
Abstract
Purpose
Information on predisposing risk factors influencing long-term survival after extracorporeal membrane oxygenation (ECMO) support remains scarce. In critically ill patients chronic obstructive pulmonary disease (COPD) is an independent risk factor for mortality and morbidity. We assessed the influence of COPD on cardiovascular and all-cause mortality in patients undergoing ECMO therapy.
Methods
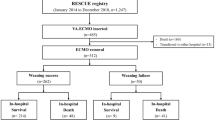
We prospectively included 191 patients undergoing veno-arterial ECMO therapy following cardiovascular surgery at a university-affiliated tertiary care center into our registry.
Results
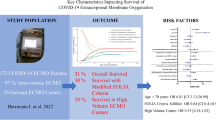
The median follow-up time was 51 months (IQR 34–71 months) corresponding to 4,197 overall months of follow-up. A total of 125 patients (65 %) died; 88 % of deaths were due to cardiovascular causes. Long-term survival was decreased in patients with COPD after 1 year (23 % vs. 44 %) and after 6 years (14 % vs. 35 %) compared to patients without COPD. COPD was independently associated with all-cause mortality with a hazard ratio of 4.22 (95 % CI 1.04–17.11, p = 0.04) and cardiovascular mortality with a hazard ratio of 5.87 (95 % CI 1.41–24.47, p = 0.02).
Conclusions
We identified COPD as a strong and independent predictor of long-term all-cause mortality and cardiovascular mortality in patients undergoing ECMO therapy following cardiovascular surgery. The current study presents valuable information for a comprehensive decision-making process prior to ECMO implantation and helps to identify high-risk patients that may benefit from intensified treatment of co-morbidities and close check-ups after hospital discharge.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Extracorporeal membrane oxygenation (ECMO) support has been established as a therapeutic option for mechanical circulatory support in critically ill patients following cardiovascular surgery [1]. Despite all efforts, long-term prognosis in this patient population remains critical [2–4]. Therefore, the decision to initiate ECMO support should be driven by a comprehensive evaluation of the patients’ individual risk profile. Nevertheless, risk stratification remains challenging because information on specific outcome predictors is scarce [2]. Previous studies predominantly focused on in-hospital mortality [3, 4], whereas predisposing risk factors influencing long-term survival are essentially unknown.
Chronic obstructive pulmonary disease (COPD) is a well-established risk factor in patients undergoing cardiovascular surgery [5–8] and independently predicts mortality and morbidity in intensive care unit (ICU) patients [9, 10]. Furthermore, with the increasing global incidence of COPD [11] and its high prevalence in ICU patients [9], information on the impact of COPD on long-term mortality in patients undergoing ECMO would be valuable for an accurate risk stratification prior to ECMO implantation. Nevertheless, there are no such data from previous investigations. We therefore assessed the influence of COPD on cardiovascular and all-cause mortality in patients undergoing veno-arterial ECMO support following cardiovascular surgery.
Methods
Study population
Between February 2002 and December 2009, we prospectively included patients undergoing veno-arterial ECMO therapy following cardiovascular surgery into our registry. All participants were recruited at the Vienna General Hospital, a university-affiliated tertiary center. The study protocol complies with the Declaration of Helsinki and was approved by the Ethics Committee of the Medical University of Vienna (EK 1952/2012).
