
Abstract
Purpose
Shoulder problems are frequent among senior elite handball players. The objective of this study was to assess the prevalence of shoulder problems among adolescent elite handball players and to investigate potential differences in gender, school grade, playing position and playing level.
Methods
During the 2014 and 2015 pre-season periods, 471 players (age 15–18 years, 54% female) completed a comprehensive baseline questionnaire regarding history of any shoulder pain and shoulder problems experienced during the past season. The players were monitored weekly for one competition season (September–April) regarding shoulder problems and the amount of match and training. Generalised linear models with a binomial link function were used to calculate a prevalence ratio (PR) with 95% confidence interval (CI) to compare the subgroups of players.
Results
In total, 110 players (23%) reported having substantial shoulder problems (defined as moderate/severe reduction in training volume, or moderate/severe reduction in performance, or complete inability to participate) at some point during the follow-up season, of which almost half reported complete inability to participate. Of those players reporting substantial problems, 43% (95% CI 39–48) did so for at least 3 consecutive weeks during the season. The prevalence was significantly higher in female players (PR 1.46, 95% 1.04–2.06) and in backcourt players (PR 1.58, 95% CI 1.08–2.32), but no differences were found for school grade (PR 1.21 95% CI 0.88–1.67) or playing level (PR 1.09 95% CI 0.76–1.56).
Conclusions
The prevalence of substantial shoulder problems in adolescent elite handball players is high, especially among females, and this warrants further studies on risk factors for shoulder injury and the development of prevention strategies in handball players already before the age of 15. These findings also highlight the importance of introducing a clinical monitoring programme on a routine basis and improving the medical support, taking gender-related aspects into consideration, at handball-profiled secondary schools.
Level of evidence
II.
Similar content being viewed by others


Introduction
Handball is a physically challenging sport that includes throwing, jumping, running and side-cutting movements as well as direct and indirect contact with opponents, which leads to a high injury rate [5]. The injury rate in youth handball players has been shown to be between 9.9 and 41.0 injuries per 1000 match hours and between 0.9 and 2.6 injuries per 1000 training hours [15, 19, 24]. Focusing on the incidence of newly sustained injuries exclusively leads, however, to the inability to describe the whole spectrum of overuse-related and long-standing shoulder problems among handball players [6, 8]. Recently, high prevalence of shoulder problems has been reported in both senior male and female elite players [1, 6, 16]. However, there is no study that has investigated the prevalence of shoulder problems among adolescent elite handball players, including potential associations with gender, school grade, playing position and playing level. The objective of this study was therefore to assess the prevalence of shoulder problems, and especially substantial problems, in adolescent elite handball players and to investigate potential differences in gender, school grade, playing position, and playing level. The hypothesis was that there is a higher prevalence of substantial shoulder problems in female players, in higher school grades, in backcourt players and in those competing at the highest playing level.
Materials and methods
This study was based on data from a prospective cohort study called the Karolinska Handball Study (KHAST) with the main aim to investigate potential risk factors for developing shoulder injuries among male and female adolescent elite handball players in Sweden. Details about the general methodology, study population and the study design are reported elsewhere and will not be fully repeated below [3].
Population
Briefly, ten out of 38 handball-profiled secondary schools in Sweden met the inclusion criteria and all these accepted to participate in the study [3]. Out of 552 eligible students aged 15–19 years in the ten schools, 471 male and female players were included during the 2014 and 2015 pre-season periods (Table 1).
Baseline questionnaire and weekly monitoring of shoulder problems
At inclusion, all players completed a baseline questionnaire based on Fahlström’s questionnaire [11], and a modified Swedish version of the Oslo Sports Trauma Research Center (OSTRC) overuse injury questionnaire [8, 10]. The OSTRC overuse injury questionnaire was modified in that instead of asking for shoulder problems during the past week, shoulder problems during the past season was asked for in the baseline questionnaire [3]. The players were also asked if they have had any previous shoulder pain during handball participation at any point during their carrier. The baseline questionnaire also included questions on playing position, match and training history, and playing level.
