
Abstract
Purpose
Early lung recruitment (ELR) during high-frequency oscillatory ventilation (HFOV) in combination with prophylactic surfactant use has been reported to reduce mortality, improve respiratory outcomes, and reduce the need for repeated surfactant dosing, suggesting that surfactant might be used more selectively in very low birth weight (VLBW) infants on HFOV than generally recommended. We report our first experience from such a selective early rescue use of surfactant in VLBW infants on HFOV.
Methods
After a deliberate ELR maneuver and “optimal” continuous distending pressure (CDP) finding during HFOV, used as primary ventilation mode for VLBW infants with respiratory distress syndrome (RDS), surfactant was only given when an unsatisfactory oxygenation response to lung recruitment (as defined by CDP × FiO2 > 5) was observed.
Results
Out of 144 VLBW infants on HFOV, 84 (58.3%) received surfactant and 60 (41.7%) did not. Duration of required oxygen supplementation (37.4 ± 44.9 vs. 46.2 ± 35.4 days; P = 0.031) and respiratory support (i.e., n-CPAP and/or mechanical ventilation; 22.3 ± 19.3 vs. 38.2 ± 24.3 days; P = 0.001) was shorter for infants who did not receive surfactant than for those who did. The incidence and severity of bronchopulmonary dysplasia was similar in both groups, and there was no difference in survival rates between groups. Subgroup analysis for infants of less than 28 weeks of gestation revealed similar results.
Conclusions
First intention HFOV combined with an early attempt at lung volume optimization might allow surfactants to be used more selectively (in relation to disease severity) in VLBW infants presenting with RDS at birth without negatively influencing the outcome.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
There is growing evidence that the ventilator strategy used during mechanical ventilation may influence pulmonary outcome in preterm infants with respiratory distress syndrome (RDS). Several reports of early lung recruitment (ELR) during high-frequency oscillatory ventilation (HFOV) suggest a benefit of such a strategy in terms of improving pulmonary outcome [i.e., occurrence of bronchopulmonary dysplasia (BPD), oxygen dependency, and duration of ventilation] in preterm infants with RDS [1–3]. However, with the increasing use of lung-protective ventilator strategies during conventional mechanical ventilation (CMV), the benefit of HFOV is not as clear-cut [4, 5]. During the transition towards more gentle (e.g., lung-protective) ventilation over the last years, indications for surfactant that were established almost 2 decades ago might need to be rethought based on some clinical and experimental observations. Accordingly, systematic prophylactic surfactant administration has been challenged recently, considering that it exposes to intubation and ventilation some premature infants who might be managed perfectly on nasal continuous positive airway pressure (n-CPAP) [6]. Furthermore, Moriette and colleagues [7] have demonstrated a reduction in the need for supplemental surfactant doses when HFOV combined with an open-lung strategy was used. Similarly, Vento et al., in a recent randomized trial, showed that early and exclusive use of HFOV combined with optimum volume strategy allowed for early and sustained improvement in pulmonary mechanics and gas exchange with earlier extubation as compared to neonates assigned to CMV treatment and reduced the need in the HFOV group for a second surfactant dose [8]. In experimental settings, lung-protective ventilation strategies seem to preserve surfactant activity better than injurious ventilation strategies [9–11]. Based on these observations, it might be justified to question the commonly accepted indications for surfactant treatment when HFOV combined with an ELR approach is initiated immediately after intubation in preterm infants presenting with RDS at birth. We report our experience and outcome data over a 9 year observation period with a restricted selective use of surfactant in this patient population.
Materials and methods
Patients
Over a 9-year observational period, all consecutively admitted inborn neonates with a gestational age <32 weeks and a birth weight <1,500 g who developed early RDS (within the first 24 h of life) requiring mechanical ventilation were identified from a prospectively maintained database. Indication for tracheal intubation was decided based on clinical criteria [i.e., persisting severe respiratory distress with CO2 retention >8 kPa (60 mmHg) and/or oxygen requirement (FiO2) >0.5 while on n-CPAP, irrespective of the timing of intubation]. While on n-CPAP, positive pressure level was set between 4 and 8 cm H2O according the attending physician’s decision. Our target tSO2 for O2 supplementation was 88–92%, accepting a minimum of 85% over short periods. Neonates with hydrops fetalis, congenital lung and heart malformations, chromosomopathies, or congenital diaphragmatic hernia were excluded from analysis. For analysis, patients were subdivided into those who received surfactant therapy and those who did not.