ECMO device and management
Indications for ECMO support were clinical criteria of cardiogenic shock such as systolic arterial hypotension (less than 80 mmHg) and signs of end-organ failure, anaerobic metabolism, and metabolic acidosis despite optimized supportive measures (i.e., inotropes, fluids, intra-aortic balloon pump). Hemodynamic criteria were cardiac index less than 1.8 L/m2 body surface area and pulmonary capillary wedge pressure of at least 20 mmHg. The ECMO circuit consisted of a centrifugal pump console (Bio-Console560; Medtronic, Minnesota, USA) with an inline plasma-tight hollow-fiber microporous membrane oxygenator (Affinity NTTM; Medtronic, Anaheim, USA). No additional left-sided venting or atrial septostomy was performed. The ECMO device was routinely checked on a 24-h basis by an experienced perfusionist and the on-shift intensive care physician [12]. The circuit was changed if significant deposition of fibrin or clots were present or blood oxygenation declined sharply. All components were heparin coated. Under ECMO support, lungs were ventilated at low peak airway pressures of less than 25 cmH2O, low physiologic respiratory tidal volumes (6–8 mL/kg), a low respiratory rate (at most 10/min), and the fractional inspired oxygen (FiO2) was reduced to 0.3 [13–16]. FiO2 was adjusted using the ECMO circuit to maintain a PO2 between 80 and 100 mmHg. To define the optimal time of weaning, myocardial recovery was assessed daily using clinical, echocardiographic, and hemodynamic measures. ECMO weaning was cautiously started when a pulsatile arterial waveform was present, intravenous inotropes were successfully reduced, and echocardiographic evaluation demonstrated a stable left and right ventricular systolic function [17]. ECMO weaning trial was performed by progressively reducing pump flow to 1.5 L/min under careful observation of metabolic status, end-organ perfusion, and central venous saturation. If signs of impaired end-organ perfusion occurred during ECMO weaning, the flow was increased to the initial value and ECMO weaning was repeated on a subsequent date. When ECMO weaning was repeatedly impossible, cardiac transplantation or a ventricular assist device was considered. In contrast, if the patient’s hemodynamic status remained stable for at least 24 h, ECMO support was removed by the on-shift cardiac surgeon and the access site was surgically repaired.
Clinical definitions
Diagnosis of COPD and global initiative for chronic obstructive lung disease (GOLD) grade was based on the judgment of two independent physicians on the basis of previous medical reports (e.g., previous hospital discharge letters, pulmonary function tests) and previous COPD medication in accordance with the GOLD executive summary [11]. Cardiovascular risk factors were recorded according to the respective guidelines. Blood samples were collected pre-operatively at time of hospital admission and analyzed without freezing according to local laboratory standard procedure. The European system for cardiac operative risk evaluation (EuroSCORE) was calculated as previously described [18]. The simplified acute physiology score (SAPS) II score [19] was recorded at time of ICU admission.
Study endpoints
The primary study endpoints all-cause mortality and cardiovascular mortality were obtained by screening the national register of death, including screening for the cause of death (according to the International Statistical Classification of Diseases and Related Health Problems 10th Revision).
Statistical analysis
Continuous data were presented as median and interquartile range (IQR) and compared using Mann–Whitney statistics. Discrete data were presented as count and percentage and compared using the chi-squared test. Cox regression analysis was applied to assess the effect of COPD on all-cause and cardiovascular mortality. To account for potential confounding effects, we calculated the risk for death adjusted for the EuroSCORE (excluding chronic pulmonary disease), the type of cardiovascular surgery, and other established cardiovascular risk factors including age, sex, hypertension, diabetes, hypercholesterolemia, estimated glomerular filtration rate (GFR), and in addition GOLD grade. We additionally tested for collinearity in the multivariate model using the variance inflation factor. Moreover, the calibration of the Cox model was assessed using the Grønnesby and Borgan statistics [20], comparing the observed and model-based estimated expected number of events within five risk groups. First-degree interaction was tested using interaction terms between the COPD and all variables included in the confounder model. Kaplan–Meier analysis was applied to evaluate the effect of COPD on survival and compared using log-rank test. Two-sided p values less than 0.05 were used to indicate statistical significance. SPSS 17.0 (SPSS/IBM) was used for all analyses.
Results
We prospectively included 191 patients with a median age of 62 years (IQR 51–69) undergoing ECMO following cardiovascular surgery between February 2002 and December 2009. Seventy-one percent of patients were male. Fifty-six patients underwent valve surgery, 26 coronary artery bypass graft (CABG) surgery, 38 combined CABG and valve surgery, 39 cardiac transplantation, and 32 other cardiovascular surgeries. The median SAPS II score and median EuroSCORE of the study population were 44 (IQR 31–60) and 10 (6–13), respectively. In total 125 patients (65 %) died; 88 % of fatal events were due to cardiovascular causes. The median duration of ECMO therapy was 4 days (IQR 2–6 days) and the median time on mechanical ventilation was 11 days (IQR 4–19 days). ECMO support following cardiovascular surgery was initiated because of weaning failure from cardiopulmonary bypass (58 %), postoperative cardiogenic shock (25 %), immediate post-transplant cardiac graft failure (6 %), postoperative respiratory failure (2 %), postoperative bleeding/tamponade with cardiogenic shock (7 %), and miscellaneous conditions (3 %; Supplemental Table 1). Detailed baseline characteristics are displayed in Table 1. Furthermore, a comparison of all baseline characteristics comparing survivors versus non-survivors is presented in Supplemental Table 1.
