
Abstract
Purpose
The infrapatellar fat pad (IFP) is a common cause of knee pain and loss of knee flexion and extension. However, its anatomy and behavior are not consistently defined.
Methods
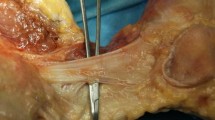
Thirty-six unpaired fresh frozen knees (median age 34 years, range 21–68) were dissected, and IFP attachments and volume measured. The rectus femoris was elevated, suprapatellar pouch opened and videos recorded looking inferiorly along the femoral shaft at the IFP as the knee was flexed. The patellar retinacula were incised and the patella reflected distally. The attachment of the ligamentum mucosum (LMuc) to the intercondylar notch was released from the anterior cruciate ligament (ACL), both menisci and to the tibia via meniscotibial ligaments. IFP strands projecting along both sides of the patella were elevated and the IFP dissected from the inferior patellar pole. Magnetic resonance imaging (MRI) of one knee at ten flexion angles was performed and the IFP, patella, tibia and femur segmented.
Results
In all specimens the IFP attached to the inferior patellar pole, femoral intercondylar notch (via the LMuc), proximal patellar tendon, intermeniscal ligament, both menisci and the anterior tibia via the meniscotibial ligaments. In 30 specimens the IFP attached to the anterior ACL fibers via the LMuc, and in 29 specimens it attached directly to the central anterior tibia. Proximal IFP extensions were identified alongside the patella in all specimens and visible on MRI [medially (100% of specimens), mean length 56.2 ± 8.9 mm, laterally (83%), mean length 23.9 ± 6.2 mm]. Mean IFP volume was 29.2 ± 6.1 ml. The LMuc, attached near the base of the middle IFP lobe, acting as a ‘tether’ drawing it superiorly during knee extension. The medial lobe consistently had a pedicle superomedially, positioned between the patella and medial trochlea. MRI scans demonstrated how the space between the anterior tibia and patellar tendon (‘the anterior interval’) narrowed during knee flexion, displacing the IFP superiorly and posteriorly as it conformed to the trochlear and intercondylar notch surfaces.
Conclusion
Proximal IFP extensions are a novel description. The IFP is a dynamic structure, displacing significantly during knee motion, which is, therefore, vulnerable to interference from trauma or repetitive overload. Given that this trauma is often surgical, it may be appropriate that surgeons learn to minimize injury to the fat pad at surgery.








Similar content being viewed by others

Abbreviations
- IFP:
-
Infrapatellar fat pad
- ACL:
-
Anterior cruciate ligament
- LigMuc:
-
Ligamentum mucosum
- RF:
-
Rectus femoris
- VI:
-
Vastus intermedius
- ITB:
-
Iliotibial band
- MRI:
-
Magnetic resonance imaging
- LCL:
-
Lateral collateral ligament
- MCL:
-
Medial collateral ligament
References
Abràmoff MD, Magalhães PJ, Ram SJ (2004) Image processing with ImageJ. Biophotonics 11(7):36–42
Abreu MR, Chung CB, Trudell D, Resnick D (2008) Hoffa’s fat pad injuries and their relationship with anterior cruciate ligament tears: new observations based on MR imaging in patients and MR imaging and anatomic correlation in cadavers. Skeletal Radiol 37(4):301–306
Bennell K, Hodges P, Mellor R, Bexander C, Souvlis T (2004) The nature of anterior knee pain following injection of hypertonic saline into the infrapatellar fat pad. J Orthop Res 22(1):116–121
Bohnsack M, Hurschler C, Demirtas T, Rühmann O, Stukenborg-Colsman C, Wirth C-J (2005) Infrapatellar fat pad pressure and volume changes of the anterior compartment during knee motion: possible clinical consequences to the anterior knee pain syndrome. Knee Surg Sports Traumatol Arthrosc 13(2):135–141