The HFOV-based ventilator strategy has been our primary ventilatory mode for premature infants presenting with RDS since 1997 and was established as such by a consensus agreement among staff physicians [3]. Detailed treatment strategies can be found in the Electronic Supplementary Material.
Data collection
Demographic data, ventilator parameters, gas exchange, and outcome variables were collected for each patient by chart review. Uniformity between groups was evaluated based on gestational age, birth weight, the use of antenatal steroids, and Apgar scores at 1 and 5 min.
Endpoints
The following primary endpoints were evaluated for differences in morbidity and outcome between the two groups: (1) length of mechanical ventilation and total time of respiratory support, including n-CPAP (days), (2) length of supplemental oxygen requirements (days), (3) occurrence of mild, moderate, and severe BPD [12], and (4) survival. Survival was assessed at 30 days, 36 weeks PMA, and at discharge. Combined mortality including death and occurrence of severe BPD was also assessed. Secondary endpoints for assessment of possible adverse effects were (1) intraventricular hemorrhage, (2) air leak syndrome (pneumothorax, pulmonary interstitial emphysema), (3) sepsis and necrotizing enterocolitis, and (4) occurrence of a hemodynamically significant patent ductus arteriosus (hsPDAS, always confirmed by echocardiography).
Statistical analysis
Continuous data were expressed as mean ± standard deviation (SD). A two-tailed Fishers’ exact test was used for categorial data. Nonparametric Mann-Whitney U test was used for continuous data. For all testing, a P value <0.05 was accepted as significant. Statistical analysis was performed using a Systat 10.0, SPSS package.
Results
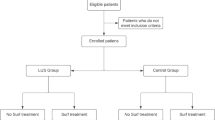
Between 1 January 1997 and 31 December 2005, 620 very low birth weight (VLBW) infants were delivered in our institution (Fig. 1). Among those, 144 infants [including 96 (67%) with a gestational age of less than 28 weeks] presenting with early RDS as a primary diagnosis required invasive mechanical ventilation: 93 (64.7%) were intubated in the delivery room after failing an initial n-CPAP trial (delay to intubation: 0.99 ± 2.7 h), and 51 infants (35.3%) were intubated later on while failing n-CPAP (delay to intubation: 18.8 ± 14.9 h) (P < 0.001). After intubation, all infants were put in a first intention on HFOV [1–3]. After an initial lung recruitment procedure on HFOV, 84 infants (58.3%) received selective early rescue surfactant therapy according to our criteria (i.e., CDP × FiO2 > 5) and the other 60 infants (41.7%) with a CDP × FiO2 ≤ 5 did not receive surfactant. Fifty-seven (67.8%) of these 84 infants treated with surfactant received Curosurf, while the remaining had Exosurf (n = 27, 31.4%). Whereas no statistical differences in most respiratory outcomes were found between the two surfactant types in treated infants, oxygen dependency was shorter in infants who received Exosurf than Curosurf (21.4 ± 23 vs. 39.5 ± 37 days; P = 0.024). Between the two groups (surfactant vs. no surfactant), no differences were noted in demographic data (gestational age, birth weight, and gender), incidence of prenatal steroid treatment, or low Apgar score at 1 and 5 min (Table 1). n-CPAP as a first respiratory support option (i.e., no intubation in the labor room) was more often used in the group of patients who, according to our criteria, would later require early rescue surfactant (36/84 vs. 15/60; P = 0.034). Overall mean time delay of intubation after delivery between the surfactant and the no-surfactant group was longer in patients who did receive surfactant than in those who did not (9.8 ± 13.4 vs. 6.4 ± 12.5 h; P = 0.01). Both observations suggest a higher need for early rescue surfactant when n-CPAP was used in a first intention in order to avoid intubation (OR 2.25, 95% CI 1.09–4.65; P = 0.042).