Thirty-five patients (18 %) had diagnosed COPD. Of these 4 (11 %) were classified as GOLD I, 21 (60 %) as GOLD II, 8 (23 %) as GOLD III, and 2 (6 %) as GOLD IV. There were no significant differences between patients with and without COPD (Table 1) except for age (p < 0.01) and EuroSCORE (p = 0.04). However, after exclusion of chronic pulmonary disease from the EuroSCORE calculation, patients with and without COPD did not significantly differ (p = 0.31). The median follow-up time was 51 months (IQR 34–71 months) corresponding to 4,197 overall months of follow-up.
Survival analysis
We detected a significant adverse effect of COPD on all-cause mortality with an unadjusted hazard ratio (HR) of 1.74 (95 % CI 1.16–2.63, p = 0.01) and cardiovascular mortality with an unadjusted HR of 1.93 (95 % CI 1.26–2.96, p < 0.01). The results persisted after multivariate adjustment with an adjusted HR of 1.62 (95 % CI 1.06–2.50, p = 0.03) for all cause mortality and an adjusted HR of 1.73 (95 % CI 1.11–2.70, p = 0.02) for cardiovascular mortality. The effect was more pronounced after additional adjustment for GOLD grade with an HR of 4.22 (95 % CI 1.04–17.11, p = 0.04) for all-cause mortality and an HR of 5.87 (95 % CI 1.41–24.47, p = 0.02) for cardiovascular mortality. There was no significant impact of COPD on all-cause and cardiovascular mortality 30 days after ICU admission (p = 0.09 and p = 0.07, respectively). Furthermore, there was no significant interaction between COPD and any variable in the multivariate confounder model (data not shown). Additionally, we could not detect a significant collinearity and the p values for the Grønnesby and Borgan statistics indicated good calibration for our multivariate models (data not shown).
Kaplan–Meier analysis revealed a significant increase of all-cause mortality (p = 0.007, log-rank test; Fig. 1a) and cardiovascular mortality (p = 0.002, log-rank test; Fig. 1c) in patients with COPD. Long-term survival was decreased in patients with COPD after 1 year (23 % vs. 44 %) and after 6 years (14 % vs. 35 %) compared to patients without COPD. A similar trend was observed for cardiovascular survival. When Kaplan–Meier analysis was repeated for 30-day survivors, a similar difference between patients with and without COPD was observed for all-cause (p = 0.02, log-rank test; Fig. 1b) and cardiovascular mortality (p = 0.004, log-rank test; Fig. 1d).

Kaplan–Meier estimates of mortality—Kaplan–Meier estimates for all patients (a, c) and 30-day survivors (b, d) with and without COPD for all-cause mortality (a p = 0.007; b p = 0.02, log rank test) and cardiovascular mortality (c p = 0.002; d p = 0.004, log rank test)
Discussion
This is the first study to identify COPD as an independent predictor of long-term all-cause mortality and cardiovascular mortality in patients undergoing veno-arterial ECMO support following cardiovascular surgery. These associations persisted after adjustment for potential confounders and were even more pronounced after adjustment for GOLD grade. Interestingly, there was no significant impact of COPD on all-cause and cardiovascular mortality 30 days after ICU admission.