Players were thereafter monitored weekly during one competition season (September–April) during the 2014–2015 or 2015–2016 seasons. Shoulder problems, traumatic injuries, and match and training load were registered using a Swedish version of the OSTRC overuse injury questionnaire [10]. Briefly, an e-mail with the link to the questionnaire was sent to the players every Sunday morning. If the players did not respond initially, they automatically received an email reminder on a daily basis. If no response was received from the players by the following Wednesday, they also received a reminder via a short message service (SMS) including the link to the weekly report. If players also failed to respond to this SMS reminder within 2 days, a research assistant contacted them over the telephone. The survey software prevented incomplete reports by not allowing submission if one or more response were omitted.
If a player reported a traumatic injury, regardless of anatomical site, he/she was contacted by telephone within 2 days by one of two experienced sports medicine clinicians, for additional standardised questions regarding the anatomical site, injury situation, any medical care, and any injury diagnosis by a health care provider. If the player did not answer the phone call he/she received the questions about the traumatic injury by e-mail.
Operational definitions
Based on information from the baseline questionnaire (regarding the preceding season) and from the weekly monitoring (regarding the follow-up season), shoulder problems were categorised into two types; any shoulder problems and substantial shoulder problems. If a player reported a problem in any of the four questions in the modified Swedish OSTRC overuse injury questionnaire this was categorised as any shoulder problem. For substantial shoulder problems, we used the same definition as Clarsen et al. “Players who reported (shoulder) problems leading to moderate or severe reductions in training volume, or moderate or severe reductions in sports performance, or complete inability to participate in sport” [8]. Consequently, players who selected options 3, 4 or 5 in questions 2 and/or 3 in the questionnaire were categorised as having substantial shoulder problems.
When comparing the prevalence between playing positions, wing and line players were categorised together as 6-m players. Playing level was dichotomised in national level, defined as players who played for an adolescent national team or were summoned to a national camp during the preceding season, and regional level, defined as players who did not have this exposure.
Ethics
This study was approved by the Regional Ethics Review Board of the Karolinska Institutet, Sweden (2013/1722-31/4). All participating players, and legal guardians when appropriate, gave written informed consent before entering the study.
Statistical analyses
Descriptive data, about player characteristics, are presented as numbers and mean values with standard deviation (SD) or proportions with 95% confidence interval (95% CI). Four types of prevalence measures were calculated: (1) week prevalence of any shoulder problems and substantial shoulder problems (defined as any shoulder problems or substantial shoulder problems during the preceding week during the follow-up season), (2) season prevalence of any shoulder problems and substantial shoulder problems retrospectively measured via the baseline questionnaire (defined as any shoulder problems or substantial shoulder problems during the preceding season), (3) season prevalence of any shoulder problems and substantial shoulder problems prospectively measured via the weekly reports (defined as any shoulder problems or substantial shoulder problems during the follow-up season), and (4) the lifetime prevalence of shoulder pain (defined as any shoulder pain during handball participation at some point during the handball carrier). The average weekly prevalence was calculated by dividing the number of players who reported having any shoulder problem and substantial problems, respectively, at each week during the season by the number of reports for that week [8]. The season prevalence was calculated by dividing the numbers of players who reported having any shoulder problem and substantial shoulder problems, respectively, at some point during the season by the total numbers of players in the cohort. Finally, the lifetime prevalence of shoulder pain was calculated by dividing the number of players who reported having had any previous shoulder pain during handball participation by the total numbers of players in the cohort.
To estimate the association between the different prevalence measures of shoulder problems/pain and gender, school grade, playing position, and playing level, prevalence ratio (PR) with 95% confidence intervals CI was calculated using generalised linear models with a binomial link function. All factors (gender, school grade playing position and playing level) were included in each model, respectively. Based on previous reported prevalence for shoulder problems from senior elite handball players [6, 16], and an estimation of the proportion of gender, school grade, playing position and playing level, using a power of 80%, a significance level of 5%, a drop-out rate of 10%, approximately 400 players were needed to describe the prevalence and PR, with a follow-up period of one competitive season.
Potential differences in gender, school grade, playing position and playing level, height, weight, BMI, and years of playing handball between those responding to less than 50% of the weekly reports and those responding to 50% or more was assessed using unpaired t test and Chi-square test. STATA software (STATA/ICIC 14.1, StataCorp, Texas, USA) was used for all statistical analysis and the level of significance was set at 0.05.
