of cam in women, but the methodology differs between the studies (radiographic method, cutoff for cam morphology, etc.). For example, Kapron et al. [21] found that 48% of female mixed athletes had cam morphology. Gerhardt et al. [13] found a prevalence of 50% cam morphology in elite female soccer players and 68% in elite male soccer players. On the other hand, in professional ballet dancers, Harris et al. [17] found that 12% of the female dancers had cam morphology, compared with 57% of the males.
In line with previous studies, we found that out of the seven measurements (from 9 o’clock to 3 o’clock), the largest α-angle was measured at 1 o’clock in the antero-superior region of the femoral head–neck junction [31, 40].
A strength with the present study is the equal distribution between females and males in the elite skiers group. More studies including female athletes are, however, needed to establish a greater understanding of cam morphology of the hips and the mechanism behind it. A highly relevant strength of the present study is that from early ages, boys and girls train together and are therefore exposed to a comparable amount of training, competing and load; i.e. this group of skiers train together depending on age and not sex. Regardless, the prevalence of cam morphology was shown to be considerably lower amongst the study’s female population. This could give important clues to the mechanism behind cam formation.
It is tempting to speculate if the difference in prevalence of cam morphology between females and males can be explained by the earlier closure of the female growth plate. When the load of training/competing increases with age, the growth plate is already closed and no cam morphology is therefore acquired.
The present study included both athletes and non-athletes of both sexes living and studying in the same geographical area. The non-athletes are a strength to this study and place the skiers results in perspective. The study includes a relatively large group of skiers that is equally divided between female and male skiers. A larger sample group with equal subgroup participation might have shown greater differences between the skiers and non-athletes, but also amongst the skiers divided into female/male and skiing disciplines. The inclusion criteria in the present study selected only a healthy population; however; this may have limited the ability to distinguish greater differences in the MRI measurements, compared with skiers presenting symptoms of FAIS.
Conclusion
Young elite skiers are shown to have a higher prevalence of cam morphology of the hip, compared with non-athletes, and this appears to be more prevalent in males. This suggests that intense training load, during growth, may be a risk factor for the development of cam morphology in young elite skiers.
References
Agricola R, Bessems JH, Ginai AZ, Heijboer MP, van der Heijden RA, Verhaar JA et al (2012) The development of cam-type deformity in adolescent and young male soccer players. Am J Sports Med 40:1099–1106
Agricola R, Heijboer MP, Bierma-Zeinstra SM, Verhaar JA, Weinans H, Waarsing JH (2013) Cam impingement causes osteoarthritis of the hip: a nationwide prospective cohort study (CHECK). Ann Rheum Dis 72:918–923
Agricola R, Heijboer MP, Ginai AZ, Roels P, Zadpoor AA, Verhaar JA et al (2014) A cam deformity is gradually acquired during skeletal maturation in adolescent and young male soccer players: a prospective study with minimum 2-year follow-up. Am J Sports Med 42:798–806
Agricola R, Heijboer MP, Roze RH, Reijman M, Bierma-Zeinstra SM, Verhaar JA et al (2013) Pincer deformity does not lead to osteoarthritis of the hip whereas acetabular dysplasia does: acetabular coverage and development of osteoarthritis in a nationwide prospective cohort study (CHECK). Osteoarthr Cartil 21:1514–1521
Agricola R, Waarsing JH, Arden NK, Carr AJ, Bierma-Zeinstra SM, Thomas GE et al (2013) Cam impingement of the hip: a risk factor for hip osteoarthritis. Nat Rev Rheumatol 9:630–634
Agricola R, Waarsing JH, Thomas GE, Carr AJ, Reijman M, Bierma-Zeinstra SM et al (2014) Cam impingement: defining the presence of a cam deformity by the alpha angle: data from the CHECK cohort and Chingford cohort. Osteoarthr Cartil 22:218–225
Bailey DA, McKay HA, Mirwald RL, Crocker PR, Faulkner RA (1999) A six-year longitudinal study of the relationship of physical activity to bone mineral accrual in growing children: the university of Saskatchewan bone mineral accrual study. J Bone Miner Res 14:1672–1679