Bohnsack M, Meier F, Walter GF, Hurschler C, Schmolke S, Wirth CJ, Rühmann O (2005) Distribution of substance-P nerves inside the infrapatellar fat pad and the adjacent synovial tissue: a neurohistological approach to anterior knee pain syndrome. Arch Orthop Trauma Surg 125(9):592–597
Bohnsack M, Wilharm A, Hurschler C, Rühmann O, Stukenborg-Colsman C, Wirth CJ (2004) Biomechanical and kinematic influences of a total infrapatellar fat pad resection on the knee. Am J Sports Med 32(8):1873–1880
Brooker B, Morris H, Brukner P, Mazen F, Bunn J (2009) The macroscopic arthroscopic anatomy of the infrapatellar fat pad. Arthroscopy 25(8):839–845
Chuckpaiwong B, Charles HC, Kraus VB, Guilak F, Nunley JA (2010) Age-associated increases in the size of the infrapatellar fat pad in knee osteoarthritis as measured by 3T MRI. J Orthop Res 28(9):1149–1154
Clockaerts S, Bastiaansen-Jenniskens YM, Runhaar J, Van Osch GJVM., Van Offel JF, Verhaar JAN, De Clerck LS, Somville J (2010) The infrapatellar fat pad should be considered as an active osteoarthritic joint tissue: a narrative review. Osteoarthr Cartil 18(7):876–882
Crossley K, Bennell K, Green S, Cowan S, McConnell J (2002) Physical therapy for patellofemoral pain a randomized, double-blinded, placebo-controlled trial. Am J Sports Med 30(6):857–865
Davies D, White J (1961) The structure and weight of synovial fat pads. J Anat 95(Pt 1):30
Dixon WT (1984) Simple proton spectroscopic imaging. Radiology 153(1):189–194
Dodds A, Halewood C, Gupte C, Williams A, Amis A (2014) The anterolateral ligament. Bone Joint J 96(3):325–331
Dragoo JL, Johnson C, McConnell J (2012) Evaluation and treatment of disorders of the infrapatellar fat pad. Sports Med 42(1):51–67
Dragoo JL, Phillips C, Schmidt JD, Scanlan SF, Blazek K, Steadman JR, Williams A (2010) Mechanics of the anterior interval of the knee using open dynamic MRI. Clin Biomech 25(5):433–437
Dye SF, Vaupel GL, Dye CC (1998) Conscious neurosensory mapping of the internal structures of the human knee without intraarticular anesthesia. Am J Sports Med 26(6):773–777
Gallagher J, Tierney P, Murray P, O’Brien M (2005) The infrapatellar fat pad: anatomy and clinical correlations. Knee Surg Sports Traumatol Arthrosc 13(4):268–272
Havers C (1691) Osteologia nova, or some new observations of the bones, and the parts belonging to them, with the manner of their accretion and nutrition. Samuel Smith, London
Hoffa AA (1904) The influence of the adipose tissue with regard to the pathology of the knee joint. J Am Med Assoc XLIII (12):795–796
Jacobson JA, Lenchik L, Ruhoy MK, Schweitzer ME, Resnick D (1997) MR imaging of the infrapatellar fat pad of Hoffa. Radiographics 17(3):675–691
Krenn V, Hofmann S, Engel A (1990) First description of mechanoreceptors in the corpus adiposum infrapatellare of man. Cells Tissues Organs 137(2):187–188
MacConaill M (1953) The movements of bones and joints. Bone Jt J 35(2):290–297
Newell R (1991) A complete intra-articular fat pad around the human patella. J Anat 179:232
Özkur A, Adaletli I, Sirikci A, Kervancioglu R, Bayram M (2005) Hoffa’s recess in the infrapatellar fat pad of the knee on MR imaging. Surg Radiol Anat 27(1):61–63
Saddik D, McNally E, Richardson M (2004) MRI of Hoffa’s fat pad. Skeletal Radiol 33(8):433–444
Schindler OS (2014) ‘The Sneaky Plica’ revisited: morphology, pathophysiology and treatment of synovial plicae of the knee. Knee Surg Sports Traumatol Arthrosc 22(2):247–262