Results
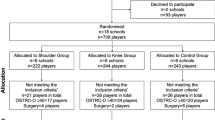
In total, 81 players did not consent to participate in the study and another 26 players did not finish the follow-up, mainly due to quitting their studies at the handball-profiled school (Fig. 1).

Study flow chart showing the recruitment, dropout and the response rate to the weekly reports. *Dropouts were included in the analysis and contributed as long they were in the study
The average response rate to the weekly questionnaire was 93% (range 87–98%), 73% of the players responded to all of the weekly reports and 85% of the players responded to more than 90% of the weekly reports. In total, 12,931 weekly reports were collected during the follow-up season.
Prevalence of shoulder problems and pain
Week prevalence
The weekly prevalence of any shoulder problems and substantial shoulder problems, respectively, was 25% (95% CI 23–27) and 6% (95% CI 5–7).
Season prevalence during the preceding season
The prevalence of any shoulder problems and substantial shoulder problems during the preceding season (assessed retrospectively in the baseline questionnaire) was 28% (95% CI 24–32) and 13% (95% CI 10–16), respectively. The prevalence of any shoulder problems was higher in female players and in backcourt players (Table 2). The prevalence of substantial shoulder problems was higher in 2nd and 3rd grade students compared with 1st grade students (Table 2).
Season prevalence during the follow-up season
The season prevalence of any shoulder problems and substantial shoulder problems (assessed prospectively in the weekly reports) was 44% (95% CI 40–48) and 23% (95% CI 20–27), respectively. Of those reported substantial shoulder problems, 48% reported complete inability to participate due to shoulder problems. The prevalence of any and substantial shoulder problems were both higher in female players and backcourt players (Table 3).
Lifetime prevalence of shoulder pain
The lifetime prevalence of shoulder pain (assessed retrospectively in the baseline questionnaire) was 41% (95% CI 36–45), and was higher among female players compared with males, 46 versus 35% (PR 1.26, 95% 1.01–1.57) and among backcourt players compared with 6-m players, 51 versus 32% (PR 1.57, 95% CI 1.22–2.03). The lifetime prevalence of shoulder pain was also higher among 2nd and 3rd grade students compared with 1st grade students, 45 versus 37% (PR 1.22, 95% CI 0.99–1.50). No difference was seen for playing level, 43 versus 41% (PR 1.07, 95% CI 0.84–1.35).
Duration of the shoulder problems
In total, 75% (95% CI 69–81) of those with any shoulder problems reported such problems for at least 3 consecutive weeks during the season. Similarly, 43% (95% CI 39–48) of those with substantial shoulder problems reported such problems for at least 3 consecutive weeks during the season. Of those with shoulder problems and substantial shoulder problems at some point during the preceding season, 77% (95% CI 66–85) and 67% (95% CI 58–75) also reported such problems at least once during the follow-up season.
Comparison between players with low and high response rates
There were no significant differences between those responding to less than 50% of the weekly reports (n = 33) and those responding 50% or more (n = 438) in gender, school grade, playing position, and playing level as well as in height, weight, BMI, and years of playing handball (ns).
Discussion
This is the first study to describe the association between shoulder problems and gender, school grade, playing position, and playing level in adolescent elite handball players. The principal findings were a high prevalence of shoulder problems, where almost one in four players reported having substantial shoulder problems at some point during a handball season, and that the shoulder problems were significantly more prevalent among female players and backcourt players.
Prevalence of shoulder problems
Describing the prevalence and burden of injuries is an important first step to develop injury prevention strategies [22]. The average weekly prevalence of substantial shoulder was 6% in this study, which is similar to figures reported in recent studies on senior handball players in Norway [1, 6, 8]. Clarsen et al. [6] reported that 24% of the players had substantial shoulder problems in their dominant shoulder at some point during the season with an average weekly prevalence of 12%, while Andersson et al. [1] and Clarsen et al. [8] reported average weekly prevalence of 8 and 6%, respectively. Our results are also similar to the weekly average prevalence of 5% recently reported in Norwegian secondary school volleyball players [7]. Furthermore, 46% of the female players and 35% of the male players in our study reported having a history of previous shoulder pain, and this is in line with a study in which a lifetime prevalence of shoulder pain was 44% in senior Iranian male and female handball players [14]. Our results are, however, somewhat lower than what has been reported in Norwegian senior elite female handball players, where it was reported that 57% were affected by previous or current shoulder pain [16].
