
Abstract
Purpose
The healthcare sector is responsible for 6–7% of CO2 emissions. The intensive care unit (ICU) contributes to these CO2 emissions and a shift from a linear system to a circular system is needed. The aim of our research was to perform a material flow analysis (MFA) in an academic ICU. Secondary aims were to obtain information and numbers on mass, carbon footprint, agricultural land occupation and water usage and to determine so-called “environmental hotspots” in the ICU.
Methods
A material flow analysis was performed over the year 2019, followed by an environmental footprint analysis of materials and environmental hotspot identification.
Results
2839 patients were admitted to our ICU in 2019. The average length of stay was 4.6 days. Our MFA showed a material mass inflow of 247,000 kg in 2019 for intensive care, of which 50,000 kg is incinerated as (hazardous) hospital waste. The environmental impact per patient resulted in 17 kg of mass, 12 kg CO2 eq, 300 L of water usage and 4 m2 of agricultural land occupation per day. Five hotspots were identified: non-sterile gloves, isolation gowns, bed liners, surgical masks and syringes (including packaging).
Conclusion
This is the first material flow analysis that identified environmental risks and its magnitude in the intensive care unit.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
This material flow analysis provides the necessary information for the intensive care in its transition from a linear to a circular system, with focus on mass, carbon footprint, agricultural land occupation and water usage. Five environmental hotspots are identified: non-sterile gloves, isolation gowns, bed liners, surgical masks and syringes (including their packaging). |
Introduction
Climate change is adversely affecting human health and health systems [1,2,3]. Recently, more than 200 health journals have called on governments to take emergency action to tackle the “catastrophic harm to health” from climate change [4].
Also, the latest Intergovernmental Panel on Climate Change (IPCC) report [5] shows the urgency for sustainability throughout the whole world. Looking in more detail at the healthcare sector, reports from the United Kingdom (UK) show that the sector is responsible for 6% of CO2 emissions [6]. In the Netherlands, healthcare is responsible for 7% of CO2 emissions [7]. These data mainly focus on the use of electric energy, drugs and mobility of personnel and make no distinction between the different healthcare sectors, hospital departments or specific flows of products or materials.
Given the current climate crisis, we must start working towards more holistic approaches to reduce the impact of the healthcare sector and shift towards a circular economy [8]. In a circular economy there are three core principles: (1) design out waste and pollution (2) keep products and materials in use, and (3) regenerate natural systems [9]. While simple in theory, there are many complexities and trade-offs when shifting towards circular practices. The 7 Pillars (of the Circular Economy framework (materials, energy, water, biodiversity, human society and culture, health and well-being and generating value)) can be used as a holistic lens to map or to describe sustainability issues and to identify environmental hotspots [10]. Based on these environmental issues and hotspots, the 10 R strategies can be used as a starting point for circular interventions by healthcare staff [11]. The 10 Rs represent refuse, rethink, reduce, reuse, repair, refurbish, remanufacture, repurpose, recycle and recover. Refuse is the strategy with the highest impact in the hierarchy of circular interventions, while recover represents the strategy with the lowest impact.
The intensive care unit (ICU) has had an intense period due to the coronavirus disease 2019 (COVID-19) pandemic. We have noticed how many products are needed to care for critically ill patients and the substantial amount of waste those products have caused. We realize that these products have a significant impact on the environment due to their use of resources, production and disposal. Action is needed. Unfortunately, there are no data on what materials are being consumed at the ICU and the so-called environmental hotspots. As stated by Bein et al. “Time is pressing and critical care medicine must participate in the race to zero-emission healthcare systems” [12].
The impact on the environment can be studied by a so-called Life Cycle Assessment (LCA). In more detail, LCAs involve the analysis of the environmental impact of natural resource extraction, manufacturing, packaging, transport, use/reuse, and recycling/waste disposal of certain products or processes [13]. LCAs related to intensive care medicine have been performed for reusable central venous catheter insertion kits [13]and septic ICU patients in the United States and Australia [14]. Regarding the septic ICU patients, the average daily greenhouse gas emissions in the US-ICU was 178 kg carbon dioxide equivalent (CO2-e) emissions, while for the Aus-ICU the carbon footprint was 88 kg CO2-e [13]. Another LCA showed 138 kg CO2-e per bed day for ICU patients [15]. An LCA of all the activities occurring within the entire ICU would be a considerable undertaking, though it is possible.