ECMO support following cardiovascular surgery is characterized by a high initial mortality rate ranging from 25 to 44 % [3, 4], which is in accordance with our 30-day mortality of 42 %. Therefore, previous studies predominantly focused on prediction and improvement of in-hospital mortality [3]. While the thereby identified risk factors are crucial for risk estimation of short-term mortality, different variables might become operative to estimate long-term outcome in patients undergoing ECMO support. Our results emphasize a clinically significant and independent impact of COPD on long-term survival in this carefully selected patient population. Interestingly, in agreement with results presented by Rastan et al. [3], COPD did not affect 30-day mortality, further suggesting that distinct differences seem to be relevant to determine long-term survival of patients undergoing ECMO therapy. A large prospective study by Funk et al. further strengthens this observation for COPD. The authors evidently established COPD as an independent risk factor for increased mortality in an unselected ICU population, whereas the presented mortality curves do not seem to indicate a significant difference in death within the first week of ICU admission between patients with and without COPD [9]. Furthermore, Angouras et al. demonstrated in a study population of patients undergoing CABG a significant association between COPD and long-term mortality over a median follow-up of 7 years with a crude HR of 1.28 (95 % CI 1.11–1.47) [5]. These long-term results were further underlined by a large prospective study population of 13,337 consecutive CABG patients with a crude HR of 1.29 (95 % CI 1.14–1.46) over a similar follow-up [6]. Our results extend the previous knowledge and demonstrate an approximately fourfold higher mortality risk for COPD patients in a highly selected population of long-term ECMO survivors after cardiovascular surgery. Notably, the present study indicates that COPD is not only associated with all-cause mortality but especially with cardiovascular mortality. This observation is in line with previous data reporting a higher risk of long-term cardiovascular mortality in COPD patients with ischemic heart disease undergoing percutaneous coronary intervention (PCI) or CABG [21, 22]. Generally, there is strong evidence that COPD is associated with increased risk of cardiovascular events [23, 24]. A recently published study suggested the impairment of endothelial function as potential underlying mechanism linking COPD and cardiovascular death [25]. Hypercapnia has been identified as a crucial factor impairing endothelial function in COPD patients [25]. It is rather speculative that appropriate carbon dioxide removal, which is mostly achieved by ECMO support and mechanical ventilation during ICU stay, might explain the delayed negative effect of COPD on outcome. The crucial effect of COPD on long-term outcome is in accord with a recently published study that demonstrated a higher incidence of hospital readmissions for recurrent myocardial infarction, heart failure, and serious bleeding events in ischemic heart disease patients with concomitant COPD [22]. A prothrombotic state in patients with COPD [18, 19] might represent a potential pathophysiological link between COPD and cardiovascular disease.
COPD has been well established as independent risk factor for mortality after cardiovascular surgery [7, 8, 26, 27]. Gupta et al. demonstrated in a large postoperative study population of 478,795 patients a significantly higher 30-day mortality in patients with COPD [28]. In particular, respiratory failure is a severe and common short-term complication in COPD patients after cardiac operations [29], which is associated with poor outcome [30, 31]. Therefore, COPD patients might initially benefit from ECMO support because of improved blood oxygenation virtually independent of the respiratory system. This temporary profit might be reflected in the current study by similar short-term mortality rates between patients with and without COPD. It is tempting to speculate that ECMO support only temporarily mitigates the high risk of COPD patients after cardiovascular surgery. A variety of reasons for the association of COPD with increased long-term mortality have been previously discussed ranging from impaired respiratory mechanics and reduced respiratory muscle capacity after cardiopulmonary support to an increased incidence of ventilator-associated pneumonia [9]. Nevertheless, the exact mechanism of increased long-term mortality in COPD patients following ECMO support still remains unknown.
Clinical implications
Knowledge of adverse long-term predictors such as COPD is a valuable addition for a comprehensive decision-making prior to ECMO implantation, because unrestrained use of ECMO might disproportionately increase hospital costs and resources consumption. Therefore, our results suggest that initiation of ECMO therapy in COPD patients, in the presence of other significant risk factors, should be carefully balanced against the poor outcome.
Furthermore, identification of long-term risk factors may help to detect high-risk patients following ECMO therapy. These patients may benefit from an intensified treatment of co-morbidities and close check-ups after hospital discharge, especially because previous reports indicate an otherwise satisfactory mental health and vitality in long-term survivors following ECMO therapy [2].