Gender
Female players had a significantly higher prevalence of both any shoulder problems and substantial shoulder problems during the follow-up period. These results are in line with the finding from a recent study on Norwegian senior elite handball players where a higher season prevalence of shoulder problems was reported in female players (26%) compared to male players (20%) [2]. A similar gender-related difference was also reported in Brazilian senior elite players where 9% of the female players reported traumatic shoulder injuries compared to 3% of the male players [12]. Interestingly, similar gender-related differences, with higher rates identified for females, have also been identified for other injuries in team sports such as concussion [18], and anterior cruciate ligament (ACL) injury [17, 23]. However, a recent study on youth handball players did not find any gender difference in shoulder injury incidence [15] and Giroto et al. [12] reported no differences in the proportion of reported overuse shoulder injuries in Brazilian elite senior players. Importantly, there were a higher proportion of female players who reported previous shoulder pain at baseline in our study. Female players may therefore develop shoulder problems at a younger age than do male players, which also would be similar to the relative age effect identified in the ACL injury discrepancy [23]. In addition, female players have demonstrated a higher relative workload compared with male players [4], and this could influence the risk of developing shoulder problems. Finally, Serrien et al. [20] showed that the throwing kinematics differed between male and female players, where male players showed a higher endo/ecorotation in trunk velocity and higher shoulder horizontal abduction angles during the cocking phase. Also, van Den Tillaar et al. showed that the maximal endpoint velocities of the hand and wrist segment during throwing were higher in male players, [21] but no other major gender differences in kinematics were found. Gender-related differences in throwing kinematics may thus influence the risk of developing shoulder problems in handball players, but there is currently no study that investigated this.
School grade
There was no significant difference in the prevalence of any or substantial shoulder problems between 1st grade students and 2nd and 3rd year students during the follow-up season in our study. Interestingly, however, the prevalence of substantial shoulder problems during the preceding season was 8% in the 1st grade students compared with 20% in the 2nd and 3rd grade students. The higher prevalence among 2nd and 3rd grade players could possibly be explained by the fact that most of the players still reported substantial shoulder problem the following season. Another plausible explanation would be that both the physical and psychological demands on the players increase when starting a handball-profiled secondary school. These findings are contrary to the findings in a recent study by Moller et al. [15] where there was no difference in occurrence of shoulder injuries between under-16 and under-18 male and female handball players. However, it should be noted that only time-loss injuries were reported in that study and they used a different injury classification, which might explain the discrepancy between the two studies.
Playing position
Backcourt players had a significantly higher prevalence compared with wing and line players in all categories of shoulder problems in this study. This finding is perhaps not surprising since a backcourt player has a well-known higher overall demand on the shoulder, with largely more frequent high-velocity throwing and they also have a higher exposure to getting stopped by an opponent during breakthroughs or blocking opponent shots which puts the shoulder in vulnerable positions [13].
Playing level
There was no significant differences in the prevalence of shoulder problems between players competing at a national level during the preceding season and those playing only at a regional level, regardless of which definition we used. The most likely explanation to this finding is that all players in our study played handball at a high level, which is a strict criterion for being accepted to study at a handball-profiled secondary school in Sweden. These results are also in line with those in a recent study by Clarsen et al. [6] who showed no association between playing level and shoulder injuries in senior male handball players in Norway.
Methodological considerations
The major strength with this study is the large sample size (471 players) and that the sample is also most likely to be representative for the total population of adolescent elite handball players in Sweden. Also, and in contrast to many previous studies describing shoulder problems in overhead athletes [6, 9, 25, 26], this study has a large number of girls and boys, which thus enables to investigate potential gender-related differences with respect to prevalence of shoulder problems. Moreover, female and backcourt players had significant higher prevalence of shoulder problems regardless of what definition used which strengthens the validity of the results. Finally, to reduce the risk of selection bias, a great effort was put on obtaining a high response rate in this study. To our knowledge, the average weekly response rate of 93% during a season is among the highest ones ever reported in studies on sports injuries using weekly questionnaire data distributed by email/SMS.