A different approach for investigating the impact on the environment and to invest in options for circularity in the ICU is to perform a Material Flow Analysis (MFA). An MFA provides a quantitative understanding of all the goods and waste flows that enter and leave the system. It can be used to manage resources and waste flows [16]. Allesch and Brunner found that MFAs are a particularly useful tool for decisions in waste management and therefore also potentially a promising tool to apply in the ICU [17]. At the start of this research, no scientific publications on applying MFA and identification of “environmental hotspots” in the hospital context at the department level were known to the researchers.
Our research aimed to perform an MFA in an ICU. Secondary aims were to obtain information and numbers on mass, carbon footprint, agricultural land occupation and water usage and to determine “environmental hotspots” in the ICU.
Methods
For this single-center study, we conducted an MFA. An MFA is defined by Brunner and Rechberger [16] as “(..) a systematic assessment of the flows and stocks of materials within a system defined in space and time.”
Our research consisted of three stages/phases:
-
A.
Material Flow Analysis
-
B.
Environmental footprint analysis of materials
-
C.
Environmental hotspots identification
Material flow analysis
An MFA was used to map the materials of major product groups entering and leaving the Erasmus University Medical Center (Erasmus MC) ICU in 2019. The MFA was conducted by combining data analysis, measurements, and desk research and was complemented by interviews with staff members (nurses, intensivists and pharmacists) at Erasmus MC. The collected data were used to compare the number of individual materials used in the ICU per day per patient to their aggregated weights.
Scope
This study focused on the material consumption of the ICU. Water and energy consumption by the department are left out of scope. Erasmus MC is a modern academic hospital, opened in 2018. The data collection covered all materials entering and leaving the ICU of the Erasmus MC in 2019. With entering the ICU, the moment of purchase is meant. The impacts of active ingredients in the medicines procured in the ICU were excluded from the environmental impact assessment.
The ICU consists of 56 beds in a mixed surgical and non-surgical setting. Common patient categories are transplantation (liver, kidney, heart and lungs), neurotrauma, cardiology (including out-of-hospital cardiac arrest and surgery), sepsis and respiratory insufficiency. Multiple organ replacement therapies are used (dominated by extracorporeal mebrane oxygenation (ECMO), left ventricular assist device and continuous renal replacement therapy (CRRT)). Patients on ventilation, and/or receiving ECMO and/or CRRT were studied as categories of special interest, regarding the use of materials (e.g. plastics) required for these therapies.
Unit of measurement
The material flows are presented in three different ways:
-
1.
The in- and outflows of the ICU over the entire year in kilogram (kg).
-
2.
The average number of products used (inflows) per patient in numbers per day.
-
3.
The average mass of materials used (inflows) per patient per day in kg.
Inflows and stock
The data from products were derived from different management reports including cleaning, disposables, medicines, and textiles purchased for the ICU. The data included supplier name, name of the product, product category, packaging configuration (amount per package), number of packages ordered, and number of units ordered. All products were assigned to product groups with a coverage of 92.7%, based on the amount. If weights and the material compositions were missing from the reports, then this information was gathered twofold: through desk research including suppliers’ websites and product brochures, and through actual measurement of the weights of products for which no information was available.
The following weights were recorded:
-
Net weight (product excluding the packaging).
-
Primary packaging (the packaging in direct contact with the product e.g., a glass vial).
The following material categories were distinguished, adapted from [16]:
-
Glass
-
Synthetic plastic and rubbers
-
Synthetic fabrics
-
Biobased materials (including fibers, paper and board)
-
Chemicals (cleaning detergents)
-
Metals
The mass inflows of goods were calculated by multiplying the percentage of material by weight and amount.
Outflows
The use of products and disposables results in waste. We did not measure the specific amounts of waste generated by the ICU. We estimated the outflows based on the inflows, with the use of the mass balancing principle. Any additional weight from human biological fluids is considered out of scope.