Limitations
One potential limitation of our study is that our data reflect the experience of a single center. In addition, although our number of long-term survivors and median follow-up evaluated is among the highest reported to date, it might still not be satisfactory to draw definitive conclusions about COPD long-term outcome. Another potential limitation is that COPD patients were significantly older than patients without COPD. Nevertheless, our results were even more pronounced after adjustment for age in the multivariate model. Moreover, other oxygenators (e.g., polymethylpentene oxygenators) demonstrated less pro-inflammatory effects, improved gas exchange capabilities, and reduced transfusion requirements compared to microporous oxygenators [32–34], which were used in the presented study. However, during the observation period of our study microporous oxygenators were widely used in clinical practice [3, 35–38]. Finally, the diagnosis of COPD was based on previous medical reports. A systematic diagnostic work-up, including spirometry in survivors, would have been desirable.
Conclusion
We identified COPD as a strong and independent predictor of long-term all-cause mortality and cardiovascular mortality in patients undergoing veno-arterial ECMO therapy following cardiovascular surgery. The current study advances the limited knowledge on long-term risk prediction in ECMO patients and represents a valuable addition for a comprehensive decision-making prior to ECMO implantation. Nevertheless, the pathophysiological mechanisms underlying these associations and the potential for risk modification through intensified measures of secondary prevention have to be further elucidated.
References
Bartlett RH, Roloff DW, Custer JR, Younger JG, Hirschl RB (2000) Extracorporeal life support: the University of Michigan experience. JAMA 283:904–908
Combes A, Leprince P, Luyt CE, Bonnet N, Trouillet JL, Leger P, Pavie A, Chastre J (2008) Outcomes and long-term quality-of-life of patients supported by extracorporeal membrane oxygenation for refractory cardiogenic shock. Crit Care Med 36:1404–1411
Rastan AJ, Dege A, Mohr M, Doll N, Falk V, Walther T, Mohr FW (2010) Early and late outcomes of 517 consecutive adult patients treated with extracorporeal membrane oxygenation for refractory postcardiotomy cardiogenic shock. J Thorac Cardiovasc Surg 139:302–311, e1
Smedira NG, Blackstone EH (2001) Postcardiotomy mechanical support: risk factors and outcomes. Ann Thorac Surg 71:S60–S66 (discussion S82–65)
Angouras DC, Anagnostopoulos CE, Chamogeorgakis TP, Rokkas CK, Swistel DG, Connery CP, Toumpoulis IK (2010) Postoperative and long-term outcome of patients with chronic obstructive pulmonary disease undergoing coronary artery bypass grafting. Ann Thorac Surg 89:1112–1118
O’Boyle F, Mediratta N, Chalmers J, Al-Rawi O, Mohan K, Shaw M, Poullis M (2013) Long-term survival of patients with pulmonary disease undergoing coronary artery bypass surgery. Eur J Cardiothorac Surg 43:697–703
Rady MY, Ryan T (1999) Perioperative predictors of extubation failure and the effect on clinical outcome after cardiac surgery. Crit Care Med 27:340–347
Samuels LE, Kaufman MS, Morris RJ, Promisloff R, Brockman SK (1998) Coronary artery bypass grafting in patients with COPD. Chest 113:878–882
Funk GC, Bauer P, Burghuber OC, Fazekas A, Hartl S, Hochrieser H, Schmutz R, Metnitz P (2012) Prevalence and prognosis of chronic obstructive pulmonary disease in critically ill patients between 1998 and 2008. Eur Respir J 41:792–799
Sellares J, Ferrer M, Cano E, Loureiro H, Valencia M, Torres A (2011) Predictors of prolonged weaning and survival during ventilator weaning in a respiratory ICU. Intensive Care Med 37:775–784