Some limitations of this study should also be noted. First, the number of missed days, training sessions or matches or specific shoulder diagnoses was not recorded, since the methodology for self-reporting of complaints according to the OSTRC model was strictly used [8]. Second there could be a risk of misclassification of the outcome when reporting any previous shoulder pain or shoulder problems during the preceding season because the questionnaire used was originally designed to report shoulder problems during the past week. Together with a possible recall bias this may therefore explain why the prevalence reported for the preceding season was lower compared with the follow-up season. Third, this study might be underpowered for analysing differences between school grades, thus these aspects should be addressed further in future studies. Last, approximately every seventh eligible player did not consent to participate in the study, which was slightly higher than expected. As in all studies assessing the prevalence of a condition, there is always a risk of selection bias that may lead to either an under- or an over-estimation of the prevalence. However, the main reason for not being included in this study was that players could not get the written consent from their legal guardians in time before data collection was initiated.
Conclusion
The prevalence of substantial shoulder problems in adolescent elite handball players is high, especially among females, and this warrants further studies on risk factors for shoulder injury and the development of prevention strategies in handball players already before the age of 15. These findings also highlight the importance of introducing a clinical monitoring programme on a routine basis and improving the medical support, taking gender-related aspects into consideration, at handball-profiled secondary schools.
References
Andersson SH, Bahr R, Clarsen B, Myklebust G (2017) Preventing overuse shoulder injuries among throwing athletes: a cluster-randomised controlled trial in 660 elite handball players. Br J Sports Med 51:1073–1080
Andersson SH, Bahr R, Clarsen B, Myklebust G (2017) Risk factors for overuse shoulder injuries in a mixed-gender cohort of 329 elite handball players: previous findings could not be confirmed. Br J Sports Med. https://doi.org/10.1136/bjsports-2017-097648
Asker M, Waldén M, Källgren H, Holm LW, Skillgate E (2017) A prospective cohort study identifying risk factors for shoulder injuries in adolescent elite handball players: the Karolinska Handball Study (KHAST) study protocol. BMC Musculoskelet Disord 18:485
Bojsen Michalsik L, Aagaard P (2015) Physical demands in elite team handball: comparisons between male and female players. J Sports Med Phys Fitness 55:878–891
Chelly MS, Hermassi S, Aouadi R, Khalifa R, van den Tillaar, Chamari K, Shepard RJ (2011) Match analysis of elite adolescent team handball players. J Strength Cond Res 25:2410–2417
Clarsen B, Bahr R, Andersson SH, Munk R, Myklebust G (2014) Reduced glenohumeral rotation, external rotation weakness and scapular dyskinesis are risk factors for shoulder injuries among elite male handball players: a prospective cohort study. Br J Sports Med 48:1327–1333
Clarsen B, Bahr R, Heymans MW, Engedahl M, Midtsundstad G, Rosenlund L, Thorsen G, Myklebust G (2015) The prevalence and impact of overuse injuries in five Norwegian sports: application of a new surveillance method. Scand J Med Sci Sports 25:323–330
Clarsen B, Myklebust G, Bahr R (2013) Development and validation of a new method for the registration of overuse injuries in sports injury epidemiology: the Oslo Sports Trauma Research Centre (OSTRC) overuse injury questionnaire. Br J Sports Med 47:495–502
Edouard P, Degache F, Oullion R, Plessis JY, Gleizes-Cervera S, Calmels P (2013) Shoulder strength imbalances as injury risk in handball. Int J Sports Med 34:654–660
Ekman E, Frohm A, Ek P, Hagberg J, Wirén C, Heijne A (2015) Swedish translation and validation of a web-based questionnaire for registration of overuse problems. Scand J Med Sci Sports 25:104–109
Fahlström M, Yeap JS, Alfredson H, Söderman K (2006) Shoulder pain—a common problem in world-class badminton players. Scand J Med Sci Sports 16:168–173