Environmental footprint assessment
An environmental footprint assessment was conducted to analyze the embodied impacts associated with the materials of the product groups by mass. Each product or packaging unit was modelled based on simple assumptions for the material compositions, found via desk research and through weighing the products and their components. Using these assumptions, compositions for each product or packaging group were defined using the material and manufacturing process entries from the Ecoinvent LCA inventory database 3.6 database (Ecoinvent, Switzerland). These compositions created a weighted average of the impact intensities for each product group. Next, the ReCiPe impact assessment methodology [18] was used to calculate specific environmental impact categories. The following impact categories were used for environmental impact: global warming potential (GWP100) (kg CO2-eq/kg material), agricultural land occupation (m2/kg material) and water usage (m3/kg material) [16].
Environmental hotspot identification
An environmental hotspot can be defined as a problem area causing significant environmental impacts. These hotspots highlight where urgent efforts are required, and where lie opportunities for circular innovation.
Hotspots were identified as products having (1) the highest mass and (2) the highest environmental footprint assessment.
Results
In 2019 2839 patients were admitted to the ICU, covering 13,059 patient days. Supplementary Table 1 shows the patient characteristics of the ICU in 2019, together with the impact of 3 therapies: ventilation, CRRT and ECMO. The tubing, water and filters used for ventilation have a mass of 7005 kg. This is 2.8% of the total inflow and 3.2% of the total use of plastics. CRRT filter sets have a mass of 965 kg (0.4% of total inflow and 3.0% of total use of plastics). ECMO sets show a mass of 269 kg (0.11% of total inflow and 0.84% of total use of plastics).
Material flow analysis
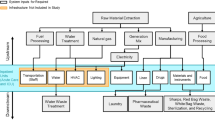
We have identified a total of 247,000 kg of materials used by the Erasmus MC ICU in 2019 (period: from 1/1/2019 to 31/12/2019). Figure 1 visualizes the MFA results, and reveals the distribution of material types across the most commonly used product groups in the ICU, presented on the far left-hand side. The masses of the material types and the subdivision of materials are shown in Supplementary Table 2. Regarding materials, most of the mass is caused by sterile water (61%), predominantly used in liquid medicines (infusion and dialysis fluids).

Material flow analysis of the intensive care; material groups are shown on the left. The flow continues towards products and leaves the ICU with the outflow on the right side. SZA = hospital waste
The data about the distribution of materials are shown in Fig. 2. The weights of the different materials are: medicines 184,190 kg, synthetic plastics and rubbers 32,167 kg, synthetic fabrics 9930 kg, glass 9710 kg, biobased materials 8,148 kg, chemicals 2158 kg and metals 770 kg.

Weight distribution of different material types in percentages. Medicines are excluded from the figure because of their large impact (65% of total mass)
With regard to the specific product groups, personal protective equipment (PPE) (14,100 kg), syringes with packaging (15,898 kg), sterile water (6200 kg) and bedliners (6140 kg) are responsible for 20% of the ICU’s total annual material use.
Figure 3 shows the weight distribution of the product groups with their packaging. The packaging of tissues and compresses has a relative high weight, in relation to the weight of the product itself.

Ratio packing per product group in percentage weight of products and their packaging
The average number of individual units used per patient per day (inflows) is shown in Fig. 4. A high use of gloves (108), compresses (57), liquid medicine (infusion bags, 34), syringes (24) and tubes and connectors (23) were used.

Individual products per patient per day
The average mass of materials used (inflows) per patient per day in kg: 11.9 kg of liquids, such as intravenous fluids, are used per patient per day (Supplementary Fig. 1). This is followed by 0.6 kg of disposable clothing and 0.43 kg bed liners and 0.43 kg sterile water (used during ventilation) per patient per day.
Total mass outflows
Supplementary table 3 shows the total mass outflows of waste and treatments. In the Netherlands, all waste is incinerated, in part as hazardous hospital waste (in special hazardous waste bins). Of the materials that are not consumed directly by the patients, such as medicines and intravenous fluids, around 50,000 kg of waste materials are incinerated as (hazardous) hospital waste. Recycling is limited to glass (1120 kg).