Vestbo J, Hurd SS, Agusti AG, Jones PW, Vogelmeier C, Anzueto A, Barnes PJ, Fabbri LM, Martinez FJ, Nishimura M, Stockley RA, Sin DD, Rodriguez-Roisin R (2013) Global Strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease, GOLD executive summary. Am J Respir Crit Care Med 187:347–365
MacLaren G, Combes A, Bartlett RH (2012) Contemporary extracorporeal membrane oxygenation for adult respiratory failure: life support in the new era. Intensive Care Med 38:210–220
Peek GJ, Mugford M, Tiruvoipati R, Wilson A, Allen E, Thalanany MM, Hibbert CL, Truesdale A, Clemens F, Cooper N, Firmin RK, Elbourne D (2009) Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet 374:1351–1363
The Acute Respiratory Distress Syndrome Network (2000) Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 342:1301–1308
Gattinoni L, Pesenti A, Mascheroni D, Marcolin R, Fumagalli R, Rossi F, Iapichino G, Romagnoli G, Uziel L, Agostoni A et al (1986) Low-frequency positive-pressure ventilation with extracorporeal CO2 removal in severe acute respiratory failure. JAMA 256:881–886
Antonelli M, Bonten M, Cecconi M, Chastre J, Citerio G, Conti G, Curtis JR, Hedenstierna G, Joannidis M, Macrae D, Maggiore SM, Mancebo J, Mebazaa A, Preiser JC, Rocco P, Timsit JF, Wernerman J, Zhang H (2013) Year in review in Intensive Care Medicine 2012: III. Noninvasive ventilation, monitoring and patient-ventilator interactions, acute respiratory distress syndrome, sedation, paediatrics and miscellanea. Intensive Care Med 39:543–557
Aissaoui N, Luyt CE, Leprince P, Trouillet JL, Leger P, Pavie A, Diebold B, Chastre J, Combes A (2011) Predictors of successful extracorporeal membrane oxygenation (ECMO) weaning after assistance for refractory cardiogenic shock. Intensive Care Med 37:1738–1745
Roques F, Nashef SA, Michel P, Gauducheau E, de Vincentiis C, Baudet E, Cortina J, David M, Faichney A, Gabrielle F, Gams E, Harjula A, Jones MT, Pintor PP, Salamon R, Thulin L (1999) Risk factors and outcome in European cardiac surgery: analysis of the EuroSCORE multinational database of 19030 patients. Eur J Cardiothorac Surg 15:816–822 (discussion 822–813)
Le Gall JR, Lemeshow S, Saulnier F (1993) A new simplified acute physiology score (SAPS II) based on a European/North American multicenter study. JAMA 270:2957–2963
Grønnesby JK, Borgan O (1996) A method for checking regression models in survival analysis based on the risk score. Lifetime Data Anal 2:315–328
Nishiyama K, Morimoto T, Furukawa Y, Nakagawa Y, Ehara N, Taniguchi R, Ozasa N, Saito N, Hoshino K, Touma M, Tamura T, Haruna Y, Shizuta S, Doi T, Fukushima M, Kita T, Kimura T (2010) Chronic obstructive pulmonary disease–an independent risk factor for long-term cardiac and cardiovascular mortality in patients with ischemic heart disease. Int J Cardiol 143:178–183
Campo G, Guastaroba P, Marzocchi A, Santarelli A, Varani E, Vignali L, Sangiorgio P, Tondi S, Serenelli C, De Palma R, Saia F (2013) Impact of chronic obstructive pulmonary disease on long-term outcome after ST-segment elevation myocardial Infarction receiving primary percutaneous coronary intervention. Chest. doi:10.1378/chest.12-2313
Engstrom G, Melander O, Hedblad B (2010) Population-based study of lung function and incidence of heart failure hospitalisations. Thorax 65:633–638
Sin DD, Wu L, Man SF (2005) The relationship between reduced lung function and cardiovascular mortality: a population-based study and a systematic review of the literature. Chest 127:1952–1959
Clarenbach CF, Senn O, Sievi NA, Camen G, van Gestel AJ, Rossi VA, Puhan MA, Thurnheer R, Russi EW, Kohler M (2013) Determinants of endothelial function in patients with COPD. Eur Respir J (in press)