Studied population. VLBW Very low birth weight, RDS respiratory distress syndrome, nCPAP nasal continuous positive airway pressure, HFOV high-frequency oscillatory ventilation
Outcome
Detailed pulmonary outcome data in survivors are given in Table 2. Both overall respiratory support and oxygen dependency were shorter in patients who did not receive surfactant, whereas overall duration on mechanical ventilation was not different between groups. No statistically significant difference was found between groups for the incidence of mild, moderate, and severe BPD, although a trend could be observed in favor of the no-surfactant group. There were no differences between the groups in the incidence of mild or severe intraventricular hemorrhage (IVH), pulmonary air leaks, necrotizing enterocolitis, or sepsis (Table 3). However, hsPDA was observed less often in patients who received no surfactant than in those who received surfactant (58.3 vs. 78.6%; P = 0.01). Survival was similar in both groups as well as in the combined outcome (Table 4). The cause of death in the four patients who died between 30 days and discharge was multiorgan failure related to septic shock in three cases and Intraventricular hemorrhage (IVH) grade 4 in one. All four patients had been weaned from HFOV and were on n-CPAP before the acute event that led them to the dismal outcome occurred.
In infants of <28 weeks of gestational age, 57 (59%) received surfactant. Patient’s characteristics were similar between both groups. Delay of intubation was shorter in patients without surfactant (5.8 ± 12.1 vs. 9.3 ± 13.9 h; P = 0.048). More hsPDA occurred in patients who received surfactant than in others. No other outcome criterion was found to be significantly different between the two groups (Table 5).
Discussion
Our results suggest that when an ELR strategy is used successfully in conjunction with HFOV, prophylactic surfactant treatment might not be systematically required in VLBW infants presenting with RDS at birth. Indeed, not using surfactant in every VLBW case—even for infants of less than 28 weeks of gestational age presenting with RDS at birth who needed mechanical ventilation and were ventilated with HFOV—did not negatively affect respiratory outcome or mortality in our patient collective.
The decision to administer surfactant was based on disease severity as assessed by the continuous distending pressure (CDP) required after a formal RM attempt to achieve a specific oxygenation goal at a relatively low CDP while on low oxygen concentration (i.e., CDP × FiO2 ≤ 5) [13]. The rationale behind this approach is that (1) an easily recruitable lung in the early stage of RDS may not need exogenous surfactant treatment for sufficient lung opening, and (2) gentle ventilation in an “open lung” may preserve surfactant function by avoiding a major inflammatory stimulus within the lungs, as suggested by experimental data [14–19]. Van Kaam and co-workers [20] have shown in an animal model of neonatal lung injury that using an open-lung strategy during both HFOV or CMV performed better in regards to dose-dependent efficacy of surfactant with less surfactant inactivation than CMV without applying an open-lung strategy. Similarly, Hilgendorff et al. [21] in an animal model showed that open-lung ventilation alone did better than surfactant and conventional ventilation. Human data confirmed the efficacy of HFOV recruitment maneuver in improving both functional lung capacity [22, 23] and inflammatory lung profiles [24, 25]. Furthermore, in two recent randomized controlled trials comparing HFO with CMV [7, 8], ELR during HFOV allowed the number of repeated surfactant doses in VLBW infants with RDS to be reduced compared to infants assigned to conventional ventilation who were not submitted to a lung recruitment attempt.
Besides appropriate lung recruitment, the timing of HFOV initiation seems to influence outcome too. Using ELR with HFOV compared to CMV in a recent randomized trial in VLBW infants with RDS demonstrated an early and sustained improvement in pulmonary mechanics and gas exchange, as well as a significant trend towards a reduced oxygen dependency at 36 weeks PMA [8]. Similarly, Mehta et al. [26] and Derdak et al. [27] in adult patients and Fedora et al. [28] in children with acute RDS showed better survival in patients who were switched from CMV to HFOV early in the course of disease when compared to those that were switched to HFOV after several days of CMV. These observations suggest that prolonged ventilation with a potentially injurious ventilatory strategy may aggravate lung injury and alter efficiency of subsequent therapy. Similarly, in our series, lung recruitment became more difficult in infants who were initially put on n-CPAP for a prolonged time before intubating and initiating HFOV, as illustrated by the increased use of surfactant, indicating that lung injury might worsen during prolonged n-CPAP application in babies presenting with an important RDS. Accordingly, some recent papers strongly suggest that lung injury can be initiated or worsened not only by positive pressure ventilation but also during spontaneous breathing [29, 30].