Impact assessment
Figure 5 shows the estimated contribution of the most important product groups to the different environmental impacts, expressed as weight, carbon footprint, agricultural land occupation and water usage. Regarding weight, disposable medical clothing has the highest impact, followed by glass ampoules, sterile water and bed liners. The highest carbon footprint is caused by disposable gloves, syringes and disposable medical clothing. Bed liners have the highest impact on agricultural land occupation. Water usage is most outspoken for the production of disposable gloves. Calculation of the environmental impact per patient per day results in 17 kg of mass, 12 kg CO2 eq, 300 L of water usage and 4 m2 of agricultural land occupation.

Estimated contribution of products or product groups with the highest mass and highest environmental impact. The mass of the medicines itself is excluded. Sterile water shown in this figure is used as a nebulizer (1 L bags) in the mechanical ventilation circuit. Its CO2 emission is relatively small: 0.000438766 CO2-eq/kg
Hotspot identification
Based on the significant embodied impact and frequency of use on the ICU as shown in Figs. 4, 5, five single-use products were identified as key environmental hotspots for circular interventions: non-sterile gloves, isolation gowns, bed liners, surgical masks, and syringes (including their packaging).
Discussion
Based on this MFA, the environmental impact per ICU patient resulted in 17 kg of mass, 12 kg CO2 eq, 300 L of water usage and 4 m2 of agricultural land occupation per day. Five hotspots were identified: non-sterile gloves, isolation gowns, bed liners, surgical masks and syringes (including packaging).
MFAs are widely used in non-healthcare sectors. Examples are used personal computers [19] and engineered nanomaterials in European waste treatment systems [20]. Our results show that it was possible to perform an MFA in an ICU. It gains inside in both the in- and outflow of products used, and the materials that are used and it results in easy-to-interpret outcomes.
The strengths of our study are the thorough investigation of the products, their environmental impact and the environmental impact per patient. The outcome resulted in 5 well-defined hotspots. Since we are the first academic intensive care showing these results, data from other types of intensive cares are needed. With these data, other intensive cares (academic and non-academic) can determine their environmental impact as a whole and per patient. It supports the change towards a circular economy.
MFAs in healthcare settings are lacking. So, no comparison with other data from intensive cares or medical wards is possible. In contrast to an LCA that focuses on one product or a specific patient pathway [13, 14], an MFA provides broad information about, in our case, all materials that enter and leave intensive care. The data create awareness in ICU personnel and the designation of the environmental hotspots is quickly adapted. It opens the discussion among ICU personnel and results in the teamwork that is needed for the change in behavior in moving from a linear to a circular system.
The limitation of our investigation is that it involved only one academic intensive care in the Netherlands. This raises the question of whether our data can be used by other intensive care. Given the five hotspots with products that are widely used, we believe that our outcome is also relevant and useful for other intensive care. Others showed in two LCA studies that the CO2 emissions were 88–178 CO2eq for septic and ICU patients, respectively [13, 14]. These LCA’s took electricity into account. This might explain the 5 to tenfold higher CO2 emissions of their data compared to our data and it underlines the impact of electricity use in the ICU. Besides electricity, we did not investigate the impact of equipment, use of water and mobility on the environment. Since these data may differ a lot between hospitals and countries, they can be added to the data of the MFA by each intensive care separately.
Another limitation is that we were not able to investigate the environmental impact of all medicines used in the ICU. This information is not available in the Eco Invent database and it was not feasible to investigate more than 100 drugs that are used in the ICU separately. We know from other data that medicines are responsible for about 18% of the CO2 footprint in healthcare [7, 21]. This might even be higher in the ICU, because of the extensive use of medication in critically ill. However, we focused on the identification of hotspots of materials to formulate practical interventions. In future studies, the environmental impact of medicines should be taken into account, as is shown in an LCA that studied the environmental impact of morphine [22].
Unfortunately, we could not measure the mass of outflows from the ICU. The mass was estimated based on the total hospital mass and number of patients in the ICU. Specific audits and recycling programs for ICU waste are available elsewhere [23]. All (infectious and non-infectious) solid hospital waste is incinerated in the Netherlands. The CO2 emissions of hazardous waste are higher than those of nonhazardous waste [24]. The challenge will be to implement strict hazardous waste protocols to keep the hazardous waste mass as low as possible, together with the use of waste bins that consist of recycled plastic [25]. We also stress the influence of ICU physicians in this perspective.