Giroto N, Hespanhol Junior LC, Gomes MR, Lopes AD (2017) Incidence and risk factors of injuries in Brazilian elite handball players: a prospective cohort study. Scand J Med Sci Sports 27:195–202
Karcher C, Buchheit M (2014) On-court demands of elite handball, with special reference to playing positions. Sports Med 44:797–814
Mohseni-Bandpei MA, Keshavarz R, Minoonejhad H, Mohsenifar H, Shakeri H (2012) Shoulder pain in Iranian elite athletes: the prevalence and risk factors. J Manipulative Physiol Ther 35:541–548
Moller M, Attermann JF, Myklebust G, Wedderkopp N (2012) Injury risk in Danish youth and senior elite handball using a new SMS text messages approach. Br J Sports Med 46:531–537
Myklebust G, Hasslan F, Bahr R, Steffen K (2013) High prevalence of shoulder pain among elite Norwegian female handball players. Scand J Med Sci Sports 23:288–294
Myklebust G, Maehlum S, Holm I, Bahr R (1998) A prospective cohort study of anterior cruciate ligament injuries in elite Norwegian team handball. Scand J Med Sci Sports 8:149–153
O’Connor KL, Baker MM, Dalton SL, Dompier TP, Broglio SP, Kerr ZY (2017) Epidemiology of sport-related concussions in high school athletes: National Athletic Treatment, Injury and Outcomes Network (NATION), 2011–2012 through 2013–2014. J Athl Train 52:175–185
Olsen OE, Myklebust G, Engebretsen L, Bahr R (2006) Injury pattern in youth team handball: a comparison of two prospective registration methods. Scand J Med Sci Sports 6:426–432
Serrien B, Clijsen R, Blondeel J, Goossens M, Baeyens JP (2015) Differences in ball speed and three-dimensional kinematics between male and female handball players during a standing throw with run-up. BMC Sports Sci Med Rehabil 18:7:27
van Den Tillaar R, Cabri JM (2012) Gender differences in the kinematics and ball velocity of overarm throwing in elite team handball players. J Sports Sci 30:807–813
van Mechelen W, Hlobil H, Kemper HC (1992) Incidence, severity, aetiology and prevention of sports injuries. A review of concepts. Sports Med 14:82–99
Waldén M, Hägglund M, Magnusson H, Ekstrand J (2011) Anterior cruciate ligament injury in elite football: a prospective three-cohort study. Knee Surg Sports Traumatol Arthrosc 19:11–19
Wedderkopp N, Kaltoft M, Lundgaard B, Rosendahl M, Froberg K (1997) Injuries in young female players in European team handball. Scand J Med Sci Sports 7:342–347
Wilk KE, Macrina LC, Fleisig GS, Aune KT, Porterfield RA, Harker P, Evans TJ, Andrews JR (2015) Deficits in glenohumeral passive range of motion increase risk of shoulder injury in professional baseball pitchers: a prospective study. Am J Sports Med 43:2379–2385
Wilk KE, Macrina LC, Fleisig GS, Porterfield R, Simpson CD, Harker P, Paparesta N, Andrews JR (2011) Correlation of glenohumeral internal rotation deficit and total rotational motion to shoulder injuries in professional baseball pitchers. Am J Sports Med 39:329–335
Acknowledgements
We would like to thank all the players and coaches who participated in this study. Further we would like to thank all the research assistants and the test leaders and for the contribution in this study. We would also like to express our gratitude to the Swedish Handball Federation for the overall support and patronage.
Funding
The article was funded by Centrum for Idrottsforskning (Grant nos. CIF 2015/11, CIF 2016/6), Folksam Insurance Company and Swedish Naprapathic Association.
Author information
Authors and Affiliations
Contributions
MA, LWH, HK, MW and ES were all involved in the conception and design of the study. MA and ES were responsible for recruitment and data collection. All authors contributed to the writing and revision of the manuscript and read and approved the final manuscript. ES is the study guarantor.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This study was approved by the Regional Ethics Review Board of the Karolinska Institutet, Sweden (2013/1722-31/4).
Informed consent
All participating players, and legal guardians when appropriate, gave written informed consent before entering the study.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Asker, M., Holm, L.W., Källberg, H. et al. Female adolescent elite handball players are more susceptible to shoulder problems than their male counterparts. Knee Surg Sports Traumatol Arthrosc 26, 1892–1900 (2018). https://doi.org/10.1007/s00167-018-4857-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-018-4857-y