In our patient series, a more restrictive use of surfactant after ELR was significantly associated with a lower incidence of hsPDA (OR 5.91, 95% CI 1.26–5.44; P = 0.015). Several authors identified hsPDA as a major risk factor for the development of chronic lung disease [31–34]. Recently, Noori et al. showed that hsPDA (hazard ratio 8.34; 95% CI 4.30–16.06) is associated with increased mortality in VLBW infants of <28 weeks of gestational age [35]. However, it is not clear whether surfactant therapy has an impact on the development of hsPDA [36, 37].
Some limitations of our study should be mentioned. First, interpretation of our results is limited by the cohort study design and a selection bias: only VLBW infants with early RDS (<24 h) were included, representing 23% of the 620 VLBW infants delivered in our institution over the same time period. Furthermore, surfactant was administered only on a selective basis as an “early rescue therapy” in patients who failed to be efficiently recruited according to our criteria (CDP × FiO2 ≤ 5 after RM). As a result, surfactant was used in the most severe cases (i.e., in those who were not recruitable according our criteria) with an early rescue approach. It could be argued that administering surfactant to all patients independent of their response to recruitment—which would correspond to a much more prophylactic approach—might have improved our good outcome results still further. On the other hand, the more restrictive use of surfactant we describe may have a substantial economic impact due to the reduction of direct cost for surfactant preparation and potential indirect cost for medical and surgical PDA closure procedures.
In summary, our outcome data show that implementation of an ELR strategy with HFOV allows for a selective use of surfactant based on the oxygenation response after lung recruitment during HFOV, with no detrimental effect on respiratory outcomes and mortality in VLBW infants presenting with RDS. Although one should consider that our patients can be divided into two groups by disease severity with the less sick patients showing better outcome independent of surfactant treatment, three important issues will need further assessment in well designed controlled clinical trials: (1) Does the use of an ELR during HFOV, as a lung-protective strategy, really allow exogenous surfactants to be used more selectively in VLBW infants with RDS without negatively affecting respiratory outcome or survival? (2) Does delaying intubation in a subgroup of infants who require intubation eventually negatively affect outcome? (3) Does initial n-CPAP in VLBW infants with RDS hamper secondary lung recruitment with HFOV?
The commonly accepted surfactant indications that were established years ago might need to be reviewed within the context of recently established lung-protective ventilation strategies, thereby providing the rationale for a well-designed randomized trial.
References
Gerstmann DR, Minton SD, Stoddard RA, Meredith KS, Monaco F, Bertrand JM, Battisti O, Langhendries JP, Francois A, Clark RH (1996) The Provo multicenter early high-frequency oscillatory ventilation trial: improved pulmonary and clinical outcome in respiratory distress syndrome. Pediatrics 98:1044–1057
Courtney SE, Durand DJ, Asselin JM, Hudak ML, Aschner JL, Shoemaker CT (2002) High-frequency oscillatory ventilation versus conventional mechanical ventilation for very-low-birth-weight infants. N Engl J Med 347:643–652
Rimensberger PC, Beghetti M, Hanquinet S, Berner M (2000) First intention high-frequency oscillation with early lung volume optimization improves pulmonary outcome in very low birth weight infants with respiratory distress syndrome. Pediatrics 105:1202–1208
Bollen CW, Uiterwaal CS, van Vught AJ (2003) Cumulative metaanalysis of high-frequency versus conventional ventilation in premature neonates. Am J Respir Crit Care Med 168:1150–1155