Beck M, Kalhor M, Leunig M, Ganz R (2005) Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Jt Surg Br 87:1012–1018
Byrd JW (2014) Femoroacetabular impingement in athletes: current concepts. Am J Sports Med 42:737–751
Clohisy JC, Baca G, Beaule PE, Kim YJ, Larson CM, Millis MB et al (2013) Descriptive epidemiology of femoroacetabular impingement: a North American cohort of patients undergoing surgery. Am J Sports Med 41:1348–1356
Dickenson E, Wall PDH, Robinson B, Fernandez M, Parsons H, Buchbinder R, Griffin DR (2016) Prevalence of cam hip shape morphology: a systematic review. Osteoarthritis Cartilage 24(6):949–961
Ganz R, Parvizi J, Beck M, Leunig M, Notzli H, Siebenrock KA (2003) Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res 417:112–120
Gerhardt MB, Romero AA, Silvers HJ, Harris DJ, Watanabe D, Mandelbaum BR (2012) The prevalence of radiographic hip abnormalities in elite soccer players. Am J Sports Med 40:584–588
Gosvig KK, Jacobsen S, Sonne-Holm S, Palm H, Troelsen A (2010) Prevalence of malformations of the hip joint and their relationship to sex, groin pain, and risk of osteoarthritis: a population-based survey. J Bone Jt Surg Am 92:1162–1169
Griffin DR, Dickenson EJ, O’Donnell J, Agricola R, Awan T, Beck M et al (2016) The Warwick Agreement on femoroacetabular impingement syndrome (FAI syndrome): an international consensus statement. Br J Sports Med 50:1169–1176
Hack K, Di Primio G, Rakhra K, Beaule PE (2010) Prevalence of cam-type femoroacetabular impingement morphology in asymptomatic volunteers. J Bone Jt Surg Am 92:2436–2444
Harris JD, Gerrie BJ, Varner KE, Lintner DM, McCulloch PC (2016) Radiographic prevalence of dysplasia, cam, and pincer deformities in elite ballet. Am J Sports Med 44:20–27
Heinrich D, van den Bogert AJ, Nachbauer W (2014) Relationship between jump landing kinematics and peak ACL force during a jump in downhill skiing: a simulation study. Scand J Med Sci Sports 24:e180–e187
Ito K, Minka MA II, Leunig M, Werlen S, Ganz R (2001) Femoroacetabular impingement and the cam-effect. A MRI-based quantitative anatomical study of the femoral head-neck offset. J Bone Jt Surg Br 83:171–176
Jonasson PS, Ekstrom L, Sward A, Sansone M, Ahlden M, Karlsson J et al (2014) Strength of the porcine proximal femoral epiphyseal plate: the effect of different loading directions and the role of the perichondrial fibrocartilaginous complex and epiphyseal tubercle—an experimental biomechanical study. J Exp Orthop 1:4
Kapron AL, Peters CL, Aoki SK, Beckmann JT, Erickson JA, Anderson MB et al (2015) The prevalence of radiographic findings of structural hip deformities in female collegiate athletes. Am J Sports Med 43:1324–1330
Kurpiers N, McAlpine PR, Kersting UG (2009) Perspectives for comprehensive biomechanical analyses in Mogul skiing. Res Sports Med 17:231–244
Lahner M, Bader S, Walter PA, Duif C, von Schulze Pellengahr C, Lukas C et al (2014) Prevalence of femoro-acetabular impingement in international competitive track and field athletes. Int Orthop 38:2571–2576
Laor T, Wall EJ, Vu LP (2006) Physeal widening in the knee due to stress injury in child athletes. AJR Am J Roentgenol 186:1260–1264
Leunig M, Casillas MM, Hamlet M, Hersche O, Notzli H, Slongo T et al (2000) Slipped capital femoral epiphysis: early mechanical damage to the acetabular cartilage by a prominent femoral metaphysis. Acta Orthop Scand 71:370–375
Martin HD, Shears SA, Palmer IJ (2010) Evaluation of the hip. Sports Med Arthrosc 18:63–75
Notzli HP, Wyss TF, Stoecklin CH, Schmid MR, Treiber K, Hodler J (2002) The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. J Bone Jt Surg Br 84:556–560
Pfirrmann CW, Mengiardi B, Dora C, Kalberer F, Zanetti M, Hodler J (2006) Cam and pincer femoroacetabular impingement: characteristic MR arthrographic findings in 50 patients. Radiology 240:778–785
Philippon MJ, Ho CP, Briggs KK, Stull J, LaPrade RF (2013) Prevalence of increased alpha angles as a measure of cam-type femoroacetabular impingement in youth ice hockey players. Am J Sports Med 41:1357–1362
Pollard TC, Villar RN, Norton MR, Fern ED, Williams MR, Murray DW et al (2010) Genetic influences in the aetiology of femoroacetabular impingement: a sibling study. J Bone Jt Surg Br 92:209–216
Rakhra KS, Sheikh AM, Allen D, Beaule PE (2009) Comparison of MRI alpha angle measurement planes in femoroacetabular impingement. Clin Orthop Relat Res 467:660–665