The consequences of our data plea for the individual ICUs to create “green teams”, as one of the ways to tackle the environmental problems [26]. These green teams can start the change towards a circular economy, starting with the hotspots. The ICU cannot be considered as an isolated entity. We need others to help with this transition, like societies, faculties, industry and healthcare policymakers [8].
We showed that most environmental impact is caused in our ICU by the use of daily materials rather than material use for specific therapies (ventilation, CRRT and ECMO). It would be interesting to investigate specific therapies in more depth (with LCA’s) in future studies.
Conclusion
Our MFA showed a material mass inflow of 247,000 kg in 2019 for 2839 intensive care patients. The environmental impact per patient resulted in 17 kg of mass, 12 kg CO2 eq, 300 L of water usage and 4 m2 of agricultural land occupation per day. 50,000 kg of this mass is incinerated as (hazardous) hospital waste. Five hotspots were identified: non-sterile gloves, isolation gowns, bed liners, surgical masks, and syringes (including packaging). Our data provide the necessary information for intensive care in its transition from a linear to a circular system.
Data availability
See methods section.
Code availability
Not applicable.
References
Haines A, Ebi K (2019) The imperative for climate action to protect health. N Engl J Med 380:263–273. https://doi.org/10.1056/NEJMra1807873
Ebi KL, Ogden NH, Semenza JC, Woodward A (2017) Detecting and attributing health burdens to climate change. Environ Health Perspect 125:1–8. https://doi.org/10.1289/EHP1509
Mitchell D, Heaviside C, Vardoulakis S, Huntingford C, Masato G, Guillod BP, Frumhoff P, Bowery A, Wallom D, Allen M (2016) Attributing human mortality during extreme heat waves to anthropogenic climate change. Environ Res Lett 11:074006. https://doi.org/10.1088/1748-9326/11/7/074006
Atwoli L, Baqui AH, Benfield T, Bosurgi R, Godlee F, Hancocks S, Horton R, Laybourn-Langton L, Monteiro CA, Norman I, Patrick K, Praities N, Olde Rikkert MGM, Rubin EJ, Sahni P, Smith R, Talley NJ, Turale S, Vázquez D (2021) Call for emergency action to limit global temperature increases, restore biodiversity, and protect health. BMJ 374:n1734. https://doi.org/10.1136/bmj.n1734
Pörtner HO, Roberts DC, Adams H, Adler C, Aldunce P, Ali E, Begum RA, Betts R, Kerr RB, Biesbroek R (2022) Climate Change 2022 Impacts, Adaptation and Vulnerability; Working Group II Contribution to the Sixth Assessment Report of the Intergovernmental Panel on Climate Change. https://www.ipcc.ch/report/ar6/wg2/downloads/report/IPCC_AR6_WGII_FinalDraft_FullReport.pdf. Accessed 27 June 2022
Karliner J, Slotterback S, Boyd R, Ashby B, Steele K (2019) Health Care's Climate Footprint https://noharm-global.org/sites/default/files/documents-files/5961/HealthCaresClimateFootprint_092319.pdf. Accessed 2 July 2022
Gupta Strategists, (2019) Een stuur voor de transitie naar duurzame gezondheidszorg. https://gupta-strategists.nl/studies/een-stuur-voor-de-transitie-naar-duurzame-gezondheidszorg. Accessed 6 June 2022
Hinrichs-Krapels S, Diehl JC, Hunfeld N, van Raaij E (2022) Towards sustainability for medical devices and consumables: the radical and incremental challenges in the technology ecosystem. J Health Serv Res Policy 27:253–254. https://doi.org/10.1177/13558196221110416
Ellen MacArthur Foundation, (2020) What is a Circular Economy? A Framework for an Economy that is Restorative and Regenerative. https://ellenmacarthurfoundation.org/topics/circular-economy-introduction/overview. Accessed 8 June 2022
Kirchherr J, Reike D, Hekkert M (2017) Conceptualizing the circular economy: an analysis of 114 definitions. Resour Conserv Recycl 127:221–232. https://doi.org/10.1016/j.resconrec.2017.09.005