van Kaam AH, Rimensberger PC (2007) Lung-protective ventilation strategies in neonatology: what do we know—what do we need to know? Crit Care Med 35:925–931
Sweet DG, Halliday HL (2009) The use of surfactants in 2009. Arch Dis Child Educ Pract Ed 94:78–83
Moriette G, Paris-Llado J, Walti H, Escande B, Magny JF, Cambonie G, Thiriez G, Cantagrel S, Lacaze-Masmonteil T, Storme L, Blanc T, Liet JM, Andre C, Salanave B, Breart G (2001) Prospective randomized multicenter comparison of high-frequency oscillatory ventilation and conventional ventilation in preterm infants of less than 30 weeks with respiratory distress syndrome. Pediatrics 107:363–372
Vento G, Matassa PG, Ameglio F, Capoluongo E, Zecca E, Tortorolo L, Martelli M, Romagnoli C (2005) HFOV in premature neonates: effects on pulmonary mechanics and epithelial lining fluid cytokines. A randomized controlled trial. Intensive Care Med 31:463–470
Ito Y, Veldhuizen RA, Yao LJ, McCaig LA, Bartlett AJ, Lewis JF (1997) Ventilation strategies affect surfactant aggregate conversion in acute lung injury. Am J Respir Crit Care Med 155:493–499
Veldhuizen RA, Tremblay LN, Govindarajan A, van Rozendaal BA, Haagsman HP, Slutsky AS (2000) Pulmonary surfactant is altered during mechanical ventilation of isolated rat lung. Crit Care Med 28:2545–2551
Veldhuizen RA, Welk B, Harbottle R, Hearn S, Nag K, Petersen N, Possmayer F (2002) Mechanical ventilation of isolated rat lungs changes the structure and biophysical properties of surfactant. J Appl Physiol 92:1169–1175
Jobe AH, Bancalari E (2001) Bronchopulmonary dysplasia. Am J Respir Crit Care Med 163:1723–1729
Kalenga M, Battisti O, Francois A, Langhendries JP, Gerstmann DR, Bertrand JM (1998) High-frequency oscillatory ventilation in neonatal RDS: initial volume optimization and respiratory mechanics. J Appl Physiol 84:1174–1177
Rimensberger PC, Cox PN, Frndova H, Bryan AC (1999) The open lung during small tidal volume ventilation: concepts of recruitment and “optimal” positive end-expiratory pressure. Crit Care Med 27:1946–1952
Rimensberger PC, Pache JC, McKerlie C, Frndova H, Cox PN (2000) Lung recruitment and lung volume maintenance: a strategy for improving oxygenation and preventing lung injury during both conventional mechanical ventilation and high-frequency oscillation. Intensive Care Med 26:745–755
Vazquez de Anda GF, Hartog A, Verbrugge SJ, Gommers D, Lachmann B (1999) The open lung concept: pressure-controlled ventilation is as effective as high-frequency oscillatory ventilation in improving gas exchange and lung mechanics in surfactant-deficient animals. Intensive Care Med 25:990–996
van Kaam AH, Dik WA, Haitsma JJ, De Jaegere A, Naber BA, van Aalderen WM, Kok JH, Lachmann B (2003) Application of the open-lung concept during positive-pressure ventilation reduces pulmonary inflammation in newborn piglets. Biol Neonate 83:273–280
van Kaam AH, de Jaegere A, Haitsma JJ, Van Aalderen WM, Kok JH, Lachmann B (2003) Positive pressure ventilation with the open lung concept optimizes gas exchange and reduces ventilator-induced lung injury in newborn piglets. Pediatr Res 53:245–253
Vazquez de Anda GF, Gommers D, Verbrugge SJ, De Jaegere A, Lachmann B (2000) Mechanical ventilation with high positive end-expiratory pressure and small driving pressure amplitude is as effective as high-frequency oscillatory ventilation to preserve the function of exogenous surfactant in lung-lavaged rats. Crit Care Med 28:2921–2925
van Kaam AH, Haitsma JJ, Dik WA, Naber BA, Alblas EH, De Jaegere A, Kok JH, Lachmann B (2004) Response to exogenous surfactant is different during open lung and conventional ventilation. Crit Care Med 32:774–780
Hilgendorff A, Aslan E, Schaible T, Gortner L, Baehner T, Ebsen M, Kreuder J, Ruppert C, Guenther A, Reiss I (2008) Surfactant replacement and open lung concept—comparison of two treatment strategies in an experimental model of neonatal ARDS. BMC Pulm Med 8:10