Farooq V, Serruys PW, Bourantas C, Vranckx P, Diletti R, Garcia Garcia HM, Holmes DR, Kappetein AP, Mack M, Feldman T, Morice MC, Colombo A, Morel MA, de Vries T, van Es GA, Steyerberg EW, Dawkins KD, Mohr FW, James S, Stahle E (2012) Incidence and multivariable correlates of long-term mortality in patients treated with surgical or percutaneous revascularization in the Synergy between Percutaneous Coronary Intervention with Taxus and Cardiac Surgery (SYNTAX) trial. Eur Heart J 33:3105–3113
Wu C, Camacho FT, Wechsler AS, Lahey S, Culliford AT, Jordan D, Gold JP, Higgins RS, Smith CR, Hannan EL (2012) Risk score for predicting long-term mortality after coronary artery bypass graft surgery. Circulation 125:2423–2430
Gupta H, Ramanan B, Gupta PK, Fang X, Polich A, Modrykamien A, Schuller D, Morrow LE (2013) Impact of chronic obstructive pulmonary disease on postoperative outcomes: results from a national database. Chest. doi:10.1378/chest.12-1499
Bailey ML, Richter SM, Mullany DV, Tesar PJ, Fraser JF (2011) Risk factors and survival in patients with respiratory failure after cardiac operations. Ann Thorac Surg 92:1573–1579
Filsoufi F, Rahmanian PB, Castillo JG, Chikwe J, Adams DH (2008) Predictors and early and late outcomes of respiratory failure in contemporary cardiac surgery. Chest 133:713–721
Hein OV, Birnbaum J, Wernecke KD, Konertz W, Jain U, Spies C (2006) Three-year survival after four major post-cardiac operative complications. Crit Care Med 34:2729–2737
Peek GJ, Killer HM, Reeves R, Sosnowski AW, Firmin RK (2002) Early experience with a polymethyl pentene oxygenator for adult extracorporeal life support. ASAIO J 48:480–482
Khoshbin E, Dux AE, Killer H, Sosnowski AW, Firmin RK, Peek GJ (2007) A comparison of radiographic signs of pulmonary inflammation during ECMO between silicon and poly-methyl pentene oxygenators. Perfusion 22:15–21
Khoshbin E, Roberts N, Harvey C, Machin D, Killer H, Peek GJ, Sosnowski AW, Firmin RK (2005) Poly-methyl pentene oxygenators have improved gas exchange capability and reduced transfusion requirements in adult extracorporeal membrane oxygenation. ASAIO J 51:281–287
Chen YS, Lin JW, Yu HY, Ko WJ, Jerng JS, Chang WT, Chen WJ, Huang SC, Chi NH, Wang CH, Chen LC, Tsai PR, Wang SS, Hwang JJ, Lin FY (2008) Cardiopulmonary resuscitation with assisted extracorporeal life-support versus conventional cardiopulmonary resuscitation in adults with in-hospital cardiac arrest: an observational study and propensity analysis. Lancet 372:554–561
Morris MC, Ittenbach RF, Godinez RI, Portnoy JD, Tabbutt S, Hanna BD, Hoffman TM, Gaynor JW, Connelly JT, Helfaer MA, Spray TL, Wernovsky G (2004) Risk factors for mortality in 137 pediatric cardiac intensive care unit patients managed with extracorporeal membrane oxygenation. Crit Care Med 32:1061–1069
Jan SL, Lin SJ, Fu YC, Chi CS, Wang CC, Wei HJ, Chang Y, Hwang B, Chen PY, Huang FL, Lin MC (2010) Extracorporeal life support for treatment of children with enterovirus 71 infection-related cardiopulmonary failure. Intensive Care Med 36:520–527
Schmidt M, Tachon G, Devilliers C, Muller G, Hekimian G, Brechot N, Merceron S, Luyt CE, Trouillet JL, Chastre J, Leprince P, Combes A (2013) Blood oxygenation and decarboxylation determinants during venovenous ECMO for respiratory failure in adults. Intensive Care Med 39:838–846
Acknowledgments
Georg Goliasch was supported by an Erwin Schrödinger Fellowship of the Austrian Science Fund (FWF J 3319-B13).
Conflicts of interest
No conflict of interest exists for the author.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Distelmaier, K., Niessner, A., Haider, D. et al. Long-term mortality in patients with chronic obstructive pulmonary disease following extracorporeal membrane oxygenation for cardiac assist after cardiovascular surgery. Intensive Care Med 39, 1444–1451 (2013). https://doi.org/10.1007/s00134-013-2931-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-013-2931-y