Reike D, Vermeulen W, Witjes S (2018) The circular economy: new or refurbished as CE 3.0? — exploring controversies in the conceptualization of the circular economy through a focus on history and resource value retention options. Resour Conserv Recycl 135:246–264. https://doi.org/10.1016/j.resconrec.2017.08.027
Bein T, Koch S, Schulz C (2021) What’s new in intensive care: environmental sustainability. Intensive Care Med 47:903–905. https://doi.org/10.1007/s00134-021-06455-6
McGain F, Muret J, Lawson C, Sherman JD (2020) Environmental sustainability in anaesthesia and critical care. Br J Anaesth 125:680–692. https://doi.org/10.1016/j.bja.2020.06.055
McGain F, Burnham JP, Lau R, Aye L, Kollef MH, McAlister S (2018) The carbon footprint of treating patients with septic shock in the intensive care unit. Crit Care Resusc 20:304–312
Prasad PA, Joshi D, Lighter J, Agins J, Allen R, Collins M, Pena F, Velletri J, Thiel C (2022) Environmental footprint of regular and intensive inpatient care in a large US hospital. Int J Life Cycle Assess 27:38–49. https://doi.org/10.1007/s11367-021-01998-8
Brunner P, Rechberger H (2004) Practical handbook of material flow analysis. Lewis Publishers, Washington, DC
Allesch A, Brunner P (2015) Material flow analysis as a decision support tool for waste management: a literature review. J Ind Ecol 19:753–764. https://doi.org/10.1111/jiec.12354
Huijbregts MAJ, Steinmann ZJN, Elshout PMF, Stam G, Verones F, Vieira M, Zijp M, Hollander A, van Zelm R (2017) ReCiPe2016: a harmonised life cycle impact assessment method at midpoint and endpoint level. Int J Life Cycle Assess 22:138–147. https://doi.org/10.1007/s11367-016-1246-y
Yoshida A, Tasaki T, Terazono A (2009) Material flow analysis of used personal computers in Japan. Waste Manag 29:1602–1614. https://doi.org/10.1016/j.wasman.2008.10.021
Rajkovic S, Bornhöft N, van der Weijden R, Nowack B, Adam V (2020) Dynamic probabilistic material flow analysis of engineered nanomaterials in European waste treatment systems. Waste Manag 113:118–131. https://doi.org/10.1016/j.wasman.2020.05.032
Malik A, Lenzen M, McAlister S, McGain F (2018) The carbon footprint of Australian health care. Lancet Planet Health 2:e27–e35. https://doi.org/10.1016/S2542-5196(17)30180-8
McAlister S, Ou Y, Neff E, Hapgood K, Story D, Mealey P, McGain F (2016) The Environmental footprint of morphine: a life cycle assessment from opium poppy farming to the packaged drug. BMJ Open 6:e013302. https://doi.org/10.1136/bmjopen-2016-013302
Kubicki MA, McGain F, O’Shea CJ, Bates S (2015) Auditing an intensive care unit recycling program. Crit Care Resusc 17:135–140
Rizan C, Bhutta MF, Reed M, Lillywhite R (2021) The carbon footprint of waste streams in a UK hospital. J Clean Prod 286:125446. https://doi.org/10.1016/j.jclepro.2020.125446
https://www.recyclingmagazine.nl/algemeen/suez-introduceert-inzamelvat-ziekenhuisafval-gerecycled-plastic/30586/. Accessed 27 June 2022
McDermott-Levy R (2011) The nurse’s role on green teams: an environmental health opportunity. Pennsylvania Nurse 66:17–21
Acknowledgements
We would like to thank Dick Tibboel, Hilde de Geus, Dinis Dos Reis Miranda and Jelle Epker for their kind assistance with specific patient data collection and advices.
Funding
The authors have not disclosed any funding.
Author information
Authors and Affiliations
Contributions
NH, JCD, MT, CdP and DG: prepared the manuscript. Data analysis was performed by PvE, JB and SBW.
Corresponding author
Ethics declarations
Conflicts of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Hunfeld, N., Diehl, J.C., Timmermann, M. et al. Circular material flow in the intensive care unit—environmental effects and identification of hotspots. Intensive Care Med 49, 65–74 (2023). https://doi.org/10.1007/s00134-022-06940-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-022-06940-6