Iles R, Edmunds AT (1997) Assessment of pulmonary function in resolving chronic lung disease of prematurity. Arch Dis Child Fetal Neonatal Ed 76:F113–F117
Tepper RS, Morgan WJ, Cota K, Taussig LM (1986) Expiratory flow limitation in infants with bronchopulmonary dysplasia. J Pediatr 109:1040–1046
Jackson JC, Truog WE, Standaert TA, Murphy JH, Juul SE, Chi EY, Hildebrandt J, Hodson WA (1994) Reduction in lung injury after combined surfactant and high-frequency ventilation. Am J Respir Crit Care Med 150:534–539
Imai Y, Nakagawa S, Ito Y, Kawano T, Slutsky AS, Miyasaka K (2001) Comparison of lung protection strategies using conventional and high-frequency oscillatory ventilation. J Appl Physiol 91:1836–1844
Mehta S, Lapinsky SE, Hallett DC, Merker D, Groll RJ, Cooper AB, MacDonald RJ, Stewart TE (2001) Prospective trial of high-frequency oscillation in adults with acute respiratory distress syndrome. Crit Care Med 29:1360–1369
Derdak S, Mehta S, Stewart TE, Smith T, Rogers M, Buchman TG, Carlin B, Lowson S, Granton J (2002) High-frequency oscillatory ventilation for acute respiratory distress syndrome in adults: a randomized, controlled trial. Am J Respir Crit Care Med 166:801–808
Fedora M, Klimovic M, Seda M, Dominik P, Nekvasil R (2000) Effect of early intervention of high-frequency oscillatory ventilation on the outcome in pediatric acute respiratory distress syndrome. Bratisl Lek Listy 101:8–13
Panda AK, Nag K, Harbottle RR, Rodriguez-Capote K, Veldhuizen RA, Petersen NO, Possmayer F (2004) Effect of acute lung injury on structure and function of pulmonary surfactant films. Am J Respir Cell Mol Biol 30:641–650
Laffey JG, Engelberts D, Duggan M, Veldhuizen R, Lewis JF, Kavanagh BP (2003) Carbon dioxide attenuates pulmonary impairment resulting from hyperventilation. Crit Care Med 31:2634–2640
Redline RW, Wilson-Costello D, Hack M (2002) Placental and other perinatal risk factors for chronic lung disease in very low birth weight infants. Pediatr Res 52:713–719
Marshall DD, Kotelchuck M, Young TE, Bose CL, Kruyer L, O’Shea TM (1999) Risk factors for chronic lung disease in the surfactant era: a North Carolina population-based study of very low birth weight infants. North Carolina Neonatologists Association. Pediatrics 104:1345–1350
Akram Khan M, Kuzma-O’Reilly B, Brodsky NL, Bhandari V (2006) Site-specific characteristics of infants developing bronchopulmonary dysplasia. J Perinatol 26:428–435
Tapia JL, Agost D, Alegria A, Standen J, Escobar M, Grandi C, Musante G, Zegarra J, Estay A, Ramirez R (2006) Bronchopulmonary dysplasia: incidence, risk factors and resource utilization in a population of South American very low birth weight infants. J Pediatr (Rio J) 82:15–20
Noori S, McCoy M, Friedlich P, Bright B, Gottipati V, Seri I, Sekar K (2009) Failure of ductus arteriosus closure is associated with increased mortality in preterm infants. Pediatrics 123:e138–e144
Kamper J, Feilberg Jorgensen N, Jonsbo F, Pedersen-Bjergaard L, Pryds O (2004) The Danish national study in infants with extremely low gestational age and birthweight (the ETFOL study): respiratory morbidity and outcome. Acta Paediatr 93:225–232
Stevens T, Blennow M, Soll R (2004) Early surfactant administration with brief ventilation vs selective surfactant and continued mechanical ventilation for preterm infants with or at risk for respiratory distress syndrome. Cochrane Database Syst Rev 3:CD003063
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Tissières, P., Myers, P., Beghetti, M. et al. Surfactant use based on the oxygenation response to lung recruitment during HFOV in VLBW infants. Intensive Care Med 36, 1164–1170 (2010). https://doi.org/10.1007/s00134-010-1838-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-010-1838-0