Solbak NM, Heard BJ, Achari Y, Chung M, Shrive NG, Frank CB, Hart DA (2015) Alterations in Hoffa’s fat pad induced by an inflammatory response following idealized anterior cruciate ligament surgery. Inflamm Res 64(8):615–626
Sonnery-Cottet B, Archbold P, Zayni R, Thaunat M, Bortolletto J, Fayard J-M, Chambat P (2011) High lateral portal for sparing the infrapatellar fat-pad during ACL reconstruction. Orthop Traumatol Surg Res 97(8):870–873
Steadman JR, Dragoo JL, Hines SL, Briggs KK (2008) Arthroscopic release for symptomatic scarring of the anterior interval of the knee. Am J Sports Med 36(9):1763–1769
Stephen JM, Urquhart DW, van Arkel RJ, Ball S, Jaggard MK, Lee JC, Church J (2016) The use of sonographically guided botulinum toxin type a (dysport) injections into the tensor fasciae latae for the treatment of lateral patellofemoral overload syndrome. Am J Sports Med 44(5):1195–1202
Sun K, Tordjman J, Clément K, Scherer PE (2013) Fibrosis and adipose tissue dysfunction. Cell Metab 18(4):470–477
Tangchitphisut P, Srikaew N, Numhom S, Tangprasittipap A, Woratanarat P, Wongsak S, Kijkunasathian C, Hongeng S, Murray IR, Tawonsawatruk T (2016) Infrapatellar fat pad: an alternative source of adipose-derived mesenchymal stem cells. Arthritis 2016:103–113. https://doi.org/10.1155/2016/4019873
Woodley SJ, Latimer CP, Meikle GR, Stringer MD (2012) Articularis genus: an anatomic and MRI study in cadavers. J Bone Jt Surg Am 94(1):59–67
Yoon KH, Tak DH, Ko TS, Park SE, Nam J, Lee SH (2017) Association of fibrosis in the infrapatellar fat pad and degenerative cartilage change of patellofemoral joint after anterior cruciate ligament reconstruction. Knee 24(2):310–318
Acknowledgements
A special thank you to the radiographers of Fortius clinic for their assistance in scanning and David Hillier of Siemens for his advice.
Funding
This study was funded with a grant from Fortius Clinic, London.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
No authors have a conflict of interest or competing interests to declare.
Ethical approval
Ethical approval for this study was obtained from Imperial College London REC, approval number: R160014.
Electronic supplementary material
Below is the link to the electronic supplementary material.
167_2018_4943_MOESM1_ESM.mp4
Video 1: Looking distally along the anterior shaft of the tibia at the IFP from superior to inferior. The tibia is fixed in position on a bench and the femur flexed and extended from 0º-120º with the quadriceps elevated to enable IFP visualization. (MP4 4973 KB)
Video 2: Viewed from medial to lateral at the IFP with the femur fixed, and the tibia flexed around it. The medial meniscus is removed to improve visualization. The IFP can be seen to fill down behind the patellar tendon in knee extension and move out of the anterior interval during knee flexion. (MOV 42643 KB)
Video 3: An animation showing IFP deformation from the segmented MRI scans during movement through 0º-120º flexion, played on a loop. On the left the IFP has been segmented on its own and on the right, with the tibia (blue), patella (pink), and tibia (yellow). (WMV 1630 KB)
Rights and permissions
About this article

Cite this article
Stephen, J.M., Sopher, R., Tullie, S. et al. The infrapatellar fat pad is a dynamic and mobile structure, which deforms during knee motion, and has proximal extensions which wrap around the patella. Knee Surg Sports Traumatol Arthrosc 26, 3515–3524 (2018). https://doi.org/10.1007/s00167-018-4943-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-018-4943-1