Reichenbach S, Juni P, Werlen S, Nuesch E, Pfirrmann CW, Trelle S et al (2010) Prevalence of cam-type deformity on hip magnetic resonance imaging in young males: a cross-sectional study. Arthritis Care Res (Hoboken) 62:1319–1327
Roels P, Agricola R, Oei EH, Weinans H, Campoli G, Zadpoor AA (2014) Mechanical factors explain development of cam-type deformity. Osteoarthr Cartil 22:2074–2082
Sankar WN, Nevitt M, Parvizi J, Felson DT, Agricola R, Leunig M (2013) Femoroacetabular impingement: defining the condition and its role in the pathophysiology of osteoarthritis. J Am Acad Orthop Surg 21(Suppl 1):S7–Ss15
Shih C, Chang CY, Penn IW, Tiu CM, Chang T, Wu JJ (1995) Chronically stressed wrists in adolescent gymnasts: MR imaging appearance. Radiology 195:855–859
Shrout PE, Fleiss JL (1979) Intraclass correlations: uses in assessing rater reliability. Psychol Bull 86:420–428
Siebenrock KA, Behning A, Mamisch TC, Schwab JM (2013) Growth plate alteration precedes cam-type deformity in elite basketball players. Clin Orthop Relat Res 471:1084–1091
Siebenrock KA, Ferner F, Noble PC, Santore RF, Werlen S, Mamisch TC (2011) The cam-type deformity of the proximal femur arises in childhood in response to vigorous sporting activity. Clin Orthop Relat Res 469:3229–3240
Siebenrock KA, Kaschka I, Frauchiger L, Werlen S, Schwab JM (2013) Prevalence of cam-type deformity and hip pain in elite ice hockey players before and after the end of growth. Am J Sports Med 41:2308–2313
Siebenrock KA, Wahab KH, Werlen S, Kalhor M, Leunig M, Ganz R (2004) Abnormal extension of the femoral head epiphysis as a cause of cam impingement. Clin Orthop Relat Res 418:54–60
Sporri J, Kroll J, Haid C, Fasel B, Muller E (2015) Potential mechanisms leading to overuse injuries of the back in Alpine ski racing: a descriptive biomechanical study. Am J Sports Med 43:2042–2048
Tak I, Weir A, Langhout R, Waarsing JH, Stubbe J, Kerkhoffs G et al (2015) The relationship between the frequency of football practice during skeletal growth and the presence of a cam deformity in adult elite football players. Br J Sports Med 49(9):630–634
Thomas GE, Palmer AJ, Batra RN, Kiran A, Hart D, Spector T et al (2014) Subclinical deformities of the hip are significant predictors of radiographic osteoarthritis and joint replacement in women. A 20 year longitudinal cohort study. Osteoarthr Cartil 22:1504–1510
Yuan BJ, Bartelt RB, Levy BA, Bond JR, Trousdale RT, Sierra RJ (2013) Decreased range of motion is associated with structural hip deformity in asymptomatic adolescent athletes. Am J Sports Med 41:1519–1525
Acknowledgements
The authors acknowledge the financial support of the Research and Development Unit, Region Jämtland Härjedalen County Council and Region Västra Götaland County Council, the Swedish National Centre for Research in Sports, and Carl Bennet AB. The authors would also like to thank Flemming Pedersen, MD, and Zaid Obady, MD, at the Department of Radiology at Östersund Hospital, Sweden, for their help with the radiological examination, and Christer Johansson, OrigoVerus AB, Gothenburg, Sweden, for statistical assistance. The authors also thank Åke Hamberg, MD, at the Department of Orthopaedics at Östersund Hospital, Sweden, for helping with the recruitment of young nonathletes.
Funding
No funding was used.
Author information
Authors and Affiliations
Contributions
ASA contributed substantially to the study design, conception, acquisition of data analysis, interpretation of data, article writing, and drafting the manuscript for critical revision. CA participated in the study design, data collection, analysis and interpretation. ASA, CA, CT, PJ, OT, MS, LS, JK, and AB contributed significantly, and participated with writing of the manuscript. All authors approved final manuscript prior to submission.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the regional and institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study. For participants younger than 18 years, informed written consent was also obtained from one parent.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Aminoff, A.S., Agnvall, C., Todd, C. et al. Young elite Alpine and Mogul skiers have a higher prevalence of cam morphology than non-athletes. Knee Surg Sports Traumatol Arthrosc 28, 1262–1269 (2020). https://doi.org/10.1007/s00167-018-5236-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-018-5236-4